

 PDF
PDF ePub
ePub Citation
Citation Print
Print


A 48-year-old man had jaundice for three months. Investigations revealed bicytopenia [hemoglobin, 4.5 g/dL; platelet, 30,000/µL; white blood cell (WBC), 11,000/µL], unconjugated hyperbilirubinemia (3.4 mg/dL), and elevated hepatic transaminases (aspartate aminotransferase, 147 IU/L; alanine aminotransferase, 297 IU/L). The peripheral blood smear (PBS) revealed anisopoikilocytosis, macroovalocytes, polychromasia, nucleated red blood cells (RBCs), microspherocytes, and RBC agglutinates. The corrected reticulocyte count was 9.76%. The direct Coomb's test was positive (4+). The indirect Coombs' test showed panagglutination. Other laboratory investigations were unremarkable. Fibroscan revealed advanced fibrosis (2.0 KPa). For immune-mediated hemolysis, 50 mg of prednisolone once a day was started.
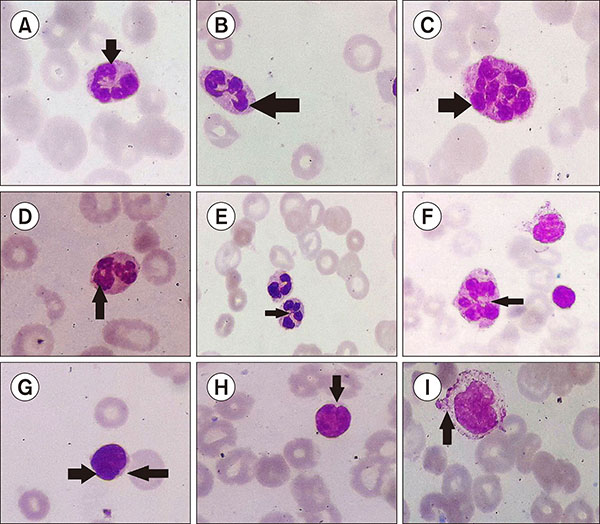
On day 5, PBS showed unremarkable WBC and platelet morphology. On day 15, granulocyte nuclei showed projections (A), clubbing, “claw” shapes (B), hypo- and hypersegmentation (C), “lobar” rings, with a single lobe forming a ring (D), and thin intersegmental filaments (E, F). Indented nuclei (“pseudocleave”) were seen in 10% of lymphocytes (G, H). Monocytes showed cytoplasmic fraying (I). Platelet morphology remained unremarkable. On day 21, RBC agglutination was absent. Nucleated RBCs, polychromasia, and granulocytic changes diminished. Hypersegmented neutrophils and intersegmental filaments persisted. Pseudocleaved lymphocytes decreased to 5%. On day 31, some microspherocytes remained. Pseudocleaved lymphocytes were replaced by activated lymphocytes. Granulocytes showed occasional lobar rings.
 XML Download
XML Download