

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Epithelial ovarian cancer (EOC) remains the fourth leading cause of gynecological cancer-related death worldwide [1]. Ovarian clear-cell carcinoma (OCCC) is one of the representative histological types of EOC, accounting for 5%–25% of all EOCs [2]. OCCC is frequently diagnosed in Asian women and is known to exhibit higher chemoresistance than high-grade serous carcinoma, the most common type of EOC [2]. It has recently been reported that in early-stage OCCC, stage IC2–IC3 OCCC recurs more frequently and becomes chemoresistant compared to stage IC1 OCCC, due to occult metastasis [3]. Advanced as well as early disease can be refractory to chemotherapy; therefore, the establishment of a preoperative marker which can predict recurrence in early-stage OCCC is greatly anticipated.
Inflammatory responses play important roles in tumor initiation and development, and several systemic inflammatory response (SIR) markers that reflect the host response to the underlying malignancy have been explored [45]. SIR markers such as neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) are simple, easily available, and inexpensive to evaluate. Recent studies have shown that elevated NLR or PLR is associated with poor prognosis among patients with several types of cancers [678910].
In EOC, three meta-analyses investigated the prognostic role of NLR at diagnosis of ovarian cancer and concluded that NLR above a cut-off value was correlated with poor overall survival (OS) [111213]. A recent retrospective study reported the prognostic significance of SIR markers in OCCC, where elevated PLR or NLR prior to treatment were found to be associated with poor prognosis and poor response rate to chemotherapy [14]. The significance of SIR markers for prognosis of early-stage OCCC has not yet been elucidated. Previous studies about patients with OCCC indicated that high NLR and PLR were correlated with poor survival [14151617]; however, these studies were small and included both early- and advanced-stage patients. Substantially, inflammation increase as cancer progress, and increased numbers of neutrophils are found in the blood of many patients with advanced cancer [18]. Therefore, evidence about NLR and PLR as prognostic factors in patients with early-stage OCCC is insufficient, although the impact of SIR markers should be discussed in early- and advanced-stage patients separately.
The aim of this study was to elucidate the prognostic predictive significance of SIR markers in patients with stage I–II OCCC as defined by the International Federation of Gynecology and Obstetrics (FIGO).
MATERIALS AND METHODS
We retrospectively reviewed the records of 83 patients who underwent surgery and were diagnosed with OCCC at Nagoya University Hospital from 2005 to 2017. Written informed consent was obtained from all patients. This study was approved by the Ethics Committee of our institute (No. 2006-0357).
Treatment strategies for each patient were determined by several gynecologic oncologists depending on age, the ECOG performance status, and spread of disease. All patients underwent surgery without macroscopic residual disease. In detail, 59 patients (71.1%) underwent staging laparotomy including hysterectomy, bilateral salpingo-oophorectomy, omentectomy, and systematic pelvic and para-aortic lymphadenectomy. Whereas, 16 patients did not undergo staging laparotomy because of advanced age or complication, and five patients whose intraoperative diagnosis were borderline tumor did not receive lymphadenectomy. Moreover, 3 patients selected fertility sparing surgery including unilateral salpingo-oophorectomy and omentectomy. Regarding to adjuvant chemotherapy, most of the patients (n=74, 89.2%) received three to 6 courses of adjuvant chemotherapy, including carboplatin (area under curve [AUC] 5, day 1) and paclitaxel (175 mg/m2, day 1) combination regimen every three weeks. Post-treatment follow-up was performed monthly at the beginning, and then the interval was extended. Recurrence was determined via physical examination, trans-vaginal ultrasound, laboratory tests including complete blood count and tumor markers, and computed tomography.
Laboratory data including NLR and PLR were calculated from clinical records at the time of preoperative evaluation, post-treatment, and at recurrence. NLR was calculated as absolute neutrophil count divided by absolute lymphocyte count, and PLR was platelet count divided by absolute lymphocyte count in peripheral blood.
Three parameters of survival period included OS, progression-free survival (PFS), and post-recurrence survival (PRS). OS was defined as the time from initial surgery to death from any cause. PFS was the time from initial surgery to tumor progression or death from any cause. PRS was defined as the time from tumor progression to death from any cause.
Statistical analyses were performed with SPSS version 25 (IBM Corp., Armonk, NY, USA). The receiver operating characteristic (ROC) curve analysis for OS was performed, and optimal cut-off value was determined by the point on the curve with minimum distance from the left-upper corner of the unit square. Baseline characteristics were compared using independent samples t-test and Mann-Whitney U test. Kaplan-Meier curves were used for the analysis of OS, PFS, and PRS. The p-values were calculated by log-rank test. Multivariate Cox-regression analysis was used to further assess the variables proved significant in univariate analysis. The p<0.05 was considered statistically significant.
RESULTS
A total of 83 patients with OCCC were enrolled. In the 64.1-month median follow-up period (range, 2.1–149.6 months), 16 patients experienced recurrence, and nine died due to disease progression. The median NLR was 2.91 (range, 1.00–20.83), and the median PLR was 188 (range, 75–488).
First, ROC curves for survival were generated to evaluate correlation between SIR markers (NLR and PLR) and OS. The AUC for preoperative NLR and PLR was 0.761 and 0.609, respectively, and the optimal cut-off value for preoperative NLR and PLR was 3.26 and 165, respectively (Fig. 1). Moreover, accuracy, positive predictive value, and negative predictive value of NLR were 66.3%, 21.2%, and 69.0%, respectively, and those of PLR were 45.8%, 15.4%, and 69.8%, respectively. Then patients were stratified into 2 groups by the cut-off value of NLR or PLR (NLR-low [n=50] and NLR-high [n=33] groups or PLR-low [n=31] and PLR-high groups [n=52]). Clinical and pathological characteristics of patients are shown in Table 1. Age at diagnosis, FIGO stage, platelet count, cancer antigen 125 (CA125) level, surgery, and adjuvant chemotherapy were well-balanced between the NLR-high and NLR-low groups; however, neutrophil count, lymphocyte count, hemoglobin level, and positive ascites cytology were significantly increased in NLR-high compared to NLR-low group. A similar trend was also observed between PLR-high and PLR-low groups.
Fig. 1
Receiver operating characteristic curve analysis of preoperative NLR and PLR.
AUC, area under curve; NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio.
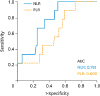
Table 1
Patient characteristics

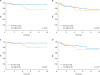
To identify the clinical significance of preoperative NLR and PLR, survival analysis was performed. Kaplan-Meier curves indicated that OS in NLR-low group was significantly longer than in NLR-high group (p=0.021; Fig. 2A). Five-year OS rate of NLR-low and NLR-high group was 95.6% and 80.2%, respectively. However, Kaplan-Meier curves showing PFS showed no significant difference between NLR-low and NLR-high group (p=0.668; Fig. 2B). No significant differences were found between PLR-low and PLR-high group for both OS and PFS (p=0.094 and 0.707, respectively; Fig. 2C and D). Five-year OS rate of PLR-low and PLR-high group was 96.7% and 84.3%, respectively, and five-year PFS rate of PLR-low and PLR-high group was 86.9% and 74.2%, respectively.
Fig. 2
Kaplan-Meier curves showing OS or PFS stratified by preoperative NLR or PLR. Curves showed OS stratified by NLR (A) and PLR (C). Curves showed PFS stratified by NLR (B) and PLR (D). The p-values were calculated by log-rank test.
NLR, neutrophil-to-lymphocyte ratio; OS, overall survival; PFS, progression-free survival; PLR, platelet-to-lymphocyte ratio.
Additionally, to clarify the reason higher preoperative NLR was associated with shorter OS, we also evaluated the significance of post-treatment NLR. Excluding two patients with rapid progression during adjuvant chemotherapy and one patient lost to follow-up, 80 patients with complete response to initial treatment were evaluated. Post-treatment NLR decreased in most cases and was similar for preoperative NLR-low and NLR-high groups (average post-treatment NLR in NLR-low and high group was 1.58 and 1.94, respectively; p=0.117; Fig. 3A). With respect to 16 recurrent/persistent cases, NLR at recurrence was significantly correlated with pretreatment NLR (Spearman's correlation coefficient was 0.624; p=0.010; Fig. 3B). There was a significant difference in PRS between NLR-low group and NLR-high group (p=0.019; Fig. 3C). Six of seven (85.7%) patients died, and only 1 patient (14.3%) survived with no evidence of disease in NLR-high group. On the other hand, only two of nine patients in NLR-low group died (22.2%).
Fig. 3
Transition of NLR and Kaplan-Meier curves showing PRS. (A) Transition of NLR in 80 patients who showed complete response to initial treatment. (B) Spearman's correlation between pretreatment NLR and NLR at recurrence. (C) Curves showed PRS stratified by pretreatment NLR. The p-value was calculated by log-rank test.
NLR, neutrophil-to-lymphocyte ratio; PRS, post-recurrence survival.

Finally, the potential impact of factors on OS was assessed using Cox-regression hazard models (Table 2). In the univariate analysis, FIGO stage II (HR=13.729; 95% CI=3.396–55.508; p<0.001) and preoperative NLR-high (HR=5.267; 95% CI=1.092–2.413; p=0.039) were significant unfavorable prognostic factors, although other factors including age, anemia, CA125 level, and ascites cytology were not significant prognostic factors. To eliminate confounding effect from a number of clinicopathological factors, multivariate OS analysis was done for all factors. Results indicated that FIGO stage II (HR=18.108; 95% CI=3.613–90.759; p<0.001) and preoperative NLR-high (HR=7.437; 95% CI=1.427–38.770; p=0.017) were significant independent poor prognostic factors.
Table 2
Univariate and multivariate Cox-regression analysis for overall survival in patients with stage I–II disease

DISCUSSION
It is often difficult to predict the clinical course of patients with malignant tumors, and establishment of an appropriate prognostic factor has been anticipated. It has been reported that positive ascites cytology is significantly associated with poor prognosis in early-stage OCCC [3]. As preoperative setting, there is growing evidence of SIR markers in various cancers, including EOCs [678910111213], and NLR is an inexpensive and readily-available biomarker of patients with early-stage OCCC. The present study explored optimal cut-off values of NLR and PLR. According to previous reports about OCCC, cut-off value of NLR and PLR was 2.3–2.8 and 123.6–205.4, respectively [141617]. Moreover, in other reports regarding EOCs, cut-off value of NLR was 2.3–5.25 [11]. Therefore, NLR>3.26 and PLR>165 in the present study were acceptable within the range of previous values.
The present study indicated that NLR and FIGO stage were independent prognostic factors for OS in patients with stage I–II OCCC. However, NLR was not associated with PFS. According to previous reports about OCCC that included 29.0%–41.3% of advanced stage patients, high NLR was one of the significant poor prognostic factors for both OS and PFS in univariate analysis [141617]. However, the results of multivariate analysis were not consistent. Overall, NLR was not considered to be an independent prognostic factor, but advanced stage was significant independent prognostic factor in multivariate analysis [141617]. Therefore, NLR and FIGO stage were considered as cofounding factor, and the proportion of advanced stage patients might affect the prognostic significance of NLR. However, interestingly, NLR was a useful prognostic factor for OS in this study that included only early-stage OCCC patients. On the other hand, the present study indicated that high PLR tended to be related to poor OS, but there was no significant difference. According to the previous reports about OCCC in all stages, high PLR was not a poor prognostic factor [1617]. Another report showed that high PLR was significant associated with shorter PFS, but about 90% of the patients with PLR-high group were advanced stage [15]. Therefore, clinical efficacy of PLR as prognostic factor was uncertain. In summary, NLR was thought to be a useful prognostic factor in early-stage OCCC patients, and its impact and optimal cut-off values should be validated in a large-scale study.
Preoperative NLR was related to OS but not PFS, which reflected that high preoperative NLR related to short PRS. In stage I–II OCCC, most of the patients showed complete response to initial treatment, and NLR decreased after treatment, reflecting resection and improvement of tumor inflammation. When recurrence happened, NLR increased to the same level as preoperative NLR. Therefore, preoperative NLR may predict tumor inflammation at recurrence. Certainly, NLR at recurrence is also thought to be a useful biomarker, but it may be affected by factors such as site of recurrence and previous treatment. Therefore, we consider it important to evaluate NLR at initial diagnosis. One of the reasons why NLR was related to OS and PRS might be chemosensitivity. A previous report showed that NLR and PLR predicted chemosensitivity in advanced gastric cancer [19]. Moreover, patients with low NLR had a higher pathological response rate after neoadjuvant therapy in advanced esophageal cancer [20], triple-negative breast cancer [21], and colorectal liver metastasis [22]. Therefore, we considered that patients with OCCC with low NLR also had high chemosensitivity and showed longer PRS.
Considering the immunologic aspect of NLR, tumor-infiltrating neutrophils (TINs) are known to play important roles in cancer microenvironment. TINs may exert a multitude of pro- and anti-tumorigenic effects, and some neutrophils behave as myeloid-derived suppressor cells [18]. Therefore, a high amount of TINs is also associated with poor survival. Whereas, prognostic value of tumor-infiltrating lymphocytes (TILs) is also discussed. In ovarian cancer, the presence of intraepithelial TILs was associated with improved OS and PFS [23]. However, there are many different subsets of TILs, and further evaluations are essential. Overall, high TINs and low TILs are considered to be associated with poor survival. To elucidate the immunologic aspect of NLR, further studies to clarify the association between tumor infiltrating immune cells and NLR are necessary.
There are several limitations in the present study. At first, only 83 patients from a single institution were included, and underlying biases in our analysis could not be controlled due to the retrospective study design. Therefore, our results should be validated in prospective larger-scale studies. Furthermore, tumor tissue samples are not evaluated. Thus, it remains unknown whether NLR is correlated with tumor immune microenvironment, such as TILs.
In conclusion, we suggest that NLR at initial diagnosis is an independent prognostic factor for OS in patients with FIGO stage I–II OCCC. Moreover, NLR is a possible predictor of treatment response after recurrence, although it cannot predict recurrence. PLR shows no significant impact on OS or PFS. Therefore, NLR is thought to be a reliable biomarker for OCCC. Further evaluation of immuno-oncology and NLR is desirable.
 XML Download
XML Download