

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Almost half of the pregnant women experience pain in the lumbar, and/or sacroiliac area, and/or symphysis pubis during pregnancy and following childbirth.1 Ankylosing spondylitis (AS) affects the sacroiliac joints and commonly occurs in the reproductive age; therefore, many studies have been conducted to evaluate disease activity during and following pregnancy. Reportedly, patients with AS showed higher back pain scores during pregnancy than healthy individuals; however, the pain was less severe in the 1st trimester than before pregnancy in women with AS.2 Moreover, disease activity was stable during pregnancy, although majority of the women with AS experienced a flare-up during the first 6 months following delivery.345 In contrast, in a previous study, disease activity was the highest in the 2nd trimester and stable in the year following delivery.6 Radiologic progression in 4 patients with AS a minimum of 2.5 years following pregnancy and childbirth has been reported.4 However, there are limited reports on the effects of pregnancy on AS course including non-pregnant AS patients as controls.
The sacroiliac joint is not a part of the pelvic inlet during delivery; however, the rate of cesarean section (CS) is higher in women with AS than in healthy women,78 which may be related to disease activity. However, the tendency to perform CS in women with inflammatory joint diseases should be considered.9
Limited studies have focused on whether vaginal delivery (VD) is more likely to affect AS course than CS. Therefore, the present study aimed to examine the effects of pregnancy and delivery methods on AS management using the Korean Health Insurance Review and Assessment Service (HIRA) claims database.
METHODS
Study design and data source
We conducted a population-based retrospective cohort study using patient records extracted from the HIRA claims database. HIRA includes all health-related information of around 50,000,000 individuals in the entire Korean population covered by the National Health Insurance program.10
Study subjects
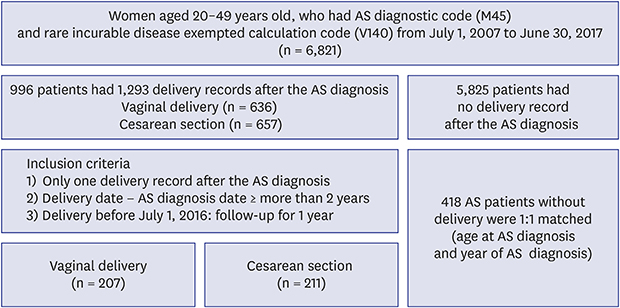
Women aged 20–49 years who were diagnosed with AS (International Classification of Disease and Related Health Problems, 10th revision [ICD-10] M45) and listed in the Korean rare intractable diseases (RID) system between July 1, 2007, and June 30, 2017 were included (Fig. 1). In Korean RID system, AS is diagnosed based on the 1984 Modified New York criteria that comprise the radiographic evidence of sacroiliitis and clinical symptoms.11 We excluded the women AS without RID codes for diagnostic validation. The subjects were classified into 2 groups: AS patients with delivery or without delivery. Women with AS without delivery records within the study period were classified in the without delivery group. Furthermore, each delivery was categorized by the method of delivery: VD and CS. Women with a history of only one delivery following AS diagnosis were included in the delivery group; this was because a second delivery may require a more conservative management. In addition, the study cohort was restricted to subjects who were diagnosed with AS at least 2 years before delivery, as the prescription of AS medications may be affected by pregnancy. Therefore, 2 time periods—before (−730 to −365 days) and after (0 to 365 days) delivery—were examined (Fig. 2). The index date was defined as the date of delivery in the delivery group and matched by the age at AS diagnosis and year of AS diagnosis in the without delivery group. Women with AS for whom no information was available on the prescription patterns before and after delivery were excluded.

AS medications and change in prescription
AS medications included oral non-steroidal anti-inflammatory drugs (NSAIDs), oral corticosteroids, disease modifying anti-rheumatic drugs (DMARDs; including methotrexate and sulfasalazine), and tumor necrosis factor (TNF) inhibitors. The proportion of days covered (PDC) was selected as an index to assess the treatment adherence to NSAIDs and corticosteroids. PDC was defined as the total number of medication-covered days divided by each observation time period (365 days). Adherence was classified as follows: PDC ≥ 0.7 as regular use and PDC < 0.7 as on demand.12
Change in prescription was defined as follows. If a patient 1) initiated the use of new corticosteroids, regular NSAIDs, DMARDs, or TNF inhibitors; 2) received increased mean prescribed daily dose of oral corticosteroids considered equivalent doses; or 3) received increased mean prescribed daily dose of the same generic NSAID or DMARD between the 2 time periods.
Statistical analyses
All statistical analyses were performed using SAS Enterprise Guide software (version 6.1; SAS Institute, Inc., Cary, NC, USA). Characteristics of AS patient, including age, comorbidities, and medications, were analyzed. Categorical and continuous variables were presented as numbers with percentages and median with interquartile range, respectively. Change in prescription was compared between the AS patient with delivery group and without delivery group using a generalized linear model with a binomial distribution to account for the matched nature of the data. And we also assessed the risk of altering prescribing patterns by delivery method using a generalized linear model with binomial distribution. Multivariable analysis was performed to determine the probability of change in prescription between the 2 groups after adjusting for potential confounders. To assess confounders, univariate analyses were performed independently for the presence of each comorbidity and age group. All variables with P < 0.1 in the univariate analysis were included in multivariable analysis, and backward elimination was performed. Results were reported using adjusted odds ratios (ORs) and their 95% confidence intervals (CIs). P < 0.05 was considered statistically significant.
Ethics statement
This study fulfilled the ethical guidelines of the Declaration of Helsinki. The requirement for informed consent was waived by the Institutional Review Board (IRB) because of the retrospective nature of the study using a database. The waiver from IRB was certified by Asan Medical Center (No. 2017-0431).
RESULTS
Baseline characteristics of AS patients with and without delivery
There were 6,821 fertile women with AS in the Korean cohort, of which 996 had 1,293 delivery records and 5,825 had no delivery records between July 1, 2007, and June 30, 2017 (Fig. 1). AS patients in the delivery group were younger; showed less comorbidities including hypertension, diabetes mellitus, and renal insufficiency at AS diagnosis; and were exposed to fewer AS medications except corticosteroid and DMARDs in a year following AS diagnosis than AS patients in the no delivery group (Table 1). To comparing of altering prescribing patterns between AS patients with and without delivery, 418 women with delivery once after diagnosis of AS were included. Among 5,825 women with AS without delivery code, 418 patients were matched by the age at AS diagnosis and year of AS diagnosis (Fig. 1). After matching, age at AS diagnosis, duration of AS, and comorbidities, except inflammatory bowel disease (IBD), were similar between the 2 groups (Table 1).
Table 1
Baseline characteristics of patients with AS with and without delivery

Data are presented as number (%).
AS = ankylosing spondylitis, NE = not estimated, IBD = inflammatory bowel disease, NSAIDs = non-steroid anti-inflammatory drugs, PDC = proportion of days covered, DMARDs = disease modifying anti-rheumatic diseases, TNF = tumor necrosis factor.
aP value was estimated by χ2 test or Fisher's exact test; bStandardized difference. Standardized difference < 0.1 indicated a negligible difference; cAt AS diagnosis ± 180 days; dAfter 365 days of AS diagnosis.
![]()
Change in prescription in AS patients with and without delivery
AS patients in the delivery group showed lower probability of requiring regular use of new NSAIDs or increased dose of NSAIDs (Table 2). However, overall rate of change in prescription was comparable between the delivery and no delivery groups (OR, 0.74; 95% CI, 0.54–1.01). The result was similar following adjustment for uveitis, IBD and psoriasis (OR, 0.76; 95% CI, 0.56–1.05).
Table 2
Alteration of prescription patterns after delivery in AS according to delivery after 1:1 matching

Data are presented as number (%).
AS = ankylosing spondylitis, OR = odds ratio, aOR = adjusted odds ratio, CI = confidence interval, NSAIDs = non-steroid anti-inflammatory drugs, DMARDs = disease modifying anti-rheumatic drugs, TNF = tumor necrosis factor.
aOR of change in prescription patterns compared between 2 groups using a generalized linear model with binomial distribution to account for the matched nature of the data (reference group: without delivery group); bAdjusted for the presence of uveitis, inflammatory bowel disease, or psoriasis.
![]()
Change in prescription following delivery according to the delivery method
Among the 418 AS patients in the delivery group, 211 patients (50.5%) underwent CS. The frequency of overall change in prescription was similar between CS and VD (OR, 0.68; 95% CI, 0.43–1.06) (Table 3). Similar trends were observed even after adjustments for age and the presence of uveitis, IBD, or psoriasis (OR, 0.72; 95% CI, 0.45–1.14). AS patients with VD showed a lower tendency of requiring the regular use of NSAIDs or increase in the dose of NSAIDs (OR, 0.50; 95% CI, 0.25–1.00), although the difference was not significant following adjustments for age and the presence of uveitis, IBD, or psoriasis.
Table 3
Alteration of prescription patterns after delivery in AS according to delivery method

Data are presented as number (%).
AS = ankylosing spondylitis, VD = vaginal delivery, OR = odds ratio, aOR = adjusted odds ratio, CI = confidence interval, NSAIDs = non-steroid anti-inflammatory drugs, DMARDs = disease modifying anti-rheumatic drugs, TNF = tumor necrosis factor.
aOR of change in prescription compared between 2 groups using a generalized linear model with binomial distribution (reference group: cesarean section); bAdjusted for the presence of uveitis, inflammatory bowel disease, or psoriasis.
![]()
DISCUSSION
In this population-based retrospective comparative study, the rate of change in prescription was comparable between AS patients with delivery and without delivery. Furthermore, the method of delivery was not associated with increased probability of change in prescription, suggesting negligible effects of VD on AS worsening.
In previous studies, majority of the AS patients experienced aggravated disease activity during pregnancy31314 and flare-up during 6 months following delivery, although this was considered a temporary flare-up associated with the increased physical stress of parturition and care for a newborn.4515 Furthermore, a recent prospective study has reported stable AS activity 1 year following delivery.6 Similarly, a previous case–control study has shown that the postpartum pain scores in AS returned to the baseline pre-pregnancy levels; therefore, pregnancy did not aggravate AS activity.2 In the present study, the 1:1 ratio with the control group matched in terms of age at and year of AS diagnosis was used, and change in AS management was assessed. According to the recommendations of European League Against Rheumatism-Assessment of Spondyloarthritis International Society (EULAR-ASAS),16 NSAIDs are recommended as the first-line treatment for AS patients with pain or stiffness and DMARDs, including sulfasalazine or methotrexate, are recommended for patients with peripheral arthritis. Although long-term corticosteroids use is discouraged, short-term corticosteroid use is effective in patients with axial symptoms. The use of TNF inhibitors should be considered in patients with persistently high disease activity despite conventional treatment. Based on this recommendation, using new NSAIDs, DMARDs, corticosteroids, and TNF inhibitors or increasing the doses of NSIAIDs, DMARDs, or corticosteroids may reflect a worsening disease. Change in prescription was noted in 24.9% (104/418) of the patients 1 year after delivery, and similar rate was noted in the no delivery group (30.9%; 129/418). To the best of our knowledge, this is the first study comparing change in prescription between AS patients with and without delivery, and our result provide evidence that may offer assurance to women with AS planning pregnancy.
Previous studies have shown that women with AS show a higher risk of CS than healthy women.78 Furthermore, the rate of elective CS was higher than that of emergent CS in women with AS, although the indications for CS were comparable. In the present study, the rate of CS (50.5%) in women with AS was higher than that in the general Korean women population.17 Although, we could not distinguish elective CS from emergent based on the HIRA database, concerns regarding the possibility of disease aggravation following delivery should be considered among women with AS when selecting the delivery method. In the present study, VD was not associated with increased probability of change in prescription. The sacroiliac joint is not a part of the pelvic inlet and is not mechanically inherent during delivery, which may explain why VD was not associated with change in AS management. Indeed, according to the core set of recommendations for patients with AS, CS is not required in women with sacroiliac joint fusion or hip joint replacement.18 Based on this result, it is recommended that pregnant women with AS opt for VD if they are concerned about disease course without any other indication for CS.
The present study has some limitations. First, change in prescription could not directly reflect a worsened disease. Second, change in prescription was compared at only 2 time periods (1–2 years before delivery and 1 year after delivery). The period 2 years before delivery was selected to avoid the bias of change in medications for planning a pregnancy; however, the period 1 year after delivery may be affected by confounders including breast feeding and may be relatively short to evaluate the effects of pregnancy and delivery. Third, although we conducted study using a nationwide database, few events were detected, and there were no significant differences in the evaluated parameters as the power of analysis was considerably low. Finally, the accessibility of medical services during prenatal periods differs with regions19; thus, the place of residence could be a confounding factor for change in prescription. Despite these limitations, this is the first study to compare change in AS treatment according to pregnancy and delivery methods.
In conclusion, the rate of change in prescription was comparable in AS patients with delivery and without delivery, and the method of delivery was not associated with change in prescription. Thus, pregnancy and delivery method do not contribute to change in treatment after delivery in women with AS, and pregnancy and VD may be encouraged in women with AS who are concerned of AS worsening.
 XML Download
XML Download