

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Neuroendocrine carcinoma occurs predominantly in the lungs, but it can be occasionally found in the digestive system and genitourinary tract. In the female genital tract, primary neuroendocrine carcinomas are observed mainly in the uterine cervix; the endometrium is the least common site of occurrence [12]. Primary neuroendocrine tumors of the endometrium include small cell neuroendocrine carcinoma (SCNEC), large cell neuroendocrine carcinoma (LCNEC), and carcinoid tumors. SCNEC and LCNEC are categorized as high-grade neuroendocrine carcinoma, while carcinoid tumors are categorized as low-grade neuroendocrine tumors [3]. The majority of neuroendocrine tumors of the endometrium are SCNEC; they account for approximately <1% of all endometrial carcinomas. LCNEC of the endometrium is considered rarer than SCNEC [4567]. To date, there have only been 2 reports of carcinoid tumors of the uterine corpus [89].
Although there are no established data regarding the prognosis of and the prognostic factors associated with neuroendocrine carcinoma of the endometrium due to its rarity, it is often detected at advanced stages and has a poor prognosis [12410]. Additionally, there are no evidence-based therapeutic regimens due to the rarity. However, some advanced stage cases treated with multidisciplinary treatment approaches (surgery, chemotherapy, and radiation therapy) obtained long-term survival [1112].
The aims of this study were to describe cases of neuroendocrine carcinoma of the endometrium from multiple medical institutions in order to clarify its clinicopathologic features, treatment, prognosis and prognostic factors and to collate findings to establish future individualized treatment regimens. To our knowledge, this is the largest retrospective case study of neuroendocrine carcinoma of the endometrium. Additionally, it is the first study to statistically analyze the prognosis and prognostic factors associated with this disease.
MATERIALS AND METHODS
1. Study population and clinical data collection
This was a multi-institutional retrospective case study. It enrolled cases diagnosed with neuroendocrine carcinoma of the endometrium between January 1995 and December 2014 at medical institutions participating in the Kansai Clinical Oncology Group (KCOG)/Intergroup. In total, 65 cases were registered from 18 medical institutions throughout Japan. Information about patient characteristics, International Federation of Gynecology and Obstetrics (FIGO) stage, histologic findings, treatment methods, progression-free survival (PFS), overall survival (OS), were obtained from patient medical records at each medical institution. The exclusion criteria were as follows: a history of other types of cancer within 5 years prior to the diagnosis of neuroendocrine carcinoma of the endometrium, and the presence of other types of cancer at diagnosis. The carcinoid tumors were not included in this study. The FIGO stage was classified according to the 2008 FIGO clinical staging system. The cases whose stages were classified according to the FIGO clinical staging system of 1988 were modified to meet the definitions of the 2008 FIGO clinical staging system [13].
2. Central pathologic review
Surgically resected or biopsy specimens were collected. Immunohistochemically stained slides for markers such as CD56, chromogranin A, and synaptophysin were collected whenever possible. In all cases, a histopathologic review was conducted independently by 2 pathologists from different medical institutions. Cases diagnosed with neuroendocrine carcinoma of the endometrium based on agreement between the 2 pathologists were analyzed. The pathologic criteria of this study were defined in accordance with the World Health Organization (WHO) classification of tumors of female reproductive organs (2014) [3]. Additionally, the WHO classification of tumors of the lung, pleura, thymus, and heart (2015) and the WHO classification of tumors of the digestive system (2010) were also referred to [1415]. Neuroendocrine carcinomas of the endometrium are often associated with tumors of other histologic types, such as endometrial atypical hyperplasia, endometrioid carcinoma, carcinosarcoma, or serous carcinoma. Such cases were defined as mixed type. Even though there was no established definition for mixed types of neuroendocrine carcinoma, this classification was recognized to be important for neuroendocrine carcinoma occurring in many anatomic sites [16]. Cases reported in the past occurring in the endometrium as well were often divided into pure and mixed types [124]. There has been no report that suggested a difference in prognosis between pure and mixed types in neuroendocrine carcinoma of the endometrium. However, in the digestive system, it is assumed that there is a difference in prognosis between pure and mixed types (mixed neuroendocrine-non-neuroendocrine neoplasms) [1718]. Therefore, we divided the registered cases into these types in order to investigate their prognosis. Mixed type was defined as a tumor consisting of >30% of both a neuroendocrine carcinoma component and a non-neuroendocrine carcinoma component based on the definition of neuroendocrine carcinoma of the digestive system [1718]. As the diagnosis of the histological type (pure or mixed) based on biopsy specimens is often difficult, we excluded cases in which differentiating between pure type or mixed type, based on biopsy specimens, was difficult.
3. Outcome measures
OS was defined as the time from starting initial treatment to the last follow-up visit or death. PFS was defined as the time from starting initial treatment to the first recurrence or the progression of disease and death. Participants were followed for 1–134 months.
4. Statistical analysis
Patients' characteristics were summarized using descriptive statistics or contingency tables. Cumulative PFS and OS rates were calculated using Kaplan-Meier methods, and the survival curves were compared using log-rank tests. To evaluate the prognostic factors associated with neuroendocrine carcinoma of the endometrium, multivariate analysis was performed. The evaluated prognostic factors were selected referencing the past reports of neuroendocrine carcinoma of the endometrium [12410] and a review of endometrial cancer [19]. The potent prognostic factors included were as follows: age (<60 years, ≥60 years), performance status (0–1, 2–4), FIGO stage (I–II, III–IV), surgery (no surgery or incomplete surgery [meaning a macroscopic residual lesion], complete surgery [meaning no macroscopic residual lesion]), and histologic subtypes (SCNEC, LCNEC) (pure type, mixed type). Additionally, the prognostic factors for 35 surgical cases were evaluated. The prognostic factors potentially associated with surgical cases were as follows: age (<60 years, ≥60 years), performance status (0–1, 2–4), FIGO stage (I–II, III–IV), surgery (incomplete surgery, complete surgery), histologic subtypes (SCNEC, LCNEC) (pure type, mixed type), lymphovascular space invasion (negative, positive), and post-operative adjuvant chemotherapy (no adjuvant chemotherapy, adjuvant chemotherapy). We constructed a scatter diagram method to confirm that there was no linear relationship between any of the factors. We used a Cox proportional hazards model to assess the impact of multiple covariates on the OS. All of the independent variables used in the univariate and multivariate analyses were expressed in a categorical form. Age, performance status, FIGO stage, surgery, histologic subtypes, lymphovascular space invasion, and post-operative adjuvant chemotherapy were regarded as categorical variables. The results of the univariate and multivariate analyses were expressed as hazard ratios (HRs) and 95% confidence intervals (CIs). For all analyses, the Statistical Package for Social Science software (IBM SPSS Statistics 25; IBM Corp., Armonk, NY, USA) was used, and p-values < 0.05 were considered statistically significant.
5. Ethics
This study was registered with the UMIN-Clinical Trials Registry (UMIN000019710). The protocol was approved by the KCOG Protocol Review Committee and the institutional review board of each participating institution. Due to the retrospective nature of this study, the need for informed consent was waived. The protocol was made available to the public on the homepage of the participating institutions. All authors have declared no conflicts of interest.
RESULT
1. Central pathologic review
Fig. 1 shows the flow diagram for the participants included in this study. Upon the central pathological review, both of the pathologists agreed that 42 (64.6%) of the 65 cases had neuroendocrine carcinoma of the endometrium. Ten of 65 cases were excluded for the following reasons: poor quality specimens thus hindering a diagnosis (n=6), severe damage to the tumor by the neoadjuvant chemotherapy (n=2), and carcinoma of non-endometrial origin (n=2). There was disagreement regarding the original diagnosis among the 13 (20.0%) remaining cases. Among the conflicting diagnoses, 5 (38.5%) were endometrioid carcinoma G2 or G3, 5 (38.5%) were undifferentiated carcinoma, and 3 (23.1%) were carcinosarcoma cases. There have been no reports that investigate the relationship between prognosis and the associated histological type (such as endometrial atypical hyperplasia, endometrioid carcinoma, carcinosarcoma, or serous carcinoma) of the mixed type. In this study, too, due to the small numbers of each associated histological type for the mixed types, the relationship between prognosis and the associated histological type of the mixed type could not be evaluated. The positivity rates as a result of immunohistochemical staining were 83.3%, 64.3%, and 78.6% for CD56, chromogranin A, and synaptophysin among all cases, 75.0%, 53.6%, and 78.6% for CD56, chromogranin A, and synaptophysin among SCNEC cases, and 100%, 85.7%, and 78.6% for CD56, chromogranin A, and synaptophysin among LCNEC cases, respectively (Supplementary Table 1). In this study, the positivity rates of CD56 and chromogranin A tended to be high in LCNEC cases; however, the reason for this tendency was not known, and such results have not been observed in other similar studies.
 | Fig. 1Flow diagram for the central pathologic review.LCNEC, large cell neuroendocrine carcinoma; SCNEC, small cell neuroendocrine carcinoma.
|
There was a possibility that some mixed type cases were misdiagnosed as pure type only based on the biopsy specimens. Nine cases were diagnosed only using the biopsy specimens, and of these, 2 cases were excluded because the diagnosis was difficult.
2. Patients' characteristics
In total, 42 cases diagnosed with neuroendocrine carcinoma of the endometrium were included. The median age at diagnosed was 58 years (range, 44–79); the median age did not significantly differ for SCNEC and LCNEC (57.5 years [range, 44–79] vs. 59 years [range, 44–78], retrospectively). The median follow-up period was 28 months (overall range, 1–134). 11 (26.2%), 2 (4.8%), 15 (35.7%), and 14 (33.3%) cases had FIGO stages of I, II, III, and IV, respectively. Overall, 69.0% of cases were of an advanced FIGO stages (stage III and IV). The subtypes identified included pure type SCNEC, mixed type SCNEC, pure type LCNEC, and mixed type LCNEC, in 17 (40.5%), 11 (26.2%), 7 (16.7%), and 7 (16.7%) cases, respectively (Table 1).
Table 1
The distribution of the FIGO stage and histologic subtype, and treatment of each FIGO stage (n=42)

Values are presented as median (range) or number of patients (%).
BSC, best supportive care; CCRT, concurrent chemoradiotherapy; CT, chemotherapy; FIGO, International Federation of Gynecology and Obstetrics; LCNEC, large cell neuroendocrine carcinoma; NAC, neoadjuvant chemotherapy; RT, radiotherapy; SCNEC, small cell neuroendocrine carcinoma.
![]()
The initial treatments administered for each stage are shown in Table 1. Among surgical cases, the type of hysterectomy (simple total hysterectomy, modified radical hysterectomy, or radical hysterectomy), the range of lymphadenectomy (none, pelvic only, or pelvic to para-aortic lymph nodes), and the additional resection (omentectomy, intestinal resection, and others) varied by medical institution. The relationship between the surgical procedures conducted and rate of surgery completion (meaning no macroscopic residual lesion) or prognosis was unevaluable. The chemotherapy regimens (including neoadjuvant chemotherapy, postoperative adjuvant chemotherapy, and chemotherapy only) used in 31 cases included a platinum drug. The most frequently used regimen was paclitaxel+carboplatin (conventional or dose dense) therapy (n=15, 48.4%), followed by cisplatin+CPT-11 therapy (n=10, 32.3%), etoposide+cisplatin therapy (n=4, 12.9%), and others (there were some overlaps).
3. Outcomes
The 5-year cumulative PFS rates were 81.8%, 50.0%, 32.5%, and 14.3% for FIGO stages I, II, III, and IV, respectively (Supplementary Fig. 1). The 5-year cumulative OS rates were 88.9%, 100.0%, 46.7%, and 21.4% for FIGO stages I, II, III, and IV, respectively. The OS was significantly decreased among cases with advanced FIGO stages (stage III and IV) (p=0.001) (Fig. 2).
 | Fig. 2OS based on FIGO stages for all cases. OS was significantly decreased among cases with advanced FIGO stages (stage III and IV) (p=0.001).FIGO, International Federation of Gynaecology and Obstetrics; OS, overall survival.
|
The 5-year cumulative PFS rates were 26.1%, 54.5%, 28.6%, and 71.4% for pure type SCNEC, mixed type SCNEC, pure type LCNEC, and mixed type LCNEC, respectively (Supplementary Fig. 2). The 5-year cumulative OS rates were 29.4%, 60.6%, 57.1%, and 85.7% for pure type SCNEC, mixed type SCNEC, pure type LCNEC, and mixed type LCNEC, respectively. OS was significantly decreased among cases with pure type SCNEC (p=0.020) (Fig. 3). It should be noted that the rate of cases with advanced FIGO stages (stage III and IV) was higher among those with pure type SCNEC. The rates of advanced FIGO stages were 88.2%, 45.5%, 71.4%, and 57.1% among those with pure type SCNEC, mixed type SCNEC, pure type LCNEC, and mixed type LCNEC, respectively (Supplementary Table 2).
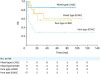 | Fig. 3OS based on histologic subtypes for all cases. OS was significantly decreased among cases with pure type SCNEC (p=0.020).LCNEC, large cell neuroendocrine carcinoma; OS, overall survival; SCNEC, small cell neuroendocrine carcinoma.
|
Upon univariate analysis, performance status, FIGO stage, surgery, and histologic subtypes (pure type, mixed type) were significant prognostic factors for neuroendocrine carcinoma of the endometrium. However, upon multivariate analysis, only surgery and histologic subtypes (pure type, mixed type) were significant prognostic factors. Significantly better prognoses were observed in complete surgery cases than in no surgery or incomplete surgery cases (multivariate HR=0.071; 95% CI=0.022–0.226; p<0.001). Significantly better prognoses were observed in mixed type cases than in pure type cases (multivariate HR=0.320; 95% CI=0.113–0.907; p=0.032) (Table 2). Upon multivariate analysis of the prognostic factors associated with the 35 surgical cases, only surgery and histologic subtypes (pure type, mixed type) were significant. However, due to the small number of the events of surgical cases, the statistical analysis was not robust (data not shown).
Table 2
Cox proportional hazards model of the prognostic factors associated with neuroendocrine carcinoma of the endometrium
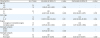
CI, confidence interval; FIGO, International Federation of Gynecology and Obstetrics; HR, hazard ratio; LCNEC, large cell neuroendocrine carcinoma; SCNEC, small cell neuroendocrine carcinoma.
![]()
Fig. 4 shows the Kaplan-Meier analysis of OS for the no surgery, incomplete surgery, and complete surgery cases with advanced FIGO stages (stage III and IV). Upon analysis of OS among cases with no surgery, incomplete surgery, and complete surgery, OS was significantly improved among cases with complete surgery (p<0.001) (Fig. 4). Moreover, PFS was also significantly improved among cases with complete surgery (p<0.001) (Supplementary Fig. 3).
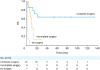 | Fig. 4OS based on surgery for cases with advanced FIGO stages (stage III and IV). OS was significantly improved among cases with complete surgery (p<0.001).FIGO, International Federation of Gynecology and Obstetrics; OS, overall survival.
|
Overall, 21 (50%) cases had recurrence; there was a high rate of hematogenous recurrence compared to lymphogenous or local recurrence (Supplementary Table 3).
DISCUSSION
In the past, only 2 retrospective case studies of SCNEC of the endometrium (n=16 and n=10) and 1 retrospective case study of neuroendocrine carcinoma of the endometrium (n=25) have been conducted [124]. The 2 studies investigating SCNEC of the endometrium were published over 20 years ago. Compared to these studies, the number of cases analyzed in this study is large. Additionally, in these past studies, a central pathologic review was not performed, nor were statistical analyses of prognosis, prognostic factors, and treatment regimens conducted.
In this study, both of the pathologists agreed that 64.6% of the registered cases had neuroendocrine carcinoma of the endometrium following a central pathological review. Due to the rarity, subtypes, and the difficulty in pathological diagnosis, cases reported as neuroendocrine carcinoma of the endometrium in the past may have included other histologic types. The central pathologic review used in this study ensures that the findings from this study were more reliable.
To clarify the clinicopathologic features of neuroendocrine carcinoma of the endometrium, we compared the distribution of the FIGO stage and the 5-year OS rates for each stage with those of grade 1 endometrioid carcinoma of the endometrium, the most common histologic type of the endometrium (Supplementary Table 4). It is noteworthy to mention that 69.0% cases had advanced FIGO stages (stage III and IV) among those with neuroendocrine carcinoma of the endometrium; this rate was clearly higher than that of grade 1 endometrioid carcinoma of the endometrium (15.1%). In the past reports, it was suggested that the key factor determining the prognosis of neuroendocrine carcinoma of the endometrium was the FIGO stage [102021]. In this study, OS was significantly decreased among cases with advanced (FIGO stage III and IV) versus early (FIGO stage I and II) stages (p=0.001). These findings are in agreement with those from past reports. The low 5-year OS rates in the cases of neuroendocrine carcinoma compared to those of grade 1 endometrioid carcinoma might be affected by the high prevalence of advanced FIGO stages. However, it should be noted that the FIGO stage was not a significant prognostic factor upon multivariate analysis in this study. We also hypothesized that the low 5-year OS rates might be affected by the high rates of hematogenous recurrence (Supplementary Table 3). The reason for the high prevalence of advanced FIGO stages in the cases of neuroendocrine carcinoma compared to those of grade 1 endometrioid carcinoma was unclear; in stage IV particularly, it might be affected by the clinicopathologic predisposing to hematogenous metastases of neuroendocrine carcinoma.
Previously, there were no reports that analyzed the relationship between prognosis and histologic subtypes for neuroendocrine carcinoma of the endometrium. In this study, pure type SCNEC cases had a significantly worse prognosis when compared to cases with other histologic subtypes (p<0.001). In this study, the rate of cases with advanced FIGO stages (stage III and IV) was higher among pure type SCNEC cases (Supplementary Table 2). It was thought that the poor prognosis of pure type SCNEC was associated with the high rate of cases with advanced stage disease. This finding also suggests that pure type SCNEC progresses more aggressively compared to other histologic subtypes. Additionally, it is important to note that upon multivariate analysis, which included FIGO stage and histologic subtypes, pure type cases had a significantly worse prognosis compared to mixed type cases. Generally, it has been hypothesized that, because the neuroendocrine carcinoma component is the most aggressive, pure type cancers progress more aggressively and have worse prognoses than mixed type cancers. However, in the digestive system (stomach, pancreas, colon, and rectum), the prognoses of pure poorly differentiated neuroendocrine carcinomas are not always worse compared to those of mixed neuroendocrine-non-neuroendocrine neoplasms [1718]. Therefore, the reason for pure type cases having significantly worse prognoses, compared to those of mixed type cases, is unknown.
With the exception of the histologic subtypes, only complete surgery was a significant prognostic factor upon multivariate analysis. Several studies have reported that debulking surgery improved the prognosis of endometrial cancer [22]. The National Comprehensive Cancer Network guideline recommends debulking surgery for endometrial cancer (both for type I and II, and also advanced stage cases), if possible [23]. Our study also suggests that complete surgery improves the prognosis of cases with early to advanced stage neuroendocrine carcinoma of the endometrium.
Despite its strengths, this study was subject to several limitations. First, there was insufficient statistical robustness due to the small number of included cases. If a larger number of cases had been analyzed, performance status, FIGO stage, and histologic subtypes (SCNEC, LCNEC) might have also been statistically significant prognostic factors upon multivariate analysis. Second, the effect of postoperative adjuvant chemotherapy on prognosis was not shown due to the insufficient statistical robustness. Kuji et al. reported the recurrence type and the effect of platinum-based postoperative chemotherapy on small cell carcinoma of the uterine cervix. In this study, it was reported that the most frequent recurrence type was hematogenous compared to lymphogenous or local recurrence, and platinum-based postoperative chemotherapy improved the prognosis of small cell carcinoma of the uterine cervix [24]. In our study, we observed a high rate of hematogenous recurrence compared to lymphogenous or local recurrence (Supplementary Table 3). Even though the effect of postoperative adjuvant chemotherapy on the prognosis could not be evaluated in our study, postoperative adjuvant chemotherapy should be performed for advanced stage cases due to the high rate of hematogenous recurrence. Further investigation is needed to clarify the effect of postoperative adjuvant chemotherapy on the prognosis of neuroendocrine carcinoma of the endometrium. Third, the effect of radiation therapy on prognosis was not evaluated in this study due to the small number of included cases. However, some patients with advanced stages or recurrence that were treated with radiation therapy experienced long-term survival, even though the effect on the prognosis was not evaluated. Two patients with a FIGO stage IV who had brain metastasis experienced long-term survival (144 and 88 months). These patients underwent resection of their brain tumors and received brain radiation therapy [12]. Additionally, 2 patients with recurrence in the pelvis experienced long-term survival (129 and 76 months). These patients were treated with pelvic radiation therapy and subsequent chemotherapy. Finally, unknown confounding factors that were not accounted for between surgery and prognosis (such as bulk and/or extent of tumors, metastatic sites, or patient's complications) may exist.
In conclusion, due to its low incidence and subtypes, standard treatment for neuroendocrine carcinoma of the endometrium has not been established. Nevertheless, our findings suggest that if complete surgery is expected to be achieved, clinicians should consider multidisciplinary therapy based on curative surgery not only for early stage cases, but also for cases in advanced stages in order to improve the prognosis of neuroendocrine carcinoma of the endometrium.
 XML Download
XML Download