

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Venous drainage of the cerebrum is expertly modulated by highly complex superficial and the deep cerebral veins. These veins anastomose with each other and drain into the major dural venous sinuses such as superior sagittal (SSS), inferior sagittal, transverse (TS), cavernous (CS), and straight sinuses. All these sinuses ultimately drain into the internal jugular vein (IJV) [12].
The superficial middle cerebral vein (SMCV) is one of the superficial veins of the cerebrum that drains the venous blood from most of the superolateral surface of the brain. The SMCV lies in the posterior horn of the lateral sulcus, which further course along the lateral sulcus, pterion, lesser wing of sphenoid to drains into the CS [34]. Interestingly, with the help of many angiographic studies, several deviations from the normal course have been observed. The knowledge of these variant courses is vital so that different surgical approaches can be applied to prevent bleeding. The termination of the SMCV and its association with the skull base is imperative in the preoperative planning of the skull base surgery [3].
Studies in the past have focused on the variant pattern of the SMCV and attempted to classify the same. However, most of them were computed tomography (CT) angiography based studies [35]. Very few cadaveric studies on the variant pattern of the SMCV is available in the existing literature in adults and fetuses alike. Here in this study, we have made a sincere attempt to classify the various anatomical variations in the termination of SMCV in the termed fetus.
Materials and Methods
For the present study, 30 full-term fetuses (13 males and 17 females) obtained from the medical termination of pregnancies from the OBG department, Kasturba Medical College Manipal, were utilized. The crown rump length of the fetus was measured, the cranial cavity was dissected meticulously, and the dural venous sinuses were observed. The variation in the drainage pattern of the SMCV was noted and photographed. The SMCV was identified and classified based on its variability using a standard reference [3].
Results
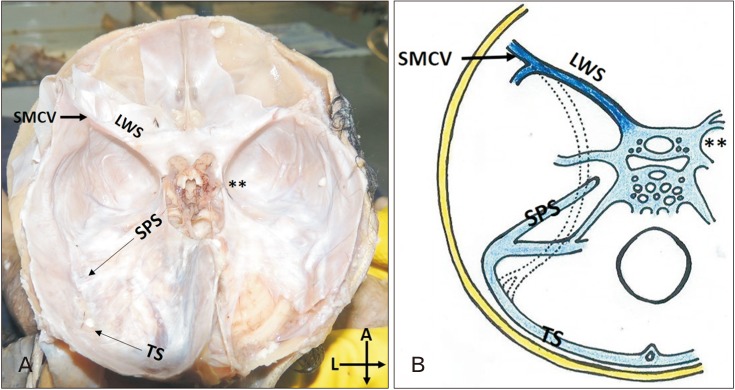
In the present study five specimens presented with variation in the pattern of the drainage of SMCV. Rest of the specimens had a typical presentation, i.e., sphenoparietal type as described previously (83.4%) (Fig. 1) [3]. The five cases fall into the two categories of the previously proposed classification, i.e., the superior petrosal (3 cases, 10%) and the basal type (2 cases, 6.6%). Interestingly in all the cases, the variations were seen on the left side.
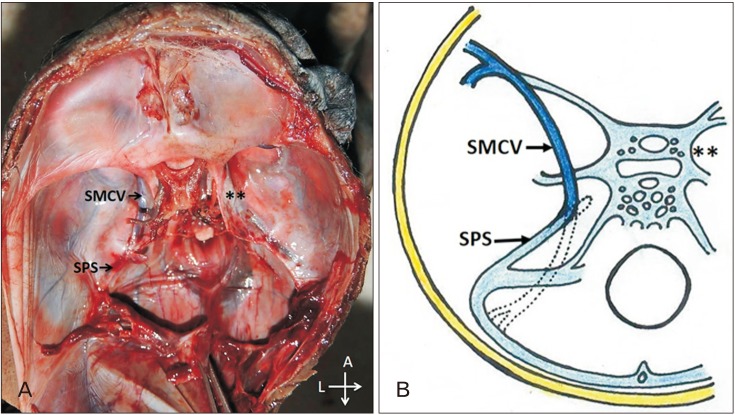
Case 1 (superior petrosal type)
The SMCV was coursing along the lesser wing of the sphenoid. It further passed downward and backward along the middle cranial fossa almost parallel to the CS to drain into the anterior end of the superior petrosal sinus (SPS) (Fig. 2).
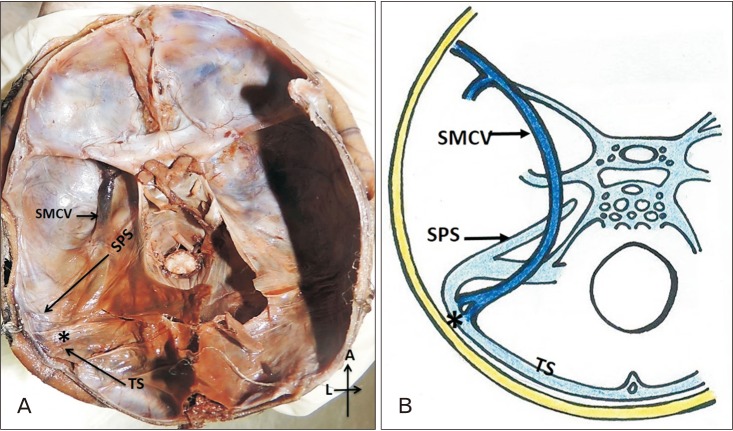
Case 2 (basal type)
The SMCV was passing along the Sylvian fissure and the lesser wing of the sphenoid (LWS). It then turned abruptly downwards and posteriorly along the middle cranial fossa, lateral to the CS. It later crossed the junction between TS and the Sigmoid Sinus and finally drained into the TS (Fig. 3). The communicating channels observed in these specimens were wider and more prominent than the other venous sinuses.
Discussion
A definitive venous pattern of the head and neck region develops in the first three months of prenatal life [67]. Two embryological sinuses, i.e., tentorial sinus and the prootic sinus take part in the formation of SMCV. Subsequent growth of cerebral hemisphere leads to elongation of the tentorial sinus. The SMCV is formed due to the medial shift of the anterior portion of the tentorial sinus into the CS. The segment of the tentorial sinus distal to it regress leading to the adult/definitive pattern of the SMCV. Fail in the medial shift/regression of the tentorial sinus results in the anomalous course and termination of SMCV [8].
The SMCV runs typically along the LWS bone and enters into the proximal SPS. However, San Millan Ruiz et al. [9] have raised a question regarding the drainage of the SMCV into the SPS in an anatomic study using an autopsied cadaver.
Suzuki and Matsumoto in 2000 [3] classified the drainage of SMCV into seven types based on embryological development or the remnant of the TS. The classification was done using a three-dimensional CT angiography and, 500 SMCVs were evaluated in 250 adult patients. The seven types included sphenoparietal (54%), cavernous (7%), emissary (12%), superior petrosal (2%), basal (2%), squamosal (2%), and underdeveloped (9%). It was not possible to confirm the drainage pattern in 8 % of the cases. 3% of the cases showed multiple drainage pathways as observed in their study [3]. In the present study in fetuses, only three types of the drainage pattern of the SMCV was observed, i.e., superior petrosal type in 10% and basal in 6.6% of the cases respectively. The remaining 83.4% of the cases were of the sphenoparietal type. The frequency of atypical SMCV's, i.e., superior petrosal and basal type was more in the fetuses as was observed in the present study unlike in the adults. The incidence of both types was rare/less in adults. It could be because the fetuses born with the types above may not survive postnatal.
The basal type of SMCV as observed in the present study results due to the persistence of the entire venous route of tentorial sinus. Thus the SMCVs routed via the sphenoparietal sinus and turned laterally along the floor of the middle cranial fossa, running along the petrous pyramid to terminate in the TS. The caudal regression of the primitive tentorial sinus is the result of the communication of the tentorial sinus to SPS leading to in superior petrosal type of the sinus [7].
A large rare squamousal type of vein running along the inner surface of temporal squama, connecting SMCV to into TS is reported by Kumar et al. in 2012 [8]. An unusual oblique sinus, which connected the right and the left TS was also reported previously [2].
In the dural arteriovenous fistulae (DAVF), the venous collaterals and venous rerouting help in the drainage of CS to the SPS, which then drains away into the cortical veins. These findings suggest that postnatal secondary anastomosis between the SPS or the TS and any possible remnant variations of the SMCVs could be a potential route of venous rerouting or collaterals in DAVFs [1011].
The basal type of venous drainage limits the temporal lobe mobility in the subtemporal approaches in neurosurgery. It is because the vein tightly adheres to the middle cranial fossa. In this situation, the collateral venous outflow patterns must be evaluated, and a different operative approach should be considered to reduce the likelihood of possible venous complications [12].
Gailloud et al. [13] performed a study on the termination pattern of SMCV. In their study, the SMCV was found to be absent in 19% of the cases. When present, they found the SMCV terminating directly into the CS in 20% of cases, the paracavernous sinus in 39% of cases, and the laterocavernous sinus in 22% of cases. Further, they also found that the paracavernous and laterocavernous sinuses drain into SPS in 33% and 18% of the cases respectively, which is the second most frequent type. Normally the paracavernous and laterocavernous sinuses drain into the pterygoid plexus [13].
The variation in the venous pattern as is observed in the present study in case of SMCV may also indicate the defective development of the IJV and the related venous sinuses. Identification of these variant veins is therefore essential in surgeries to avoid the dangerous catastrophic hemorrhage [14].
A variant of the SMCV mimicking an extra-axial hematoma has been reported. Herein the patient presented with an underdeveloped type of SMCV that was drained by a large venous channel into the SSS [1]. Variation in the course of SMCV should be considered and screened by angiogram before the surgery to reduce the risk during surgical procedures and the possibilities of post-operative edema [15].
Knowledge of the variations in the drainage of the SMCV as observed in the present study in fetal cadavers is essential for diagnosing several diseases involving the CS or paracavernous sinuses. It is also important in the correction of the lesions of the para-cavernous sinus and endovascular treatment of arteriovenous fistulas. The SMCV and SPS can serve as a venous refluxing route in patients with arteriovenous fistulas.
 XML Download
XML Download