

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Ovarian cancer is the fifth most common female cancer worldwide and its mortality rate is 20%. Because women with early stages of ovarian cancer have few definite clinical symptoms, over 80% of ovarian cancer is diagnosed in the advanced stages [1]. To overcome the high mortality of ovarian cancer, multiple studies focusing on screening for ovarian cancer have been performed worldwide.
To detect ovarian cancer, tumor markers are usually measured along with transvaginal ultrasound examination (TVU). A traditional tumor marker for ovarian cancer is cancer antigen 125 (CA 125), a high molecular weight glycoprotein which reacts to the monoclonal antibody generated from ovarian cancer cell line. CA 125 was elevated in some kinds of cancers including ovary. Finally, it had been the most commonly used biomarker for ovarian cancer [2]. However, CA 125 has clinical limitations as an effective tumor marker because it showed low specificity to predict ovarian cancer. Elevation of serum CA 125 is associated with benign conditions or physiological status as well as ovarian malignancy: endometriosis, uterine fibroids, pelvic inflammatory disease, menstruation, pregnancy, peritoneal tuberculosis, peritonitis, or following recent abdominal surgery [3]. Furthermore, CA 125 has low sensitivity especially in the early stage of ovarian cancer [4].
Human epididymis protein 4 (HE4) is translated from the WFDC2 gene. Although it was already known as an epididymis-specific protein, it was amplified in sera of patients with epithelial ovarian cancer [5]. Because HE4 showed higher specificity than CA 125, it has been identified as a tumor marker for ovarian cancer [6]. Even in endometriosis, HE4 was less affected than CA 125 [78]. When HE4 was used together with CA 125 to detect ovarian cancer, sensitivity and specificity were enhanced [9]. Thus, Risk of Ovarian Malignancy Algorithm (ROMA), the calculation with CA 125 and HE4 according to menopausal status, was proposed to discriminate ovarian cancer from benign conditions [10]. Many studies validated the discrimination power of ROMA including Asian populations [11].
However, some researchers could not identify the superiority of ROMA over CA 125 or HE4 alone and have tried to devise new potential tumor marker for ovarian cancer [12]. There were few studies that evaluated the effect of menopause on ROMA, although ROMA was induced from two different calculations according to menopausal status [10]. In Korea, ROMA is commonly used to detect ovarian malignancy without definite guidelines for general population [13]. Therefore, we designed this study to evaluate the discrimination power of ROMA compared with CA 125 or HE4 in Korean women.
MATERIALS AND METHODS
1. Patients
The Institutional Review Board of Seoul National University Hospital approved this study (IRB No. 1604-050-753). We retrospectively collected medical data of women who visited the hospital for regular checkup between March 2015 and March 2016 in Seoul National University Hospital and Seoul National University Hospital Healthcare System Gangnam Center, a medical college-based hospital and its health promotion and screening center. We defined that regular checkup is gynecologic examination with cervical cancer screening and TVU to physically healthy women without symptoms. Women with ovarian cystic masses of age 19 or higher, who underwent TVU and blood tests for CA 125, HE4, and ROMA were included in our study. Women who had previous history of gynecologic cancer were excluded, while survivors of non-gynecologic cancer were included.
2. Measurement
Blood tests for tumor markers of ovarian cancer were performed except during menstruation, and samples were examined within 4 hours of collection. The CA 125 and HE4 were measured using the ARCHITECT system (Abbott Diagnostics, Abbott Park, IL, USA). The calculation of ROMA was performed as described by Moore et al. [10] In postmenopausal women, the predictive index (PI)=−8.09+1.04×LN (HE4)+0.732×LN (CA 125). In premenopausal women, PI=−12.0+2.38×LN (HE4)+0.0626×LN (CA 125). The predictive probability (%)=exp (PI)/[1+exp (PI)]. The predictive probability corresponds to ROMA according to menopause status. Menopause was defined when a period of amenorrhea persisted over 1 year. If women had an unknown menstruation date, premenopause was determined by confirming serum follicle stimulating hormone level below 22 IU/L. The cut-off value for CA 125 was 35 IU/L. The instructions of our equipment applied different cut-off values for HE4: 70 IU/L in premenopausal women, and 140 IU/L in postmenopausal women [14].
TVU was performed to identify ovarian cyst or to find the morphologic abnormality of these lesions. Some patients underwent surgical exploration afterwards in case of the following surgical indications: findings suggesting malignancy, such as, solid portion, papillary projection, multiple septa, large volume, and increased color Doppler flow; symptoms related to ovarian cysts, such as abdominal pain, vaginal spotting, and mass effect [1516]. Pathologic diagnosis was confirmed with specimen examination after surgical operation. Others were followed-up using TVU every 3 months to identify malignant transformation [1718]. The number of patients newly diagnosed with ovarian malignancy within a year were investigated.
Two types of ovarian cancer, primary ovarian cancer including borderline ovarian malignancy and metastatic ovarian cancer originating from other organs, were analyzed in this study. Metastatic ovarian cancer was included when detected during preoperative work-up or when identified by pathologic diagnosis after surgical exploration.
3. Statistical analysis
Continuous or numeric variables, such as age and levels of tumor markers, were analyzed with the Student's t-test or Mann-Whitney rank test. Nominal or ordinal variables, such as menopausal status and pathologic diagnosis were analyzed with χ2 test or Fisher's exact test. Receiver operating characteristic (ROC) curve analysis was performed to predict the risk of ovarian malignancy. To compare the area under the curve (AUC) between ROC curves, pairwise comparison analyses were used [19]. Statistical analyses were performed with SPSS 21 software (SPSS, Inc., Chicago, IL, USA). A p-value less than 0.05 was considered statistically significant.
RESULTS
Fig. 1 is the flow chart of this study for patients' selection. A total of 876 women who had ovarian cysts on TVU underwent blood tests for tumor markers, including CA 125, HE4, and ROMA. Among them, 532 patients were premenopausal (60.7%) and 344 were postmenopausal women (39.3%). Surgical exploration and pathological diagnosis for ovarian cysts were conducted in 157 premenopausal women (29.5%) and 102 postmenopausal women (29.7%). In premenopausal women who took surgical exploration, there were 32 patients with primary ovarian cancer, 1 patient with secondary ovarian cancer, 11 patients with borderline ovarian malignancy, and 113 patients with benign ovarian cysts. In postmenopausal women who took surgical exploration, there were 48 patients with primary ovarian cancer, 2 patients with secondary ovarian cancer, 1 patient with borderline ovarian malignancy, and 51 patients with benign ovarian cysts. The other women took serial monitoring with TVU. Among them, there were 375 women with premenopause (70.5%) and 242 women with postmenopause (70.4%).

Table 1 shows the patients' characteristics according to menopausal status. Distribution of elevated CA 125 and ovarian lesions between pre- and postmenopausal women were analyzed with χ2 tests. The values of CA 125, HE4, and ROMA did not follow normal distribution and were skewed to the lower level within the reference range. The proportion of elevated CA 125 was higher in the premenopausal women than in the postmenopausal women (p=0.003), whereas the proportion of elevated HE4 and high-risk ROMA was higher in the postmenopausal group than in the premenopausal group (p=0.001 and p=0.036).
Table 1
Patients' characteristics according to menopause status
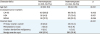
Values are presented as median (range) or number (%).
CA 125, cancer antigen 125; HE4, human epididymis protein 4; ROMA, Risk of Ovarian Malignancy Algorithm.
![]()
Most of the ovarian cystic masses primarily found on TVU had benign nature. Malignant lesions were more frequently found in postmenopausal women than in premenopausal women (p<0.001). The number of patients with primary ovarian cancer in the premenopausal group was 32 (6.0%) and that in the postmenopausal group was 48 (14.0%). A total of 13 patients had ovarian metastasis from other organs. The origins of metastatic tumor to the ovary were the uterine endometrium (n=5, 38.5%), intestine (n=3, 23.1%), stomach (n=2, 15.4%), pancreas (n=1, 7.7%), and bile duct (n=2, 15.4%). The number of uterine endometrial cancer was 1 (0.2%) in premenopausal and 4 (1.2%) in postmenopausal women.
Among the patients, 123 women (14.0%) had previous history of non-gynecologic malignancy: breast (n=75, 8.6%), stomach and colorectal (n=21, 2.4%), and hepatobiliary cancer (n=9, 1.0%). In patients with previous breast cancer, 1 woman had BRCA1 mutation and 1 woman had BRCA2 mutation (2.6%). The type of underlying malignancy did not correlate with the existence of malignant ovarian cyst (p=0.294). There was no difference in the three tumor markers between primary and metastatic ovarian cancer: serum CA 125 levels, serum HE4 levels, and ROMA value (p=0.074, p=0.349, p=0.713, respectively).
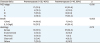
Table 2 shows the histopathologic results of primary ovarian cancer which were evaluated in this study. The postmenopausal group had significantly more patients with an advanced stage (p=0.016) and a higher pathologic grade (p=0.003) than the premenopausal group. Among the various histological types, serous cystadenocarcinoma was most common in both premenopausal and postmenopausal groups.
Table 2
Histopathologic results of primary ovarian cancer
![]()
Table 3 indicates the predictive power of tumor markers for ovarian cancer. The overall sensitivity of ROMA to discriminate ovarian malignancy was 66.7% and the overall specificity was 86.8%. HE4 had the highest positive predictive value and ROMA had the highest negative predictive value to detect ovarian malignancy among CA 125, HE4, and ROMA. These tumor markers had distinct diagnostic accuracy depending on menopausal status. The diagnostic accuracy of HE4 was high in premenopausal women and that of CA 125 was high in postmenopausal women.
Table 3
Sensitivity and specificity of tumor markers for ovarian cancer
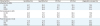
CA 125, cancer antigen 125; HE4, human epididymis protein 4; NPV; negative predictive value; PPV, positive predictive value; ROMA, Risk of Ovarian Malignancy Algorithm.
![]()
Fig. 2 shows the ROC curves of tumor markers according to menopausal status. In premenopausal women, AUCs of variables were 0.685 for CA 125 (95% confidence interval [CI]=0.644–0.725), 0.732 for HE4 (95% CI=0.692–0.769), and 0.731 for ROMA (95% CI=0.691–0.768). The difference between the AUCs of the ROC curves of HE4 and ROMA was not statistically significant according to pairwise comparison analysis in premenopausal women (p=0.832, Fig. 2A). In postmenopausal women, the AUCs of variables were 0.888 for CA 125 (95% CI=0.849–0.919), 0.845 for HE4 (95% CI=0.803–0.882), and 0.871 for ROMA (95% CI=0.831–0.905). The difference between the AUCs of the ROC curves for CA 125 and ROMA was not statistically significant according to pairwise comparison analysis in postmenopausal women (p=0.440, Fig. 2B). Excluding secondary ovarian cancer, metastatic cancer from other organs to ovary, AUCs of tumor markers were as follows: 0.681 for CA 125 (95% CI=0.587–0.774), 0.734 for HE4 (95% CI=0.644–0.823), and 0.731 for ROMA (95% CI=0.639–0.822) in premenopausal women; 0.883 for CA 125 (95% CI=0.815–0.951), 0.837 for HE4 (95% CI=0.771–0.903), and 0.861 for ROMA (95% CI=0.789–0.932) in postmenopausal women.

DISCUSSION
In this study, we evaluated the power of ROMA to predict ovarian malignancy compared with CA 125 and HE4 alone according to the menopausal status of Korean women. Previous study on ROMA in Korean population suggested optimized weights of CA 125 and HE4 incorporated in ROMA [20]. Going one step forward from that previous study, we investigated the non-inferiority of existing tumor marker itself comparing ROMA according to menopausal status. There are some previous studies to propose the association between menopause and tumor markers for ovarian cancer. In our study, we included large number of women with ovarian cysts in Korean general population because we intended to evaluate the clinical usage and interpretation of common tumor markers for ovarian cancer according to menopause in general population. The results of our study correspond to previous studies which reported that menopausal status affected diagnostic ability of CA 125, HE4, or ROMA. Thus, clinicians would be helped to interpret ROMA by comparing CA 125 or HE4 according to menopausal status in actual clinical field [2122].
In the same viewpoint, our study included patients with secondary ovarian cancer metastasis from other origin as well as primary ovarian cancer. TVU was usually conducted to women with ovarian cysts in the primary care, however, it had limitations in discriminating benign ovarian lesion, primary ovarian cancer, or secondary ovarian cancer. In this study, metastasis was confirmed after cancer workup or pathologic review after surgical exploration. The origins of secondary ovarian cancer were the uterine endometrium, colorectal, stomach, and biliary system in order of frequency. ROMA was increased in metastatic ovarian cancer from uterine endometrium or gastrointestinal tract [23].
We investigated the sensitivity, specificity, and ROC curves of ovarian tumor markers; CA 125, HE4, and ROMA. The highest sensitivity was found in ROMA and the highest specificity was found in HE4 without considering menopausal status. However, discrimination power of these tumor markers was different according to menopausal status [24]. As same as our results, previous studies reported that higher sensitivity and higher specificity of CA 125 were observed in postmenopausal women than in premenopausal women [25]. On the other hand, we analyzed that diagnostic accuracy of HE4 was higher in premenopausal women than in postmenopausal women. HE4 was more accurate in younger population, because HE4 levels increase according to age [26].
In the ROC curve analyses, menopausal status was associated with an effective tumor marker to identify ovarian malignancy including secondary ovarian cancer or not. Although the differences between the AUCs of the ROC curves were not significant, the widest areas were found under the ROC curve of CA 125 in postmenopausal women and under the ROC curve of HE4 in premenopausal women. A meta-analysis reported similar results to our study. CA 125 was more suitable than ROMA in postmenopausal women and HE4 was more suitable than ROMA in premenopausal women according to ROC curve analysis [27]. If menopausal status was checked in advance of the interpretation of tumor markers, HE4 or CA 125 alone was not inferior to ROMA in determining ovarian malignancy.
The discriminating power of ROMA for ovarian malignancy was not higher in our study than those found in previous studies. Unlike previous studies that included women with ovarian cysts who were scheduled to undergo surgery, our study included women with ovarian cysts found during regular check-up regardless of treatment thereafter [10]. Although there were few data on the predictability of ROMA for screening ovarian cancer, generalized ovarian cysts which we analyzed would have decreased the power of ROMA. Low HE4 would also have reduced the power of ROMA in our study. Most cases showed lower level of HE4 than the cut-off value by manufacturer's guideline. HE4 level is known to be affected by ethnicity, and Asian populations had a wide reference range of HE4 [1328]. In Korean women, a new cut-off level of HE4 was suggested to differentiate ovarian cancer from benign lesion. The revised cut-offs of HE4 in Korean was more predictable to ovarian cancer, and it was lower than the presented cut-offs by manufacturer's guideline [29].
Our study has some limitations. The number of ovarian malignancy was not sufficient to establish a new cut-off level of HE4 in Korea women. However, we suggested the possibility of ROMA for ovarian cancer screening and assured the inadequate reference range of HE4 in Korean women. The whole women included in this study was not evaluated for BRCA mutation. However, the prevalence of BRCA mutation in included women with previous history of breast cancer was similar to the usual risk of BRCA mutation in Korean with breast cancer [30]. Despite a retrospective review of medical records, this is the first study to report the discriminating power of ROMA in women with ovarian cysts found from the general population in Korea.
In conclusion, we investigated the discrimination power of ROMA compared with CA 125 or HE4 when considering menopausal status. ROMA was not superior to HE4 in premenopausal women and was not superior to CA 125 in postmenopausal women. Our study may help clinicians to clarify the clinical interpretation of ROMA. To apply ROMA for ovarian cancer screening to different ethnicities, an additional prospective study should be performed.
 XML Download
XML Download