

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The relationship between malignancy and myositis was first defined by Stertz in 1916 [1]. It is a type of paraneoplastic syndrome described as immune cross-reactivity between tumor and normal host tissues or secretion of functional peptides and hormones [2]. Dermatomyositis (DM) is a rare idiopathic inflammatory myopathy (IIM) which is characterized by typical cutaneous manifestations including heliotrope rash, Gottron's papules, cuticular changes including periungual telangiectasia, photodistributed erythema, poikiloderma and scaly alopecia [3]. Treatment strategy of DM includes corticosteroids, immunosuppressive agents and topical calcineurin inhibitors [4]. It has been reported that the frequency of malignancy in adults with DM varies from 6% to 60% [567]. Ovarian cancer (OC) accounts for approximately 13.3%–21.4% of the female DM population [8]. The onset of malignancy can be before, simultaneously with, or after the diagnosis of DM.
OC is the most lethal gynecologic malignancy and most cases of OC are diagnosed in the advanced stages. Cytoreductive surgery (CRS) and chemotherapy are standard initial treatment measures. According to the report of American Cancer Society (ACS), the 5-year survival for all stages of epithelial ovarian cancer (EOC) ranging from 35% in non-Hispanic blacks to 57% in Asians/Pacific Islanders [9]. There are only a few case reports of OC associated with DM due to the rare correlation. To analyze the clinical characteristics, prognosis and parallel clinical course of OC and DM, we conducted a retrospective study of 23 cases in our institution.
MATERIALS AND METHODS
Current study was approved by our Institutional Review Board (IRB), and the requirement for informed consent was waived for all patients (approval No. S-K727). We retrospectively analyzed the medical records of all patients who were diagnosed with OC and DM treated at Peking Union Medical College Hospital (PUMCH) between 2002 and 2017. Medical records were obtained from patients' admission, discharge and out-patient case history. OC was diagnosed pathologically and DM was diagnosed based on the diagnostic criteria of Bohan and Peter [10]. Four of the 5 criteria related to the muscle disease were as follow: progressive, proximal, symmetrical weakness, an increased concentration of muscle enzymes, an abnormal electromyogram, and an abnormal muscle biopsy sample. The fifth was compatible cutaneous disease [3]. The following information of patients was collected for analysis: age, menopausal status, pathological type of OC, tumor grade, tumor stage according to International Federation of Gynecology and Obstetrics (FIGO), time of DM diagnosis (negative number means DM diagnosed before OC, and positive number means DM diagnosed after OC, zero means two disease diagnosed simultaneously), serum cancer antigen 125 (CA 125) level (U/mL) and creatine kinase (CK) level (U/L) tested simultaneously with CA125, treatment, follow up and outcome. Follow up time was up to November 2018.
To reducing the confounding effects of covariates, we used propensity score matching (PSM) method in a 1:5 ratio to match patients who have concurrence of OC and DM to those diagnosed with OC alone. Six covariates, age, menopause status, tumor pathological type, tumor grade, FIGO stage, and gross residual disease were taken into account at the start of follow up [11].
Statistical analysis was carried out using SPSS software version 19 (IBM Company, Armonk, NY, USA). The χ2 test was used for categorical variables. Kaplan-Meier survival analysis and log-rank test were used to describe overall survival (OS) and progression-free survival (PFS) difference between groups. Multivariate analysis using Cox proportional hazard regression model to determine independent predictors to survival. The correlation between serum CA 125 and CK was measured by Pearson correlation scatter plot and Pearson's r. The closer the r value is to 1, the greater the correlation is between CA 125 and CK. Statistical difference was considered significant when p value was <0.05.
RESULTS
Between 2002 and 2017, 2882 patients were diagnosed with OC in total, of which 23 (0.8%) patients had the concurrence of DM in PUMCH. The clinicopathologic characteristics are presented in Table 1 (DM group). The mean age of patients was 53.4 years (range, 40–74 years). Of those 23 patients, 18 (78.3%) were in their menopause and 5 (21.7%) were not. Pathologically, the tumor was all serous papillary carcinoma except for 2 patients who had endometrioid carcinoma and clear cell carcinoma, respectively. Nineteen patients had tumor grade 3 of tumor differentiation and 4 patients had grade 2. Eleven patients were diagnosed with dermatomyositis before OC, and 12 patients were diagnosed with dermatomyositis after or simultaneous with OC. Nineteen patients were diagnosed with FIGO stage III OC, and 4 patients were diagnosed with FIGO stage IV OC. As for diagnosis of dermatomyositis, there were 9 patients who complained of distal muscle weakness, 8 patients had heliotropic rash, 4 patients had myalgia, and 2 patients had dysphagia. All patients underwent CRS and platinum-paclitaxel combination chemotherapy in primary treatment.
Table 1
Characteristics of patients diagnosed with OC with or without DM after PSM (n=138)
The median follow-up time was 47.9 months (range, 12–125 months) in patients who diagnosed with OC and dermatomyositis. At the time of review, 3 patients were alive and without evidence of disease, and 14 patients (60.9%) showed a relapse of disease, and 4 patients had uncontrolled disease after primary treatment. Six patients accepted second cytoreductive surgery (SCRS) in total. However, there were 11 (47.83%) patients died of disease progression ultimately.
One hundred and fifteen patients who diagnosed with OC alone (No DM group) were matched to 23 patients who have the concurrence of OC and dermatomyositis (DM group) by using PSM method at a ratio of 1:5. Baseline tumor characteristics were comparable between the 2 groups were shown in Table 1. The 5-year OS (71.6% vs. 51.8%, p=0.020) and 5-year PFS (30.5% vs. 0%, p=0.018) were poorer in dermatomyositis group. Survival outcomes are presented in Fig. 1A and B.
Fig. 1
(A) OS of patients who have the concurrence of OC and DM vs. OC alone (p=0.020). (B) PFS of patients who have the concurrence of OC and DM vs. OC alone (p=0.018). (C) OS of patients diagnosed with DM before OC vs. DM after or simultaneously with OC (p=0.021).
DM, dermatomyositis; OC, ovarian cancer.
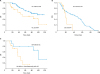
For 23 patients who have the concurrence of OC and dermatomyositis, no significant differences were noted in the OS based on patient age, menopause status, pathology type or tumor grade, except for the time between OC and dermatomyositis diagnosis. Patients diagnosed with dermatomyositis after or simultaneously with OC had a significantly poor prognosis than those diagnosed with dermatomyositis before OC (p=0.021). Survival outcomes are shown in Fig. 1C. While in multivariable analysis, none of these clinical factors was associated with poorer OS. The results are shown in Table 2.
Table 2
Multivariate analysis of factors related to survival in patients have concurrence of OC and DM

The details of patients have the concurrence of OC and dermatomyositis are depicted in Table 3. Twenty-one patients (91.3%) diagnosed with dermatomyositis within 3 years before or after OC diagnosis. All patients had elevated CA 125 levels at the time of diagnosis of OC, and the mean level of CA 125 was 1,261.5 U/L (range, 36.6–9,715 U/L). There were 16 patients who took the test for serum CA 125 and CK level at the same time during therapeutic process, and correlation between serum CA 125 and CK level was observed in 12 of them. Pearson correlation scatter plot and Pearson's r of these 12 patients are shown in Fig. 2.
Table 3
Details of patients with the concurrence of OC and DM
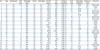
CA 125, cancer antigen 125; CCC, clear cell carcinoma; CK, creatine kinase; CRS, cytoreductive surgery; CT, chemotherapy; DM, dermatomyositis; EC, endometrioid carcinoma; FIGO, International Federation of Gynecology and Obstetrics; NA, not available; NED, no evidence of disease; OC, ovarian cancer; SCRS, secondary cytoreductive surgery; SPC, serous papillary carcinoma; TOD, time of dermatomyositis diagnosis (negative number means dermatomyositis diagnosed before ovarian cancer, and positive number means dermatomyositis diagnosed after ovarian cancer, zero means 2 disease diagnosed simultaneously); TOR, time of recurrence; UD, Uncontrolled disease.
*CA 125, Preoperative test level (normal range, 0–35 U/mL); †CK, Tested simultaneously with CA 125 (normal range, 24–170 U/L).

DISCUSSION
Paraneoplastic syndrome occurs in 1%–8% of patients with malignancy [212], and dermatomyositis comprises 10% of it [13]. Bohan and Peter [10] suggested a set of criteria of diagnosis and classification of dermatomyositis and polymyositis. The association between cancer and dermatomyositis has been extensively reported. A population-based study estimated the standardized incidence ratios (SIRs) for malignancy compared with general population at 3.8–7.7 for dermatomyositis [14]. The malignancies most strongly associated with dermatomyositis are ovarian, lung, gastric, colorectal, and pancreatic cancers, as well as non-Hodgkin's lymphoma [15]. In Asian populations, nasopharyngeal and lung cancers were found to be the most common malignancies associated with dermatomyositis [16]. Although the pathogenesis of cancer associated with dermatomyositis still unclear, there are some theories that explain this phenomenon: 1) tumor may produce bioactive factors that directly or indirectly cause inflammation or are resistant to muscle/skin immune response; 2) cross-reaction with muscle/skin antigens elicited by antitumoral immune reaction which becomes an autoimmune syndrome; 3) exposing to environmental hazards such as viruses, drugs, or chemicals, which are carcinogenic and trigger immune reactions resulting in compromised immune systems; and 4) neoplasms that are secondary to the cytotoxic effect of agents used in therapeutic regimens to treat dermatomyositis patients [171819]. Classic reviews have emphasized that immune activation and overexpression of proteins by apoptotic cells after exposure to environmental risk factors can result in antigen presentation, autoreactive T cell propagation and autoantibody production [20]. Consequently, this results in tissue and a release of autoantigens which amplifies the autoimmune response and sustains disease progression [21]. In the study of Livia et al. [22], they proved that myositis autoantigen expression markedly increased in cancer associated with autoimmune myositis, but not in their related normal tissue, which demonstrating that tumor cells and undifferentiated myoblasts are antigenically similar.
In this study, PSM method was used to match control group. After analyzing, patients who have concurrence of OC and dermatomyositis showed poorer outcome in 5-year OS and PFS comparing to those diagnosed with OC alone. Similarly, Hemminki et al. [23] analyzed risk and survival in close to 200,000 patients diagnosed with female cancers and autoimmune diseases. They deemed that the survival disadvantage in patients who diagnosed with cancer is related to chronic, severe disease, autoimmune disease, and other co-morbidities. The possible explanation is that cross-reaction between tumor antigens and autoantigens enhances patients' autoimmune response. Immunosuppressive drugs for the treatment of dermatomyositis cause tumor progression which releases more tumor antigens. A key question is whether it is the immune disease itself that increases the risk of malignance, or its treatment. The study conducted by Hojo et al. [24] has shown that cyclosporin A promotes cancer progression by direct cellar mechanism inducing morphological alternations in tumor cells.
The time between OC and dermatomyositis diagnosis is significant through univariable analysis but not in multivariable analysis in patients who have the concurrence of OC and dermatomyositis. This inconsistent results possible due to low test efficiency of small sample size of population. Our data show that there were 21 patients (91.3%) diagnosed with dermatomyositis within 3 years before or after OC diagnosis in this study. According to the study of Chen et al. [25], the risk is still apparent 5 years after diagnosis of IIM, and this may be related to immune environment disturbance. However, a Danish study suggested that the risk of malignancy was highest during the first year after diagnosis, and returned to baseline levels in the third year [26]. Namely, when the high-risk period pass, regarding patients who were diagnosed with dermatomyositis, good response to immunotherapy to dermatomyositis was seen in most patients, and cancer risk in patients actually decreased with time [25]. A lower risk of cancer has been reported in patients who previously received cytotoxic treatment for myopathies [27]. Similarly, Cibere et al. [28] and Sorianello et al. [29] both pointed out that immunosuppressant drugs did not promote tumor development in their studies. In addition, tumors can secrete one or more factors that counteract immunosuppressant drugs.
One of intriguing phenomena is that 9 patients who have severer symptoms of skin lesion, myalgia, myasthenia, and dysphagia when diagnosed with OC. The symptoms of dermatomyositis improved rapidly and CK levels decreased dramatically after underwent the CRS. Both OC and dermatomyositis reached clinical remission soon after chemotherapy and corticosteroids treatment. During the follow-up, the existing results showed that the increase level of CA 125 was accompanied by the increase level of CK when tumor recurrence. After evaluating the CK and CA 125 level, a correlation between serum CA 125 and CK level was observed in 12 patients based on the Pearson correlation test. The severity of myositis frequently correlates with enzyme concentrations in the blood and degree of weakness, and CK is the most sensitive and specific indicator of dermatomyositis [30]. Similarly, the serum level of CA 125 antigen has been documented as a useful marker for diagnosis, observing the therapeutic effect, evaluating the recurrence and prognosis of disease in individual patients with EOC [31]. In a way, the level of CK can represent the severity of dermatomyositis, and the level of CA 125 can represent the clinical course of OC. Our results demonstrated that OC and dermatomyositis had a parallel clinical course in these patients.
The limitations of retrospective studies are well known. The sample size in this study was small because of the low incidence of this concurrence, and small sample size may lead to the bias and low teat efficiency. In addition, PSM analysis might be potentially limited by biases related to unmeasured and hidden covariates. Despite limitations, our study retrospectively analyzed the characteristics and prognosis of the patients who were diagnosed with OC and dermatomyositis in a single institution, and most of the patients had long-term follow-up data and survival outcomes. In addition, a correlation between serum CA 125 and CK level was found which suggests a parallel clinical course in patients.
In conclusion, the concurrence of OC and dermatomyositis as a paraneoplastic syndrome is rare and has a poor prognosis. The risk for patients diagnosed with dermatomyositis is highest within 3 years before or after OC diagnosis. A correlation and a parallel clinical course exist in these 2 diseases.
 XML Download
XML Download