

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Ovarian cancer is the most lethal gynecological malignancy. Approximately 295,000 new cases are diagnosed, and 185,000 deaths result from the disease annually worldwide [1]. Ovarian cancer is heterogeneous in terms of its histologic background and is now classified into at least 5 subtypes: the high grade serous, low grade serous, endometrioid, clear cell, and mucinous types, with carcinogenesis and risk factors varying between the subtypes. High grade serous carcinoma (HGSC) is the most common subtype, accounting for 75% of cases and the majority of mortalities [234].
Research in the past 2 decades has identified the fallopian tube epithelium rather than the ovarian surface epithelium as the site of HGSC origin [56]. Although the pathomechanism underlying early stage HGSC carcinogenesis is not fully understood [67], the current hypothesis holds that the p53 signature, defined as the accumulation of p53-positive cells in the fallopian tube with near-normal morphology, represents an early stage in HGSC genesis; the final stage in the fallopian epithelium is serous tubal intraepithelial carcinoma (STIC), and the intermediate proliferative status, also called serous tubal epithelial proliferation/lesions of uncertain significance, occurs between the early and final stages described above [5].
Several studies investigating the risk factors of HGSC [489] or type II ovarian cancer [10] showed that oral contraceptives (OC) and parity inversely correlated with the incidence of HGSC. OC and pregnancy suppress ovulation and change hormonal status. These changes are thought to protect the ovarian epithelium from carcinogenesis [11]. However, the effect of these changes on the fallopian tubes has not been examined well, and little is known about the association between OC or pregnancy and the HGSC precursors in the fallopian epithelium. Clarifying this association may help explicate the pathomechanism underlying HGSC.
In this prospective observational study, we explored the relationship between the incidence of HGSC precursors and patient characteristics in benign gynecological patients and pregnant women by focusing on the effects of pregnancy.
MATERIALS AND METHODS
1. Study population
We prospectively examined consecutive cases in which the bilateral fallopian tubes were removed during benign gynecological or obstetric surgery at Tokyo Metropolitan Tama Medical Center between April 2017 and August 2018. Obstetric surgery included surgical sterilizations during a cesarean section (CS) and postpartum hysterectomies after 35 weeks. Gynecological surgery was defined as all types of surgery for benign gynecologic diseases which included the bilateral salpingectomy as part of the procedure. Patients whose bilateral fimbriae were able to be examined were enrolled. Patients with a current or past history of borderline or malignant gynecological tumors except cervical intraepithelial neoplasms were excluded. The patients' genetic risk for ovarian cancer was assessed using a referral screening tool [12]. Other clinical information was collected from the medical records.
2. Histological assessment
All fallopian tubes were submitted for a histological analysis using the Sectioning and Extensively Examining the Fimbriated End (SEE-FIM) Protocol. All fimbriae were sectioned into 4 longitudinal specimens, and the isthmuses and ampullae were cut transversely at 2–3 mm intervals [13]. The median number of sections of one fallopian tube was 13 (range, 8–19). All the sections were examined by hematoxylin and eosin staining and immunohistochemistry.
3. Immunohistochemistry
Immunohistochemical analysis was done with the paraffin-embedded sections using p53 (mouse monoclonal, DO-7, ready-to-use; Dako, Glostrup, Denmark), Ki-67 (rabbit monoclonal, SP6, ready-to-use; Nichirei Bioscience, Tokyo, Japan), and PAX8 (mouse monoclonal, ready-to-use; Roche, Basel, Switzerland) antibodies with the BenchMark XT automated slide processing system (Roche) [14].
The diagnostic criteria for the precursors in this study were as follows: a p53 signature, defined as the presence of at least 12 consecutive p53-positive secretory cells with normal morphology and less than 10% positive nuclear Ki-67 expression; a serous tubal epithelial proliferation/lesion of uncertain significance, defined as the presence of 12 consecutive p53-positive secretory cells with mild cytological atypia and/or 10%–50% positive nuclear Ki-67 expression; and STIC, defined as the presence of 12 consecutive p53-positive secretory cells with moderate to severe cytological atypia and/or more than 50% positive nuclear Ki-67 expression [515]. Cells with PAX8-positive nuclei were considered to be secretory cells [16]. A pathologist and a gynecologist (T.K. and T.I.) independently evaluated the pathological findings. Whenever the assessments disagreed, the diagnosis was determined by discussion.
4. Statistical analysis
Data were analyzed with IBM SPSS version 23.0 (IBM, Armonk, NY, USA). For comparison, the following tests were used: the Shapiro-Wilk test for distribution, Student t-test for normally distributed variables, Mann-Whitney U test for non-normally distributed variables, Fisher's exact test and the χ2 test for categorical variables, and multivariate logistic regression analysis for regression analysis. The p value of <0.05 was considered statistically significant.
5. Ethical approval
This study was approved by the Institutional Review Board at Tokyo Metropolitan Tama Medical Center and was registered with the University Hospital Medical Information Network (registration number: UMIN000027001). We obtained written informed consent from all the patients before enrollment.
RESULTS
The patient characteristics are shown in Table 1. Of the 113 patients enrolled, 67 were gynecological and 46 were obstetric patients. The referral screening tool was negative for 112 patients (99%). Therefore, most of the patients were considered at low risk for ovarian cancer.
Table 1
Clinical characteristics (n=113)

Non-normally distributed variables are expressed as the median (range). Categorical variables are expressed as number (%). BMI and current smoking status in obstetric patients indicate patient's status before current pregnancy. Parity includes current delivery in obstetric patients.
BMI, body mass index.
In the histological examination, the p53 signature was identified in 21 patients (19%). Serous tubal epithelial proliferation/lesions of uncertain significance and STIC were not identified. Of the 21 patients with the p53 signature, 18 (86%) had 1 lesion and 3 (14%) had 2 lesions with the p53 signature. Of 3 patients who had 2 lesions, 1 had the p53 signature in her bilateral fallopian tubes. Of 24 p53 signatures, 21 (88%) were in the fimbriae, and 3 (12%) were in the ampullae.
The relationship between the p53 signature and the clinical characteristics is shown in Table 2. The p53 signature-positive group had a significantly higher age and more postmenopausal women than the p53 signature-negative group. Parous women were significantly fewer in the p53 signature-positive group (53% vs. 86%, p=0.002), as were obstetric patients (10% vs. 47%, p=0.001). Current pregnancy was also associated with a significantly lower incidence of the p53 signature after multivariate adjustment for age, body mass index (BMI), and menopausal status (odds ratio [OR]=0.112; 95% confidence interval [CI]=0.017–0.731; p=0.022); however, age, BMI, and menopausal status were not associated with the incidence of the p53 signature (Table 3).
Table 2
Patient characteristics of p53 signature-positive and negative groups
Non-normally distributed variables are expressed as the median (range). Normally distributed variables are expressed as the mean±SD. Categorical variables are expressed as number (%). BMI and current smoking status in obstetric patients indicate patient's status before current pregnancy. Parity includes current delivery in obstetric patients. Total percentage of parity in p53-positive group was not 100% due to rounding to the first decimal place.
BMI, body mass index.
*Mann-Whitney U test; †Student's t-test; ‡Fisher's exact test.
Table 3
Multivariate analysis of factors associated with p53 signature positivity

OR are shown with the 95% confidence interval. Factors for multivariate analysis included age, BMI, menopausal status, and pregnancy. Parity was not included in multivariate analysis because it was considered an intermediate variable between pregnancy and p53 signature positivity.
OR, odds ratio; BMI, body mass index.
*Logistic regression analysis.
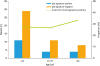
To investigate the effect of characteristics other than pregnancy, we assessed the relationship between the p53 signature and clinical characteristics in gynecological patients (Table 4). As in the results for all the patients, parous women were significantly fewer in the p53 signature-positive group than in the p53 signature-negative group after excluding obstetric patients (47% vs. 73%, p=0.047), and the difference was still significant after multivariate adjustment (OR=0.252; 95% CI=0.069–0.911; p=0.036); however, other clinical characteristics did not differ significantly between the p53 signature-positive and negative groups. The incidence of the p53 signature in gynecological patients was similar across all age groups (p=0.931) (Fig. 1).
Table 4
Relationship between p53 signature and clinical characteristics in gynecological patients

Categorical variables are expressed as number (%). OR are shown with the 95% confidence interval. Non-normally distributed variables are expressed as the median (range). Normally distributed variables are expressed as the mean±SD. Factors for multivariate analysis included age, BMI, menopausal status, and parity.
OR, odds ratio; BMI, body mass index.
*Mann-Whitney U test; †Student t-test; ‡Chi-square test; §Logistic regression analysis.
DISCUSSION
In this prospective study, we showed that among patients at low risk for HGSC, parous women had a significantly lower incidence of the p53 signature than nulliparae. Furthermore, pregnant women had a significantly lower incidence of the p53 signature than non-pregnant women.
Among patients at low risk for HGSC, parous women had a significantly lower incidence of the p53 signature. Although the p53 signature was more frequently encountered in patients with STIC, previous studies have demonstrated a 20%–50% occurrence rate among patients without HGSC, STIC or a hereditary risk for HGCS [515171819]. The incidence of the p53 signature in gynecological patients (28%) was similar to that reported by previous studies. A previous study reported that increased parity inversely correlated with the incidence of the p53 signature in women receiving a prophylactic salpingo-oophorectomy for a hereditary mutation in the breast cancer susceptibility gene (BRCA) [20]. This study found a similar decrease in the p53 signature in parous women among patients at low risk for HGCS.
Pregnant women also presented a significantly lower incidence of the p53 signature, which was still significant on multivariable analysis. The difference was clearer between pregnant and non-pregnant women than between parous women and nulliparae, suggesting that pregnancy itself may be the cause of the decreased incidence in parous women. Although the differences in age and other characteristics between the gynecological and obstetric patients require careful scrutiny, analysis of the gynecological patients in both the present and previous studies showed that age had no effect on the incidence of the p53 signature in patients at either low or high-risk for HGSC [1920] or on the incidence of p53-positive cells in the fallopian epithelium in patients at low-risk for HGSC [21].
The developmental mechanism of the p53 signature is still unknown. The presence of p53 mutations and DNA damage associated with the p53 signature [17] suggests that the p53 signature may arise from some genotoxic insult [5]. One possible cause of such a genotoxic insult is the follicular fluid to which the fimbriae are exposed at ovulation. A previous study showed that follicular fluid caused DNA damage and p53 accumulation in fallopian epithelial cells in vitro [22]. Anovulation during pregnancy may decrease the incidence of DNA damage in the fallopian tube epithelium and decrease the incidence of the p53 signature in parous women and pregnant women. However, a previous study reported that other factors related to the menstruation (e.g., age at menarche, age at menopause and duration of OC use) were not associated with positivity for the p53 signature [20]. Anovulation may thus be insufficient to explain the decrease.
Another possible cause is the increase in progesterone during pregnancy. A previous study showed that progesterone induced necroptosis in p53-deficient tubal epithelial cells [23]. Continuous exposure to a 10-fold increase in progesterone during pregnancy [11] may decrease the incidence of the p53 signature. This progesterone hypothesis may also explain the absence of any decrease in the incidence of the p53 signature in postmenopausal women since the expression of progesterone receptor A and apoptotic cells in the fallopian tubes decrease in postmenopausal women [24]. Epidemiologically, the risk-reducing effect of parity on HGSC is limited to middle age and diminishes after the middle of the sixth decade of life [4], and later age at last birth is associated with a decreased incidence of ovarian cancer [925]. These results also support the hypothesis that temporary clearance of p53-deficient tubal epithelial cells during pregnancy may decrease the risk of HGSC.
The fallopian tubes removed during CS may provide new information which may help clarify the risk-reducing mechanism of HGSC. Several recommendations for the use of the bilateral salpingectomy instead of tubal ligation as a method of surgical sterilization have been published during the past few years [26272829]. Recent studies showed that the bilateral salpingectomy was as safe as tubal ligation even during CS [30313233], and the procedure is increasingly being preferred for surgical sterilization during CS. More fallopian tubes collected during CS may allow us to examine the mechanism behind the decreased incidence of HGSC in parous women.
This study has several strengths and limitations. Its strengths lie in its prospective design, inclusion of consecutive cases, and use of the SEE-FIM Protocol for all specimens. One limitation of this study is the small sample size with varying characteristics of the gynecological and obstetric patients. Although our data and those of previous studies suggested that differences in age may not affect the results, further investigation using a larger matched control is needed to clarify the effects of pregnancy. The lack of information about OC use is another limitation. The proportion of women using OC in Japan is low [34], and no association was observed between the incidence of the p53 signature and OC use in a previous study [20]. Therefore, we consider the influence of OC use on the results to be negligible. Finally, although the p53 signature is considered to be an early phase of serous carcinogenesis, the pathomechanism linking the p53 signature and HGSC has not been clarified [56]. Therefore, we cannot conclude that the decreased incidence of the p53 signature in this study leads to a reduced HGSC risk. Further investigation of serous carcinogenesis is needed to clarify the relationship between the decreased incidence of the p53 signature and HGSC risk.
In conclusion, the incidence of the p53 signature was significantly lower in parous women and pregnant women. This decreased incidence of early phase serous carcinogenesis may be one of the possible mechanisms underlying HGSC risk reduction among parous women. Further investigation, including an analysis of other possible effects of pregnancy besides the p53 signature on the serous carcinogenetic process, is needed to clarify the implications of our findings.
 XML Download
XML Download