

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Progestin therapy is a popular treatment options for preserving fertility in patients with atypical endometrial hyperplasia (AEH) and endometrial cancer (EC). Guidelines of the National Comprehensive Cancer Network and the European Society of Gynecological Oncology Task Force for fertility-sparing treatment recommend progestin therapy for patients with AEH and EC who wish to conceive [12]. However, results of 3 meta-analyses revealed a high remission rate, as well as an association with a high rate of relapse [345], which is the most problematic feature of this therapy.
Metformin is a biguanide that is widely used worldwide for the treatment of type 2 diabetes mellitus. Several recent epidemiological studies have revealed that metformin reduces the incidence of cancer and cancer-related mortality in diabetes patients [67]. Metformin induces anti-neoplastic effects on various cancer cell lines through the suppression of mitogen-activated protein kinase (MAPK) and inhibits the mammalian target of rapamycin (mTOR) pathway [89]. Moreover, metformin has been associated with improved relapse-free survival (RFS) and overall survival in EC patients with diabetes [1011].
Based on this information, we had previously conducted a phase II study of medroxyprogesterone acetate (MPA) plus metformin as a fertility-sparing treatment for AEH and EC patients and reported that metformin had inhibited disease relapse after remission [12]. However, the relapse rate was analyzed only for the patients who had achieved remission by 9 months, with a median follow-up period of only 38 months.
Here, we retrospectively analyzed long-term outcomes of MPA plus metformin as a fertility-sparing treatment for AEH and EC patients. We believe this is the largest-scale evaluation to-date of metformin's efficacy in treating EC patients.
MATERIALS AND METHODS
1. Patients
This retrospective study was approved by the Institutional Review Board (IRB) of Chiba University (IRB No. 2871). From July 2009 to December 2017, we treated 63 patients with AEH and EC by administering MPA plus metformin as a fertility-sparing treatment at Chiba University Hospital (Chiba, Japan). Among the 63 patients, 36 were included in our previously reported phase II study [12]. However, the former study analyzed the outcome of only 29 patients who had achieved remission by 9 months. Here, we retrospectively reanalyzed all the patients who were enrolled in the phase II study as well as additional patients who were treated after the conclusion of that study.
The eligibility criteria for administration of MPA plus metformin as a fertility-sparing treatment were as follows: 1) AEH or well-differentiated adenocarcinoma grade 1 (stage IA disease, as determined by the International Federation of Gynecology and Obstetrics guidelines); 2) myometrial invasion ruled out by magnetic resonance imaging (MRI); 3) strong desire and consent for fertility-sparing treatment; and 4) 40 years or less of age in principle. Exclusion criteria were as follows: 1) Suspicion of myometrial invasion on pelvic ultrasound or MRI in patients with EC; 2) Suspicion of lymph node metastases, ovarian tumor, or other metastasis on ultrasound, MRI, or computed tomography; 3) Diabetes mellitus requiring insulin injections; 4) Abnormalities in blood coagulation tests and/or history of thromboembolism; 5) Moderate to severe kidney damage or dialysis; and 6) Other standard exclusion criteria such as inadequate liver/cardiac function.
All patients, except those already diagnosed as having diabetes mellitus, underwent a 75 g oral glucose tolerance test (OGTT) to assess insulin resistance (IR). IR was defined as a homeostasis model assessment of IR (HOMA-IR) score of ≥2.5. The HOMA-IR was calculated according to the following formula: fasting glucose (mg/dL)×fasting insulin (U/mL)/405. Data regarding age, gravidity, parity, infertility, obesity (defined as body mass index [BMI] ≥25 kg/m2), diabetes, and polycystic ovary syndrome (PCOS) were obtained. PCOS was diagnosed according to the Rotterdam 2003 criteria. After the phase II clinical trial concluded, we prescribed metformin to the patients with abnormal glucose metabolism (AGM), and to those who met the criteria for PCOS.
We treated the patients who desired fertility preservation with MPA alone before 2009. From 2009 onward, we started administering metformin in combination with the MPA; however, the patients who were ineligible for metformin treatment were treated with MPA alone. Twenty-three patients with EC who were treated with MPA alone as a fertility-sparing treatment at Chiba University Hospital (Chiba, Japan) from 1996 to 2017 were set as historical controls with whom we compared EC patients of the current study.
2. Treatment
The patients received a daily oral dose of 400 mg MPA until remission. If patients do not progress, MPA treatment should continue for at least 6 months. If patients have not achieved remission at 6 months, we allow an additional 6 months of MPA treatment under careful management. After achieving remission, maintenance therapy with low-dose estrogen/progestin (EP) (1 cycle consisted of continuous daily administration of low-dose EP [1 mg norethisterone and 0.035 mg ethinylestradiol] for 21 days and interrupted administration for 7 days) or cyclic lower-dose progestin (daily dose of medroxyprogesterone [15 mg per day] was continued for 14 days and administered interrupted for 14 days). Metformin (initial dose, 750 mg/day; increased weekly by 750 mg up to 2,250 mg/day if no adverse effects occurred) was administered concurrently with MPA from the initiation of treatment. Metformin therapy was continued after MPA administration until either conception or disease recurrence.
3. Evaluation of response to progestin treatment and management after remission
The response to progestin treatment was assessed histologically by using endometrial specimens obtained through dilatation-curettage biopsy performed under anesthesia each 2–3 months until remission. The pathological diagnoses of the endometrial samples were reviewed by 2 independent pathologists. Complete response (CR) was defined as remission with the absence of evidence of hyperplasia or carcinoma. Partial response was defined as the presence of a hormone effect without evidence of progression. After remission, all patients were followed up every 3 months with pelvic examinations, tumor markers, imaging studies with transvaginal ultrasound, and histological assessment of specimens obtained via office-based endometrial biopsy. If a patient who achieved remission wanted to conceive immediately, fertility treatment was initiated after 6 cycles of maintenance treatment. Otherwise, a low-dose EP or cyclic lower-dose progestin was prescribed until the patient wished to conceive.
4. Statistical analysis
Variations between the 2 unpaired groups were analyzed using the Mann-Whitney U test. Frequency distributions were compared by using the χ2 test, unless the expected frequency was <5, in which case, the Fisher's exact test was employed. RFS was estimated by using the Kaplan-Meier method. Kaplan-Meier curves were generated to display event distributions over time. Comparisons between paired values were made by using the Wilcoxon signed-rank test. Logistic regression analysis was used to estimate the risk of relapse associated with IR, BMI, and clinical status of patients. All comparisons were planned, and the tests were 2-sided. A p-value of <0.05 was considered significant. All statistical analyses were carried out using SPSS software version 23 (IBM Corp., Armonk, NY, USA).
RESULTS
1. Patient characteristics
The patients' characteristics, including their metabolic profiles, are shown in Table 1. Forty-eight (76%) of the 63 patients exceeded BMIs of 25 kg/m2. Of the total patients, 30 (48%) showed impaired glucose tolerance, and 44 (70%) had IR. The mean fasting glucose level was 138 U/mL (95% confidence interval [CI]=124–151). The mean fasting insulin level was 149 U/mL (95% CI=109–189). The mean glucose level at 2 hours after OGTT was 138 U/mL (95% CI=124–151). The mean insulin level at 2 hours after OGTT was 149 U/mL (95% CI=109–189). Thirty-eight of the 42 married patients were nulliparous; only 4 were parous.
Table 1
Characteristics of patients who underwent fertility-sparing treatment

Data are presented as median (range) or number (%).
AEH, atypical endometrial hyperplasia; AGM, abnormal glucose metabolism; BMI, body mass index; HOMA-IR, homeostasis model assessment of insulin resistance; OGTT, oral glucose tolerance test; PCOS, polycystic ovary syndrome.
![]()
2. Response and RFS
Of the 63 patients, 61 (97%) achieved CR within 18 months, and the median time interval to CR was 6 months (range, 3–18 months). Two patients (3%) with EC that had progressed within the first 3 months underwent hysterectomies. Outcomes of these 2 patients were described previously [12]. The number of patients who had achieved remission within 6, 8–9 and 12 months were 38 (60%), 53 (84%), and 57 (90%), respectively. The CR rate of EC was 95% (40 of 42 patients). The CR rate of AEH was 100% (21 of 21 patients). Eight (13.1%) of the 61 patients who had achieved CR relapsed during a median follow-up period of 57 months (range, 13–88 months) from initial treatment (Fig. 1). The median interval to recurrence was 17 months (range, 15–67 months) after MPA treatment. RFS in all patients at 5 years was 84.8%. For 2 of the 8 patients who had recurrence at 18 and 61 months after MPA treatment opted to undergo hysterectomies. The patient who had recurrence at 61 months after MPA treatment was 48 years old at time of recurrence and had discontinued metformin 4 years prior. The other 6 patients consented to MPA retreatment because of a strong desire to maintain fertility, and 5 of them achieved remission again. However, 1 patient who had not reached remission by retreatment, underwent a hysterectomy. Therefore, of the 63 patients who initially tried fertility-sparing treatment with MPA plus metformin, 58 patients (92%) achieved durable CR with uterine preservation for a median duration of 57 months.
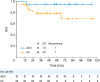 | Fig. 1RFS in 63 patients who underwent fertility-sparing treatment with metformin plus medroxyprogesterone acetate. RFS was measured from the date of initial treatment until the date of event occurrence, defined as recurrence, progression, or not reaching remission.AEH, atypical endometrial hyperplasia; CR, complete response; EC, endometrial cancer; RFS, relapse-free survival.
|
3. Analysis of factors that affected response and relapse
Analysis of factors that affected response and relapse was performed on the data from 63 patients who had been treated by MPA plus metformin. Our results showed that patients with BMI ≥25 kg/m2 had significantly better prognoses than did those with BMI <25 kg/m2 (Fig. 2A). Upon univariate analysis, patients with BMI ≥25 kg/m2 had significantly better prognoses than did those with BMI <25 kg/m2 (odds ratio [OR]=0.19; 95% CI=0.05–0.66; p=0.009) (Table 2). AGM, IR, and infertility treatment did not significantly affect prognosis (Fig. 2B-D).
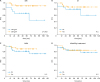 | Fig. 2Relapse-free survival of 63 patients who underwent fertility-sparing treatment with metformin plus medroxyprogesterone acetate, with respect to BMI (A), status of IR (B), AGM (C), and infertility treatment (D).AGM, abnormal glucose metabolism; BMI, body mass index; IR, insulin resistance; N.S., not significant.
|
Table 2
Univariate analysis to predict relapse after fertility-sparing treatment
AEH, atypical endometrial hyperplasia; AGM, abnormal glucose metabolism; BMI, body mass index; CI, confidence interval; EC, endometrial cancer; HR, hazard ratio; IR, insulin resistance; N.S., not significant; PCOS, polycystic ovary syndrome.
![]()
4. Pregnancy outcomes
Of the 61 patients who achieved remission, 31 desired to conceive (Supplementary Table 1). Mean age of the infertile patients was 35 years (range, 26–44 years). All patients who desired to conceive underwent in vitro fertilization and embryo transfer immediately after 6 cycles of maintenance therapy with a lower-dose monophasic agent. Nineteen patients had 24 conceptions during the follow-up period, and, eventually, 14 patients had 17 live births. The overall pregnancy rate and live birth rate per patient were 61% (19/31) and 45% (14/31), respectively (Supplementary Fig. 1). Moreover, 83% of pregnancies occurred within 12 months. Only 1 twin pregnancy occurred. In addition, 2 women achieved 2 pregnancies. Three patients, 2 of whom had a history of myomectomies, experienced placental adhesions following caesarean sections. Moreover, one of these underwent a subsequent hysterectomy. The other 17 patients did not experience any obstetric complications related to the fertility-sparing treatment.
5. Adverse events
No severe toxicities were observed. Most instances of diarrhea and nausea occurred at the metformin dose of 2,250 mg/day; however, these symptoms disappeared after the dose was reduced to 1,500 mg. Grades 1 and 2 diarrhea occurred in 6 and 3 patients, respectively. Grades 1 and 2 nausea occurred in 6 and 4 patients, respectively. While metformin administration was interrupted in 2 patients because of grade 2 nausea (but was resumed at a reduced dose after childbirth), it was discontinued immediately in 2 patients because of grade 2 nausea.
Abnormal blood test results, including liver function and coagulation tests, were not reported during MPA treatment. There were no cases of thrombosis or treatment-related death. Five patients presented with liver dysfunction after MPA treatment. Three of these patients were diagnosed with a fatty liver and adverse events associated with the low-dose EP pill were identified in 2 patients.
No weight gain (grade ≤1) occurred in any patients when MPA was administered with metformin.
6. Response for metabolic profiles
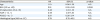
We evaluated the effect of metformin on the pharmacologic status of the patients. We analyzed fasting serum glucose and insulin levels 6 months after the completion of MPA treatment. Following treatment with metformin and after achievement of remission, BMI and HOMA-IR scores were both significantly reduced (Table 3).
Table 3
Changes in metabolic profiles after MPA plus metformin administration as fertility-sparing treatment (n=51)*

Group comparisons were performed by using the Wilcoxon signed rank test. All patients achieved complete response.
BMI, body mass index; CI, confidence interval; HOMA-IR, homeostasis model assessment of insulin resistance; MPA, medroxyprogesterone acetate.
*Patients who obtained pair data at pre- and post-treatment; †Post-treatment: 6 months after MPA treatment was completed; ‡Fasting level.
![]()
7. Compared with MPA alone group
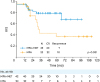
The median age of the control group of patients was 35 (range, 28–45 years). Five of 23 patients (20%) met the criteria for PCOS in the MPA alone group. There was some difference between the 2 groups; the incidence of PCOS in those treated with MPA+metformin was significantly higher than those who received MPA alone (p=0.013). Mean BMI (range) in MPA+metformin group was significantly higher than MPA alone group, which were 29.7 (27.3–32.0) and 23.3 (21.6–27.1), respectively (p=0.002).
In the MPA alone group, the responses rate was 20/23 (87%). After remission, 10 of 20 (50%) patients showed recurrence. Our results showed that patients treated with MPA plus metformin had significantly better prognoses than those treated with MPA alone did (OR=0.38; 95% CI=0.16–0.92; p=0.032). RFS in patients with MPA plus metformin and MPA alone group at 3 years was 79.3% and 45.2%, respectively (Fig. 3).
DISCUSSION
The present retrospective reanalysis demonstrated and confirmed that MPA plus metformin achieved a high response rate, low recurrence rate, and good fertility outcomes for fertility-sparing treatment of AEH and EC patients. The concurrent use of metformin appeared to be efficacious in terms of the RFS rate for patients with IR, especially in obese patients.
We have reconfirmed that MPA plus metformin can achieve a high response rate and low disease recurrence rate in fertility-sparing treatment for AEH and EC patients. Moreover, addition of metformin achieved a high rate of uterine preservation (median length of 57 months). A recent meta-analysis of a fertility-sparing treatment using only progestin showed a pooled regression rate of 77.2%; whereas the recurrence rate was 32.2% [5]. In another meta-analysis, long-term remission rates of all patients who started fertility-sparing treatment were under 50% [4]. Falcone et al. [13] reported a lower recurrence rate; however, these patients had undergone additional surgery after having live births. We could achieve long-term uterine preservation using progestin as a fertility-sparing treatment which had not been sufficiently efficacious in previous reports [345]. This study was a retrospective analysis; however, we first demonstrated the additional effect of metformin to fertility-sparing treatment using MPA in AEH and EC patients. Though the patients with MPA+metformin group were found to be more obese than the control group, which was thought as a general disadvantage, the addition of metformin improved the efficacy of fertility sparing treatment of MPA in the current study. We assume that the higher uterine preservation rate seen in the present study was achieved, at least in part, by retreatment; however, this was due primarily to the addition of metformin.
The present study demonstrated that the addition of metformin to MPA was more effective in treating obese patients. Several studies have revealed that increased BMI in patients correlated with poor response to progestin therapy and long treatment duration to achieve remission [141516]. Conversely, our results showed that addition of metformin treatment resulted in significantly better prognoses in patients with BMI ≥25 kg/m2 than in non-obese patients. Metformin has been thought to have both direct and indirect effects on patients with EC [17]. We speculated that metformin might be more effective in obese patients. First, the direct effect is related to the regulation of adenosine monophosphate-dependent kinase-dependent growth inhibition via the mTOR and MAPK signal pathways. These data have been reported in several cancer cell lines, including EC cell lines [89]. Second, metformin could suppress the secretion of adipokine from adipocytes. Adipokines, in addition to insulin and estrogen, play important roles in obesity-accelerated cancer [18]. Hence, metformin may regulate cell proliferation through suppressing the secretion of adipokines [1920]. Finally, the indirect effect of metformin might be related to the reduction of some humoral factors such as insulin-like growth factor 1(IGF-1) and leptin, which are known to act as growth factors [212223]. Our previous ex vivo results revealed that suppressing the humoral factors like IGF and leptin, but not insulin, will lead to reduced cell growth [24]. We hypothesized that the indirect effects of metformin more positively affected patients with obesity than they did patients without these conditions.
MPA with metformin achieved good fertility outcomes for fertility-sparing treatment of AEH and EC patients. In 1 meta-analysis, the live birth rate among women trying to conceive reached 26.3% and 28% in patients with EC and AEH, respectively [3]. We suggest that the improvement in the pregnancy rate (61%) and live birth rate (45%) seen in our study were affected by administration of metformin, because 50% of our cohort consisted of PCOS patients who commonly use metformin as an ovulation-inducing agent [2526]. Therefore, improvement of metabolic states such as IR and glucose intolerance due to metformin might produce good results for fertility outcomes.
The most common metformin-related adverse events were gastrointestinal symptoms, including nausea and diarrhea. A few patients discontinued metformin because of nausea; however, most of the patients were able to continue metformin treatment for a long time. It has been reported that glucose intolerance and increase in body weight are common side effects of MPA treatment [2728]. However, we suggest that metformin might countervail the metabolic impact of MPA and result in a decrease in the patient's weight after completion of MPA treatment, thus having a beneficial effect when taken during MPA treatment.
The primary limitation of the present study is that it was a retrospective analysis conducted at a single center. Moreover, we did not check the compliance with metformin administration after the end of the phase II study or evaluate the outcome of efficacy for all patients who were prescribed metformin-even if they only received 1 dose. Despite its limitations, the present study is the largest series to-date describing the long-term efficacy of metformin administration as a fertility-sparing treatment.
In summary, we have demonstrated metformin's efficacy as a fertility-sparing treatment as seen through reduction in the relapse rate after MPA therapy, especially in obese patients, and in its efficacy in improving the conception ratio.
 XML Download
XML Download