

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Papillary thyroid microcarcinoma (PTMC) is a form of papillary thyroid carcinoma (PTC) <1 cm in size with a good postoperative prognosis. Most patients who develop PTMC do not exhibit any clinical symptoms, and the progression is very slow. Active surveillance is therefore necessary in combination with immediate surgical intervention (12). However, despite the need for regular screening, the biological features of PTMC remain poorly understood, with few markers available to predict long-term prognosis and few appropriate follow-up criteria for use with patients with this condition.
To date, the most common treatment method for PTMC is surgery. A definitive correlation between the surgical method and clinical prognosis of PTMC has not yet been established (3). Bilateral total thyroidectomy was long the preferred method because it enables better maintenance of normal thyroid function and reduces the risk of recurrence (4). However, due to the increased incidence of adverse effects after bilateral total thyroidectomy, unilateral thyroid lobectomy (UTL) may be preferred as a conservative treatment modality in the absence of known risk factors for recurrence (extrathyroidal extension, lymph node metastasis or distant metastasis, unfavorable histology, familial history of thyroid cancer, or previous radiation exposure), even in cases with a larger tumor size (1–4 cm) (5).
Post-UTL hypothyroidism is unpredictable, occurring in 11%–43% of cases (6). This rate varies due to the diverse definitions of hypothyroidism, duration of follow-up, study population, and interventional techniques (7). As hypothyroidism requires long-term follow-up and thyroid hormone replacement, several studies have been conducted to identify factors predicting the need for thyroid hormone therapy. This is particularly true in the case of thyroid-stimulating hormone (TSH) suppression, which is the indication for continuing thyroid hormone therapy after UTL. Among patients deemed at high-risk of adverse effects after surgery, a TSH level <0.1 mIU/L was reported to improve prognosis in the case of TSH suppression (8). In contrast, the impact of TSH suppression on disease prognosis in low-risk patients remains unclear.
Several studies have been conducted on patients at our institution who experienced hypothyroidism after UTL. One study analyzed the predictive factors for levothyroxine discontinuation after immediate initiation of thyroxine replacement therapy in patients who did not undergo postoperative thyroid function tests after UTL (9), and the other evaluated the optimal timing of discontinuing levothyroxine supplementation (10). Unlike these earlier studies, this study aimed to evaluate risk factors for developing hypothyroidism in patients who did not receive perioperative levothyroxine treatment, by analyzing thyroid function before and after UTL in PTMC patients.
MATERIALS AND METHODS
1. Study population
A total of 232 patients were treated for PTMC between January 2015 and December 2017, of whom 40 were excluded due to treatment for thyroid disease (n=22) or an inability to maintain normal thyroid function during the preoperative examination (n=18). Thus, the final cohort consisted of 192 patients who were able to undergo regular postoperative thyroid function tests at least four times a year. Our Institutional Review Board (IRB) approved this retrospective study and waived the need for informed consent due to the retrospective nature of this study (IRB-2017-03-0003).
Patients with thyroid disease who received preoperative medications were diagnosed with subclinical hypothyroidism (n=11), hypothyroidism (n=9), or hyperthyroidism (n=2). Among the patients who had thyroid dysfunction but were not on medication prior to surgery, 16 were diagnosed with hypothyroidism and 2 with hyperthyroidism.
2. Serological and histopathological evaluations
We assessed the preoperative levels of free T4 (reference range [RR]: 0.93–1.71 ng/dL), TSH (RR: 0.27–4.20 mIU/L), thyroglobulin (TG; RR: 1.4–78 ng/dL), anti-thyroid peroxidase (anti-TPO) antibodies (RR: <5.61 IU/mL), and anti-TG antibodies (RR: <4.11 IU/mL). Positive results were defined as an anti-TPO level of ≥5.61 IU/mL or anti-TG level of ≥4.11 IU/mL. A patient with at least one positive antibody test result was considered positive for thyroid autoantibodies. All serological parameters were measured by electrochemiluminescence immunoassays using the Elecsys® automatic system (Roche Diagnostics Deutschland GmbH, Mannheim, Germany).
Patients were classified as either having normal thyroid function, Hashimoto thyroiditis, non-Hashimoto lymphocytic thyroiditis, Graves' disease, or diffuse hyperplasia based on the histopathological results.
The volume of the residual thyroid gland was retrospectively measured using an image-archiving and communication system and calculated based on the measurements obtained by ultrasonography using the following equation according to the ellipsoid method: V = π/6 × (lobe length [cm]) × (lobe width [cm]) × (lobe depth [cm]). Body mass index (BMI) was calculated based on the height and weight of the patients. Commonly accepted BMI ranges are as follows: <18.5 kg/m2 (underweight), 18.5–25 kg/m2 (normal weight), 25–30 kg/m2 (overweight), >30 kg/m2 (obese) (11).
3. Surgery and levothyroxine replacement therapy
UTL was performed by preserving the contralateral lobe isthmus of the thyroid gland. All surgeries were performed by a single surgeon who performs >100 conventional open, endoscopic, and robot-assisted surgeries per year. Our hospital does not provide immediate levothyroxine replacement therapy after UTL. During the first 12 months after UTL, each patient's serum TSH levels are measured at 1, 3, and 6 months, and then every 12 months thereafter. Postoperative hypothyroidism was defined as a TSH level ≥4.20 mIU/L (RR: 0.27–4.20 mIU/L).
Levothyroxine discontinuation is considered successful if the patient exhibits normal TSH levels without thyroid hormone treatment 1 year after UTL. In cases in which normal TSH levels were not successfully maintained during the study period, levothyroxine therapy was initiated immediately.
4. Statistical analysis
Postoperative hypothyroidism and clinicopathological characteristics were compared according to whether levothyroxine replacement was performed or not, using the χ2 test for categorical variables and independent t-test for continuous variables. Univariate logistic regression analyses were initially conducted to evaluate the predictive power of individual parameters. The parameters were selected and included in the binary logistic regression analysis to determine an optimal logistic regression model for predicting the response to levothyroxine replacement. The results are presented as odds ratios with corresponding 95% confidence intervals (CIs) and P values using the Wald test. The cut-off value of continuous variables for predicting the development of hypothyroidism was determined using a receiver operating characteristic curve. All statistical analyses were conducted using SPSS version 21.0 (SPSS Inc., Chicago, IL, USA). P values <0.05 were considered statistically significant.
RESULTS
Of the 192 patients included in this study, 97 maintained normal thyroid function without levothyroxine replacement during the study period, whereas the remaining 95 failed to maintain normal thyroid function and thus were treated with levothyroxine. Clinical characteristics including sex, age, preoperative free T4, TSH, TG, thyroid autoantibodies (anti-TG and anti-TPO), BMI, postoperative thyroid gland histopathology, and remnant thyroid gland volume of the patients are summarized in Table 1. Male sex, low preoperative TSH level, and normal parenchyma of the thyroid gland were significant factors for maintaining normal thyroid function after surgery, suggesting that levothyroxine replacement is not necessary in these patients. No other parameters showed statistically significant differences between the patients who did and those who did not maintain normal thyroid patient.
Table 1
The relationships of the individual parameters according to postoperative euthyroidism and hypothyroidism

Values are presented as mean±standard deviation (range) or number (%).
TSH = thyroid-stimulating hormone; TG = thyroglobulin; BMI = body mass index; HT = Hashimoto's thyroiditis; CLT = chronic lymphocytic thyroiditis.
![]()
In the multivariate logistic regression analysis, sex and the preoperative TSH level were significantly associated with postoperative euthyroidism (P<0.05). The cut-off value of the preoperative TSH level for predicting maintenance of normal thyroid function after UTL was 1.89 mIU/L, with an area under the curve of 0.657 (95% CI, 0.585–0.724, P<0.001), sensitivity of 62.8%, and specificity of 65.7% (Fig. 1). Patients with a preoperative TSH level >1.89 mIU/L were 5.76 times more likely to require levothyroxine replacement therapy (Table 2).
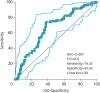 | Fig. 1Receiver operating characteristic curves for cut-off value of preoperative thyroid-stimulating hormone levels occurred postoperative hypothyroidism among 192 papillary thyroid microcarcinoma.AUC = area under the curve.
|
Table 2
Univariate and multivariate analysis for the development of hypothyroidism

OR = odds ratio; CI = confidence interval; TSH = thyroid-stimulating hormone.
*Underlying thyroid disease include subclinical hypothyroidism, hypothyroidism, and hyperthyroidism.
![]()
DISCUSSION
PTMC is less invasive than PTC and has a better prognosis compared with other thyroid tumors due to the very low rates of associated mortality, local recurrence, and distant metastasis. UTL is an acceptable surgery for low-risk patients who have a single lesion localized within the thyroid gland, with no evidence of metastasis to the surrounding cervical lymph nodes.
Postoperative hypothyroidism after UTL usually occurs within 6 months to 1 year after surgery and is diagnosed based on the TSH level. Reported incidence rates of hypothyroidism after UTL range from 11% to 44% (121314). In this study, 49.5% of the patients who did not receive thyroid hormone replacement experienced asymptomatic or clinical hypothyroidism with elevated TSH levels. This overall incidence is therefore similar to that reported in previous studies.
For low-risk patients whose thyroid cancer is not detected clinically and is regarded as unlikely to recur, it is recommended to maintain TSH levels between 0.10 and 0.50 mIU/L using levothyroxine replacement as the postoperative TSH suppression therapy. Ideally, TSH values should be maintained between 0.3 and 2.0 mIU/L for longer follow-up (15). High-risk patients with PTC showed a good prognosis when their TSH level was maintained below 0.1 mIU/L; however, the advantage of TSH suppression therapy in low-risk patients has not yet been established. This poor understanding of TSH levels in low-risk thyroid cancer patients after thyroid lobectomy is primarily due to the lack of focus on the optimal TSH level or T4 dose (815). Without consideration of spontaneous recovery of postoperative hypothyroidism, thyroid hormone replacement therapy is performed on subclinical hypothyroidism patients with a mildly elevated TSH level (7). The adverse effects of subclinical thyroid disorders on both the cardiovascular and skeletal systems have also been shown to be greater than expected (16). To our knowledge, there are no established guidelines on the time of initiation or cessation of thyroid hormone replacement therapy. Recently, our institution reported the preoperative TSH level as a risk factor for postoperative hypothyroidism in PTMC patients who underwent immediate levothyroxine replacement after UTL (9). As the rates of maintaining normal postoperative thyroid function reported in previous studies (58%, 91/157) are similar to those reported here (50.5%, 97/192), we believe that the immediate initiation or non-initiation of thyroid hormone replacement after lobectomy is selective.
In general, the known factors associated with postoperative hypothyroidism are the preoperative TSH level, histopathology indicative of chronic lymphocytic infiltration, presence of thyroid autoantibodies, remnant thyroid volume, preoperative free T4 level, and patient age (6717). In this study, 49.5% (95/192) of patients required levothyroxine replacement due to an inability to maintain euthyroidism after UTL, whereas 50.5% maintained euthyroidism without levothyroxine replacement. These results were similar to those reported in previous studies (42.0%), in which patients whose levothyroxine was discontinued after initial treatment without monitoring thyroid function. However, unlike previous studies that reported the preoperative TSH level as the only significant predictor of postoperative hypothyroidism, both sex and histopathology of the thyroid gland were identified as key components in maintaining normal thyroid function postoperatively in this study. A preoperative TSH level <1.89 mIU/L, as measured by Receiver Operating Characteristic curve, was significantly associated with successful maintenance of normal postoperative thyroid function. This finding is consistent with the results of previous studies (67). Therefore, a high TSH level, the most influential factor in postoperative hypothyroid function, is the most useful factor for postoperative management and function prediction in low-risk PTMC patients. The potential risk of postoperative hypothyroidism based on TSH levels should therefore be discussed with patients before surgery.
In this study, histologically normal thyroid parenchyma and male sex were significantly associated with normal postoperative thyroid function without levothyroxine replacement. Previous literature has suggested that thyroid autoantibodies and lymphatic infiltration are key components in the maintenance of normal thyroid function. Thyroid autoantibodies have been reported to cause postoperative hypothyroidism (1417); however, no significant association was found in this study. In addition, lymphocytic thyroiditis or autoimmune thyroiditis causes hypothyroidism (1718). Therefore, patients with a normal parenchymal thyroid gland are more likely to exhibit normal postoperative thyroid function than are those with autoimmune thyroiditis. Most of the thyroid diseases that cause hypothyroidism are more common in women than in men (19). This is consistent with our finding that male sex is a significant factor in maintaining normal postoperative thyroid function.
This study has some limitations. First, the follow-up period of this study was relatively short (<1 year). Our findings were not consistent with those of previous studies, suggesting that the longer the follow-up period, the greater the likelihood of recovering sufficient thyroid function and a lower TSH level in some patients. Second, there is no information on the potential risk factors (iodine intake, lymphocyte infiltration grade, etc.) for hypothyroidism after UTL, as the data were obtained retrospectively. Third, few patients attempted to discontinue levothyroxine treatment within the first year of treatment (n=10), and no patient attempted to discontinue levothyroxine treatment more than twice during the study period.
CONCLUSION
Our study showed that 50.5% (97/192) of patients maintained normal thyroid function without the need for levothyroxine replacement after UTL, whereas the remaining 49.5% (95/192) required levothyroxine therapy to maintain euthyroidism. Female sex and a higher preoperative TSH level were identified as independent predictors of the development of postoperative hypothyroidism. The cut-off preoperative TSH level for predicting maintenance of normal thyroid function after UTL was 1.89 mIU/L in this study. For those patients with a high TSH level, which is the most influential factor in postoperative hypothyroid function, the potential risk of postoperative hypothyroidism should be discussed with patients before surgery.
 XML Download
XML Download