

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The incidence of thyroid cancer has increased worldwide, for reasons that are not yet clear (1). In Korea, thyroid cancer was found in 2016 to be the third most common solid organ cancer and the second most common in women (2). The survival rate of patients with thyroid cancer, however, is generally good. Thyroid cancer mainly affects adolescents and young women aged 15–34 years (2), making cosmetic outcomes of thyroid surgery an important issue.
Open thyroidectomy, considered the standard thyroid surgery procedure (3), provides an adequate surgical view for all types of thyroid surgery but inevitably leaves a noticeable scar on the visible portion of the anterior neck. Some patients with dense or complicated neck scars have reported psychological and physical distress (45).
Remote access thyroid surgery approaches have been developed over the last 20 years to improve cosmetic outcomes (6). The bilateral axillo-breast approach (BABA) to endoscopic thyroid surgery, first reported in 2004 (7), has several advantages, including adequate access to both thyroid lobes, surgical safety comparable to that of open surgery, and excellent cosmetic outcome. However, the finite degrees of motion of rigid laparoscopic instruments has limited the ability to perform lymph node dissection during BABA endoscopic thyroid cancer surgery (8). To overcome this limitation, BABA thyroid surgery was combined with the Da Vinci robotic system in 2009. Over its 10 years of use, BABA robotic thyroid surgery has shown excellent cosmetic and oncologic outcomes (910111213). At present, the BABA method with the Da Vinci robotic system is used worldwide for robotic thyroid surgery (14). The present study reports the initial results in patients who underwent robotic BABA thyroidectomy with the Da Vinci Xi system at Inha University Hospital in Incheon, Korea.
MATERIALS AND METHODS
1. Patients
This study included 53 patients who underwent BABA robotic thyroidectomy, performed by a single endocrine surgeon using the Da Vinci Xi system, between December 2018 and March 2019. Indications for robotic BABA thyroidectomy included maximal tumor diameter <10 cm for benign tumors and <4 cm for malignant nodules; tumors not located near the tracheo-esophageal groove; no history of radiation of the neck or neck surgery; and absence of serious medical diseases or high risk of bleeding tendency. Patients' electronic medical records and surgical video clips were reviewed retrospectively.
Vocal cord function was evaluated by laryngeal ultrasound at the outpatient clinic. For more than 6 months after surgery, impaired mobility of vocal cord was considered permanent recurrent laryngeal nerve (RLN) injury. Transient RLN injury was regarded as recovered normal vocal cord mobility within 6 months of surgery. The serum intact parathyroid hormone (iPTH) test was performed on patients who underwent total thyroidectomy. Hypoparathyroidism was defined as a concentration of iPTH <10 pg/mL. The study protocol was approved by the Institutional Review Board of Inha University Hospital (IRB number: 2019-07-010). All statistical analyses were performed using SPSS version 19.0 software (IBM Corp., Armonk, NY, USA).
2. Surgical technique
Following induction of general anesthesia, the patient was placed in the supine position with neck extension, followed by endotracheal intubation with a NIM-3.0 neuromonitoring system (Medtronic Xomed, Jacksonville, FL, USA). After aseptic draping from the anterior neck to the breast and axillary area, a 1:200,000 solution of epinephrine in saline was injected into the subcutaneous layer (hydrodissection) around the destined flap area (Fig. 1A). Blunt dissection from the axillary area to the chest wall was initiated using the vascular tunneller, and the flap was extended from the anterior chest area to the neck. Da Vinci Xi trocars 8 mm in diameter were inserted through the axillary and breast incisions (Fig. 1B), followed by trimming of the flap elevation with an energy device, such as a Harmonic ACE® (Ehticon Endosurgery, Inc., Cincinnati, OH, USA) or LigaSure™ (Valleylab, Boulder, CO, USA). After flap elevation was completed, 4 robot arms were docked to the axillary and breast trocars. Robotic instruments used routinely included ProGrasp and LongBipolar forceps and Permanent Cautery Hooks. Tissue was dissected and vessels were sealed using Harmonic ACE Curved Shears or Vessel Sealer Extend. A neuromonitoring cable or monopolar coagulation cable for probing the nerve was connected to the Permanent Cautery Hook. During surgery, CO2 gas was supplied at 6–7 mmHg pressure and a flow rate of 10–15 L/min.
 | Fig. 1Flap design and insertion of trocars. (A) Flap design of bilateral axillo-breast approach. (B) The 8 mm trocars were inserted.
|
After docking the robot, the midline of strap muscle was divided and the isthmus was cut using an energy device (Fig. 2A). The isthmus was pulled to the opposite site of the thyroid lobe using ProGrasp, and the lateral side of the thyroid gland was divided from the strap muscle with middle thyroid vein ligation (Fig. 2B). The thyroid was retracted to the superior-medial side using the toggle control of robotic arms 3 and 4 (switching motion), and the level 6 area was exposed to identify the RLN (Fig. 2C). RLN identification was assisted by a neuromonitoring system connected to the Permanent Cautery Hook (Fig. 3D). The lower parathyroid gland was identified so that it could be saved by careful dissection (Fig. 2E). The thyroid gland was dissected from the trachea to the ligament of Berry (Fig. 2F). The superior pole of the thyroid was ligated with an energy device, preserving the superior parathyroid gland, followed by the completion of the lobectomy (Fig. 2G). Selected thyroid cancer patients also underwent ipsilateral central node dissection (Fig. 2H). The thyroid specimen was extracted through the left axillary port into a surgical vinyl bag. A Jackson–Pratt drainage tube was inserted through the left axillary port. The strap muscle was closed with Vicryl 3-0 continuous sutures, and skin incisions at the trocar sites were closed with Vicryl 4-0 intradermal sutures.
 | Fig. 2Procedures in robotic bilateral axillo-breast approach thyroidectomy. (A) Midline division and isthmectomy. (B) Divide the strap muscle from the thyroid gland. (C) Mobilization of thyroid lobe to superior-medial side (switching motion). (D) Identification of recurrent laryngeal nerve. (E) Saving lower parathyroid. (F) Thyroid was dissected from the trachea to Berry's ligament. (G) Ligation of superior pole with preservation of superior parathyroid. (H) Central node dissection.
|

RESULTS
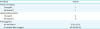
Table 1 shows the clinical characteristics of the 53 enrolled patients. These patients included 44 women and 9 men of mean age 44.51±10.36 years (range, 24–64 years) and mean body mass index 24.65±3.76 kg/m2. Preoperative fine needle aspiration cytology results showed that 44 nodules were malignant or suspected to be malignant. Twenty-five patients underwent lobectomy: 22 patients underwent lobectomy with ipsilateral central lymph node dissection, and 3 underwent lobectomy alone. Twenty-eight patients underwent total thyroidectomy: 27 patients underwent total thyroidectomy with central lymph node dissection, and 1 underwent total thyroidectomy alone. Mean operation time for flap creation was 19.03±5.49 minutes. Mean console times were 75.08±15.96 minutes for lobectomy and 93.53±17.86 minutes for total thyroidectomy. Estimated blood loss was 33.60±48.72 mL in patients who underwent lobectomy and 56.79±49.97 mL in patients who underwent total thyroidectomy. Mean hospital days after surgery was 3.65±1.03 days.
Table 1
Clinical characteristics of patients (n=53)

![]()
Pathologic findings are shown in Table 2. Of the 53 patients, 45 were diagnosed with classic type papillary thyroid carcinoma (PTC) and one with the follicular variant of PTC. Tumor diameters ranged from 0.3–3.7 cm for malignant nodules and 1.3–4.6 cm for benign nodules. The mean numbers of central lymph nodes harvested during lobectomy and total thyroidectomy were 2.00±1.96 and 5.36±4.42, respectively, and the mean numbers of metastatic central lymph nodes were 0.16±0.62 and 1.75±2.76, respectively.
Table 2
Pathological findings (n=53)

Values are presented as number or mean±standard deviation.
PTC = papillary thyroid cancer or [apillary thyroid microcarcinoma; FVPTC = follicular variant papillary thyroid cancer.
![]()
Table 3 shows surgical outcomes after robotic thyroid surgery. Only one patient developed vocal cord palsy after surgery, either transient and permanent palsy was occurred in same patient. Eight patients developed transient hypoparathyroidism, which resolved in all patients after 2 months. Serum concentrations of iPTH level were 15.21±15.21 pg/mL immediately after surgery and 24.49±20.24 pg/mL 2 months later. No patient required conversion to open surgery or experienced postoperative bleeding or injury to the trachea or esophagus. Three patients developed seromas that required aspiration treatment. Cosmetic results of robotic BABA thyroidectomy were excellent (Fig. 3).
DISCUSSION
The incidence of thyroid cancer has increased worldwide, especially among younger women at ages of social activity (1). Many surgical approaches have attempted to hide thyroidectomy scars far from the visible anterior neck (615). Endoscopic parathyroid resection was first reported in 1996 (16), and endoscopic thyroidectomy was first reported in 1997 (17). During that period, all endoscopic trocars were inserted through or around the neck. Although these methods still leave scars on the neck, and the number of scars increased, the scar size was reduced.
Remote access thyroid surgery using breast, transaxillary, and anterior chest approaches was introduced in 2000 (181920). The axillo-breast approach to endoscopic thyroidectomy was first introduced in 2003, and the BABA method was introduced in 2007 (721). The Da Vinci robot system was adopted for use in the BABA method, with the results first reported in 2009 (15).
The advantages of the robotic system for BABA thyroid surgery include a 15-fold magnified full 3-dimensional high definition surgical view, a view more detailed than that provided by endoscopic surgery. The intuitive articulation of robotic instruments enables a wider range of motion than the endoscopic approach, enabling both central and lateral lymph node dissection. Instrument movement speeds can be altered, making the surgery safer and more precise (13).
BABA robotic thyroidectomy has shown excellent outcomes over the last 10 years. Relative to conventional open surgery, robotic BABA thyroidectomy shows excellent cosmetic outcomes, as assessed objectively. Patients who undergo BABA robotic thyroid surgery show reduced psychological stress and improved quality of life compared with patients who undergo open thyroid surgery (5). Oncologically, BABA robotic thyroid surgery shows favorable surgical completeness, as estimated by stimulated thyroglobulin (Tg) level before radioactive iodine treatment. The proportion of patients with stimulated Tg levels <1.0 is reported to range from 65%–75% (2223). Moreover, BABA robotic thyroid surgery yields acceptable outcomes in patients with large size (>2 cm) cancers and in patients with Graves' disease. Moreover, this method enables lateral node (modified radical neck) dissection without altering surgical and oncologic safety (112425).
Incheon is located on the west coast of the Korean Peninsula and is the third most populous city (3 million people) in South Korea. To date, no hospital in Incheon had performed BABA robotic thyroid surgery. This study is the first to describe robotic BABA thyroidectomy with the Da Vinci Xi system in Incheon. None of our patients experienced severe complications, such as RLN injury or permanent hypoparathyroidism (Tables 2 and 3). The only patient with RLN injury had a thyroid cancer that had firmly infiltrated into the nerve. Compared with previous reports of robotic BABA surgery, with mean operation times ranging from 142–228.75 minutes, our operation times were relatively short: 93.60±15.12 minutes for lobectomy and 113.03±18.92 minutes for total thyroidectomy (26). The shorter operation time in our study may have been due to the experience of the surgeon, who had about 4 years of BABA training at the center that introduced this method before transfer to Inha University Hospital. In addition, the robotic system used by our hospital is the Da Vinci Xi system, the latest to be developed. This system has several advantages over the previous Da Vinci S and Si systems. For example, the diameter of all robotic trocars in the Da Vinci Xi was 8 mm, allowing changes in instruments and cameras on robotic arms during surgery. By comparison, the Da Vinci S and Si systems require one 12 mm trocar due to the large diameter of the robotic camera. More steps are therefore required to move the camera to another site. Moreover, smaller trocars require smaller breast incisions and yield better cosmetic outcomes. The Da Vinci Xi system also enables the installation of new robotic equipment that is not supported by the previous versions.
In summary, the introduction of robotic BABA thyroid surgery with the Da Vinci Xi system at our institution was successful, with no severe complications. Because this report includes a relatively small number of patients who underwent surgery over a relatively short 3-month period, prospective studies of large numbers of patients and comparisons with open and other types of endoscopic surgery are required.
 XML Download
XML Download