

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
The Stafne bone cavity (SBC), first reported by Edward Stafne in 1942 [1], also called the static bone cavity, salivary inclusion cyst [2], latent cyst [3], and lingual bone defect [4], is an asymptomatic bony defect that is commonly located inferior to the mandibular canal and slightly above the inferior border of the mandible [15]. The reported incidence of the SBC ranges from 0.1% to 6.06% [56]. It is usually found on one side but occasionally, on both sides of the mandible [7]. The submandibular gland, fat tissue, connective tissue, lymphatic tissue, muscle or vessels have all been considered as potential contents of the SBC [4]. In the clinical setting, most SBC is found incidentally during panoramic radiography. Since the SBC is an asymptomatic bone cavity and does not require treatment, it is relatively rare to see the actual bony defect without radiographic images. Therefore, herein, we report a case of unilateral SBC in a cadaver.
Case Report
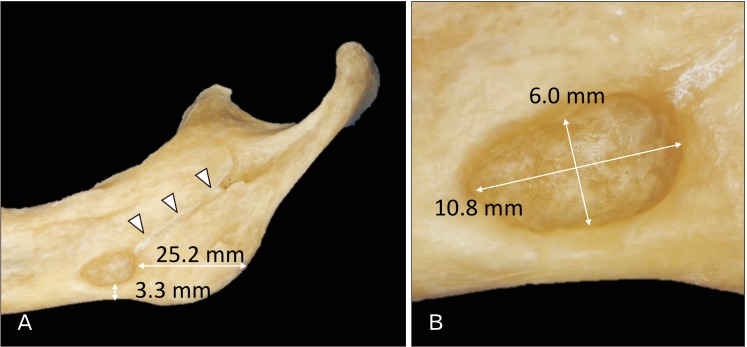
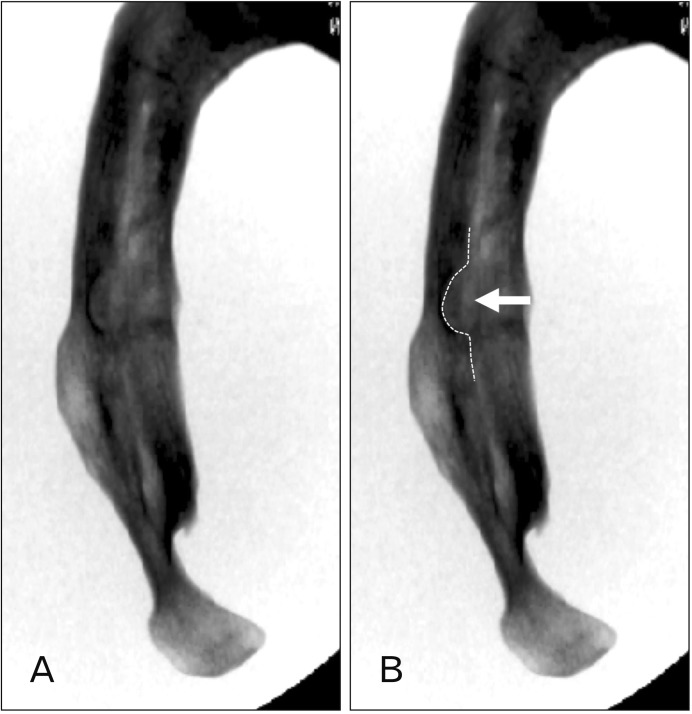
A 76-year-old at death male Caucasian cadaveric head (fresh-frozen) was dissected. During routine dissection of the head, the mandible was dissected, and the soft tissues of the mandible were removed. After the mandible was separated from the head, a large bony defect was found on the lingual surface of the right mandible, which was located 25.2 mm anterior to the angle of the mandible and 3.3 mm superior to the inferior border of the mandible. The shape and size of the bony defect was oval and 10.8×6.0 mm, respectively (Figs. 1, 2). The bony defect had a smooth surface and did not show any pathological condition. Therefore, it was determined to be an SBC. The SBC had continuity with the right mylohyoid groove. The depth of the SBC and width of the mandible at the SBC was 4.15 mm, 3.14 mm, respectively. The SBC was not observed on the left side.
Discussion
Studies on the SBC using dry mandibles were reported by Harvey and Noble in 1968 [7] and Kay in 1974 [8]. Since then, most of the reported studies examined either patients' panoramic radiography or computed tomography. The etiology of SBC is unclear. Many hypotheses exist regarding the cause of the bony defect, including a hypertrophic lobe of the submandibular gland, erosion by vascular compression [9], or incomplete Meckel cartilage ossification [9]. Minowa et al. [9] hypothesized that an SBC results from bone resorption or an overlying lipoma. In a case report by Kaya et al. [10], an ectopic parotid gland was found in the SBC. SBCs are most frequently found in patients over 50 years old [9] and there have been no reports of SBCs in patients younger than 10 years old [11]. On conventional panoramic radiographs, the SBC usually resembles a unilocular cystic lesion with well-defined borders. Multiple SBC was also reported by Aguiar et al. [12].
Histological examination by Harvey and Noble [7] revealed such bony defects did not invade the mandibular canal. However, the most recent study by Hisatomi et al. [13] demonstrated that an SBC in the premolar area might be misdiagnosed as a periapical lesion or odontogenic cyst. Thus, an SBC is occasionally not located inferior to the mandibular canal. Barker [14] also reported a case with an SBC situated on ascending ramus. An anthropological study conducted by Wasterlain and Silva [15] investigated ancient mandibles with an SBC. These SBC were most commonly situated below the third molar or inferior to the mylohyoid groove. In the present case, the mylohyoid groove had continuity with the SBC.
Even though the SBC is asymptomatic and does not require treatment, this anomaly should be taken into consideration by dentists and oral surgeon in order to avoid misdiagnosis.
 XML Download
XML Download