

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Breast cancer is among the most common malignancies that affect both humans and dogs. Both species have remarkably similar natural histories, and the patient can die from metastatic disease if not treated effectively [1]. Canine mammary tumors (CMTs) have been characterized extensively, as a comparative model of human breast cancers, and have been shown to have similar genetic defects and phenotypes including hormone-dependence, similar malignant tissue types, and natural history [2345678910].
Cancer cells express selective antigens that are recognized frequently by the immune system and in some cases can promote natural remission of the tumor [11121314]. The formation of hybrid-cell vaccines that are produced through the fusion of antigen presenting cells (APCs) with tumor cells, have been used to successfully exploit this natural defense using the mechanisms required for antigen presentation to express tumor antigens [15161718]. T-cell activation is achievable if vaccines are autologous and major histocompatibility complex (MHC) I matched, particularly if dendritic cells (DCs) are used for antigen presentation due to their expression of MHC class I and class II molecules and necessary co-stimulatory and adhesion molecules [151617181920]. Attempts to develop such hybrid-cell vaccine strategies in human patients have had mixed success in improving the management of disease but have demonstrated improved immune recognition and fewer adverse effects [1521222324]. Poor responses may be due to the inadequate antigen presentation or suboptimal sources of antigens or may be due to the aggressive immune suppression of autoimmunity by regulatory T cells (Tregs) [25262728]. Such challenges are difficult to overcome in human patients when moving directly from a mouse model because of the significant differences in biology, genetics, and natural history [29]. A more similar intermediate model of spontaneous breast cancer in canine patients with an intact immune system would provide a better system for developing such therapies [293031].
Enhanced immune recognition by vaccination with allogeneic hybrid-cell fusions of antigen presenting cells and tumor cells as well as autologous DCs fused to unmatched CMT cells have been reported [34]. Although the mechanisms for antigen presentation in this vaccine are not well described, cross-presentation between allogeneic CMTs and autologous DCs may be responsible [1824]. The high-speed sorting technology for the isolation of low frequency circulating canine DCs from the peripheral blood developed previously has provided antigen presenting cell populations suitable for constructing patient-specific autologous hybrid-cell fusion vaccines [4].
This paper reports a preliminary precision medicine strategy composed of the fusion of CMT cells and primary DC-enriched populations sorted from individual canine patient peripheral blood to construct individualized autologous hybrid-cell fusions and their use as living cancer vaccines in canine patients.
MATERIALS AND METHODS
Mammary cancer patients
Clinical and pathological data were collected for canine mammary cancer patients involved after admission to the Auburn University Small Animal Teaching Hospital. The inclusion criteria were a diagnosis of grade 1–3 mammary carcinoma confirmed by the histopathology, no history of previous treatment or disease, no evidence of metastatic disease, and a minimum weight of 6 kg [35]. All patients were treated with a surgical resection, and the biopsies were analyzed by a board certified veterinary pathologist (E.G.M.R.). All owners were offered the same treatment benefits and cost reduction regardless of the treatment group. The overall survival (time to death) and cause of death, if known, were recorded. The breast cancer phenotype was determined as described previously [33]. Follow-up data were collected from the clinical records and direct contact with the owners. This project was approved by, and conducted under the oversight of, the Auburn University College of Veterinary Medicine Clinical Research Review Committee and the Auburn University Institutional Animal Care and Use Committee (IACUC) in AAALAC approved animal care facilities.
Primary autologous DC sorting
Flow cytometry and high-speed cell sorting were used to isolate the peripheral blood-derived DC populations labeled with antibodies targeting the specific canine CD antigens. The peripheral blood mononuclear cell (PBMC) populations were prepared from whole canine blood (60 mL) collected by venipuncture from patient dogs to ethylenediaminetetraacetic acid (EDTA) tubes (Becton Dickinson, USA). Buffy coats were isolated and the PBMC populations were purified by centrifugation on discontinuous Ficoll-Hypaque gradients, as described previously [3]. Selectively washed populations of canine patient PBMCs were resuspended in 4 ml of flow wash buffer (FWB; filter sterilized HBS containing 1% bovine serum albumin fraction V) to block the nonspecific interactions and were incubated for a minimum of 40 min at room temperature.
Canine PBMC populations from individual patients (1 − 3 × 109 cells in 1 mL) were labeled with the specific antibodies against canine CD4 (fluorescein isothiocyanate-conjugated polyclonal rat anti-canine; Bio-Rad AbD Serotec, USA), CD8 (RPE-conjugated polyclonal rat anti-canine; Bio-Rad AbD Serotec), and CD11c (monoclonal mouse anti-canine; Bio-Rad AbD Serotec, and labeled with secondary anti-mouse monoclonal antibody conjugated to Alexa-Fluor 660), as described previously [34]. The cells were analyzed and sorted on a MoFlo XDP flow cytometer and a high-speed cell sorter (equipped with 405, 488, and 635 nm lasers) and the sorting parameters were managed using Summit 5.2 software (Beckman Coulter, USA). Labeled PBMC populations and sorted cell populations were maintained at 4°C. The entire PBMC populations were sorted for each animal for each vaccine production run and the sorted DC-enriched cell populations were collected sterilely into one or more tubes containing 1 mL of fetal bovine serum (FBS). After sorting, the cells were collected by centrifugation and cultured in RPMI-1640 (Gibco/BRL, USA) containing 10% FBS (Hyclone Laboratories Inc, USA) and including penicillin/streptomycin/fungizone (Gibco/BRL), as described previously until fusion [34].
Hybrid-cell fusion and vaccine preparation
Populations of CMT28 and autologous sorted DCs (CD11c+/CD4−/CD8−) were fused by incubation with sterile solutions of 50% w/v polyethylene glycol (up to 3,350 MW) in improved MEM, as described previously, including parallel fusions of stained cells, for analysis by flow cytometry, and unstained cells to be injected into patient dogs [34]. Mixed populations of CMT28/DCs to be fused (5 × 106 autologous DCs fused to 1 × 107 CMT cells at a ratio of 1:2 in 0.5 mL phosphate-buffered saline [PBS]) were prepared, as described previously [336]. The fused cell population, composed of a single injectable vaccine dose (approximately 0.5 mL total/dose), was collected by centrifugation and resuspended in 0.3 mL of sterile pyrogen-free PBS and 0.2 mL of injection-grade pyrogen-free PBS containing 200 µg/injection CpG-containing phosphorothioate oligo-nucleotide immune-stimulant (5′-TCGTCGTTGTCGTTTTGTCGTT-3′) [37].
Animal handling, vaccine injection, sampling and statistics
Dogs diagnosed with mammary cancer by a gross examination were treated by a surgical resection, and a pathology assessment was performed (Auburn University Anatomic Pathology). Informed consent from the owners was obtained in cases where the study inclusion criteria were met. Initiation of the vaccination protocol began approximately 1 week after surgery and the owners were requested to withhold food from 6 PM on the day prior to admission. Each patient animal was admitted to the oncology service in the morning, and 60 mL of blood was collected in EDTA-Vacutainer tubes (Becton Dickinson) for PBMC isolation and vaccine production. The patient animals were then moved to oncology and chemotherapy consisting of the infusion of 2 mg/kg of gemcitabine (diluted in 250 mL of saline) delivered intravenously over a period of 2 h. Dogs were held in kennels with food and water provided ad libitum. The vaccines were constructed as described and delivered to the patients the next morning. The vaccines were delivered into the right popliteal lymph node by a single ultrasound guided injection (18-gauge needle) and were composed of approximately 5×106 autologous DC-CMT28 cell fusions in suspension in PBS with immune-stimulant oligonucleotides, as described elsewhere. The patient animals were observed by clinical staff for approximately 2 h to ensure that no acute adverse reactions were evident and then released to their owners. A follow-up examination at one week after vaccination included a physical examination, blood collection of 10 mL, blood chemistry, and cell (complete blood count) assessment. Thoracic radiographs were a part of the routine monitoring for metastasis.
Each patient was injected with a total of 3 Gemcitabine chemotherapy treatments and vaccinations at 3-week intervals according to the protocol described (Fig. 1). Once the vaccination protocol was complete, including rechecks at 1 week after each vaccination, a further recheck was completed at 9 weeks after the third vaccination and then twice more at 18-week intervals covering approximately the first year. Rechecks by telephone were conducted with the owners over the second year. Further treatment of each patient, if necessary, was conducted under the standard of care and with the consent of the owners.
Fig. 1
Hybrid-DC fusion vaccine strategy for individualized living cell therapy for canine breast cancer. The patient animals were divided into the treatment groups based on a diagnosis after successfully obtaining owner consent. Animals belonging to the owners, who consented to the clinical trial enrollment, were provided with a complete vaccine protocol, including Gemcitabine chemotherapy and an injection of the hybrid-DC fusion vaccine. Animals belonging to those owners who withheld consent, after treatment with a surgical resection of the tumor, were not treated further (control group). All vaccinated animals were assessed at rechecks for up to one year and then by a telephone follow-up interview with the owners for up to 2 years. Control group animals were followed by a telephone interview only.
DC, dendritic cell; Vx, vaccine & Gemcitabine treatment.

The natural history of the disease for each patient was recorded, including the cause and time to death. The Kaplan-Meier curves of survival for each treatment group were plotted (MEDCALC statistical software https://www.medcalc.org). The patients were divided into 3 groups, including the control, in which only a surgical resection was provided at the request of the owners who elected not to participate in the vaccination protocol; vaccine and Gemcitabine treated patients (cBC Vx); and lastly vaccine and Gemcitabine-treated patients, whose disease had progressed to inflammatory carcinoma (iBC Vx) before or at the beginning of the vaccination period. Statistically significant differences between all treatment groups was assessed using the Logrank test (MedCalc) and plots of the 95% confidence overlap (Eureka Statistics calculator http://eurekastatistics.com).
RESULTS
A previous study reported a hybrid-DC fusion vaccine strategy for immunizing normal healthy dogs against CMT cell immunogens based on a high-speed cell sorting strategy for the isolation of autologous canine DCs from healthy beagles [4]. The same strategy was employed to first isolate autologous the primary canine DCs from canine mammary cancer patient blood and then fuse them to CMT cells, as a source of breast cancer-specific immunogens, at high rates (40%–70%). The immunization of canine patients was designed to allow a direct assessment of the therapeutic effects of such vaccine strategies in a spontaneous canine breast cancer model using the dosage and formulations evaluated previously and the allogeneic CMT28 cell line, which has proven to be the most broadly immunogenic (Fig. 2) [34]. Adjuvant therapy was included to enhance the immune response nonspecifically using CpG-encoding oligonucleotides [14]. Gemcitabine chemotherapy was also included because it has been putatively associated with the suppression of Treg populations that are believed to suppress autoimmune recognition [252728]. This formulation was selected because it had been shown to be free of adverse effects in laboratory beagles [34].
Fig. 2
Hybrid-DC fusion vaccine strategy for individualized autologous living cell therapy to treat canine breast cancer. Autologous patient DCs were isolated in enriched populations from whole blood. The buffy coat was isolated first followed by further enrichment of PBMC populations on Ficol Hypaque gradients and centrifugation. The PBMC populations were labeled for 3 surface CD antigens (CD4, CD8, CD11c) and multicolor high-speed cell sorting of rare DC-enriched CD11c+ cell populations was performed. Autologous DCs were then fused in a culture with CMT28 cells using PEG at rates of 40%–60% fusion. These cells were combined with an adjunct CpG oligonucleotide immune-stimulant in a total volume of 0.5 mL of pyrogen-free phosphate-buffered saline for injection following gemcitabine chemotherapy.
DC, dendritic cell; PBMC, peripheral blood mononuclear cell; PEG, polyethylene glycol; CMT, canine mammary tumor.

The selection of canine patients was based on the criteria designed to reduce the clinical complexity and confounding sources of heterogeneity by rigorous application of the vaccination inclusion (Table 1). The patient dogs needed to have a positive diagnosis of mammary carcinoma by histopathology (benign and mixed mammary cancers were excluded) and be greater than or equal to 6 kg in weight due to the volumes and frequency of blood draws required to construct the vaccine. In addition, the patients had to produce cell explants that could be cultured for phenotype analysis, have no prior cancer diagnosis or have been subjected to prior cancer treatment. No metastatic disease (liver or lungs) could be evident to bias the population to an earlier stage disease. Finally, the owners had to agree to complete the trial protocol, comply with surgical resection of the tumors prior to initiating the vaccine treatments and comply with a year-long series of vaccinations and recheck visits followed by a second year of telephone rechecks (Fig. 1).
Table 1
Criteria for autologous hybrid cell vaccination

A total of 14 canine mammary cancer patients were identified and all were reviewed over the course of approximately 2 years (Table 2). The patient animals represented a variety of breeds and sizes of 6 kg or more. All of the animals were identified as reproductively intact female dogs representing a canine population known to be at high risk of mammary cancer [1]. Of the 14 patient animals identified, 6 of the owners declined consent to enroll their animals in the trial, but elected to proceed with standard of care therapy; thus, these 6 dogs comprised the control group (Table 2). These animals were compliant with all 7 enrollment criteria, had undergone a surgical resection, had a positive histologic diagnosis of mammary carcinoma, and were returned to their owners without further treatment. The follow-up interviews were conducted by telephone to determine the health and disposition, including cause and time of death.
Table 2
Animals according to the treatment group with diagnosis, phenotype and survival

The patients were divided into 3 groups, only surgical resection was provided at the request of the owners who elected not to participate in the vaccination protocol (Control); vaccine and Gemcitabine treated patients (cBC Vx); and lastly, vaccine and Gemcitabine-treated patients, whose disease had progressed to inflammatory carcinoma (iBC Vx).
ERα, estrogen receptor α; PR, progesterone receptor; ND, not determined; CMT, canine mammary tumor.
*Determined by histopathology analysis. Grade I (low), Grade II (intermediate), Grade III (high) [35]; †CMT cells from each vaccinated dog were evaluated by quantitative reverse transcriptase polymerase chain reaction for breast cancer (BRCA) gene marker expression including ERα, PR, and HER1–4 receptors (as noted) as previously described [33]. Expression was scored on a 3-point scale of not expressed (−), positively expressed (+) or highly expressed (++). Non vaccinated control dogs and one inflammatory carcinoma case were ND due to lack of availability of specimens; ‡Days from surgical resection to the death of the animal or termination of the study; §Phenotype of canine mammary carcinoma cells including Luminal A (A), Luminal B (B) or HER1–4+ (1–4+) determined as described previously [33]; ∥Dogs surviving through termination of the study (days to death beyond these limits unknown).
Of the remaining 8 animals screened, all entered the vaccine protocol approximately 1 to 2 weeks after the initial surgical resection because all were positive for a diagnosis of mammary carcinoma by histopathology. The vaccinated mammary carcinoma (cBC Vx) group diagnosis ranged from grade 1 to 3, whereas the vaccinated inflammatory mammary carcinoma (iBC Vx) group were all grade 3 (Table 2). All 4 members of this population were identified initially as being mammary carcinoma patients. On the other hand, all 4 developed inflammatory mammary carcinoma following surgery but prior to (2 cases), or just following (2 cases), the first vaccination at the beginning of the treatment period. The animals that developed inflammatory carcinoma were segregated into a separate treatment group because of the aggressive nature and poor prognosis of this mammary cancer subtype (inflammatory mammary carcinoma, Table 2). The remaining 4 patient animals comprised the canine breast cancer (cBC) vaccine and gemcitabine chemotherapy treatment group (Table 2). Six animals in these last 2 patient groups completed the full treatment protocol; 2 of the inflammatory carcinoma patients died prior to completion of the last injection in the vaccine series. The patient animals in each group were all of different breeds and were comparable with respect to age and weight range for these small groups, reducing this as a source of bias between the treatment groups. The cBC Vx group ranged from 4–12 years and 15–29 kg, whereas the iBC Vx group ranged from 7–11 years and 6–28.4 kg and the control mammary carcinoma group (control) ranged from 8–12 years and 6–26.4 kg (Table 2).
Mammary carcinomas from the initial surgeries were assessed for the histologic grade and breast cancer phenotype comparable to human breast cancer phenotype analysis, as described previously [8]. For the cBC Vx group, the phenotypes were all Luminal B with but one exception of luminal A. All cBC Vx cases were also HER4+ and all but one of the Luminal B tumors were HER3+, as was the luminal A tumor (Table 2). The iBC Vx group phenotypes were all Luminal B and only one was HER3+ whereas all were HER4 positive. The phenotypes for the control mammary carcinoma group (control) and one of the inflammatory mammary carcinoma tumors were not determined due to a lack of specimens to assess (Table 2).
The survival of the patient animals in each of the 3 treatment groups revealed distinguishable differences in the times to death for each population. Kaplan-Meier curves and the associated log-rank test of patient survival according to the treatment group also demonstrated the effects of the combined vaccine and Gemcitabine treatment compared to the control treatment group (Fig. 3 and Table 3). Median survival of mammary carcinoma patient animals in the vaccine and Gemcitabine treatment group (cBC Vx - median survival of 611 days) were prolonged approximately 3.3-fold compared to survival of the control group (median survival 184 days) and also were anecdotally reported by the owners to have exhibited an enhanced quality of life when compared to the period prior to treatment during follow-up interviews (Tables 2 and 3, Fig. 4). These differences were analyzed using the log-rank test and were statistically significant among all groups (p = 0.0019, Table 3). The areas representing the 95% confidence levels between the vaccinated breast cancer and control treatment groups overlapped only peripherally largely due to the higher variation in survival times encountered in the control group (Fig. 4). The differences between the vaccinated and control animal survival times represent a median increase in the observed survival of approximately 14 months for vaccinated animals when compared to the control group. For these 2 experimental groups, contact with the owners of the last few patient animals was lost after 23 months survival for the vaccine (2 animals) and after 29 months for the control group (one animal). Only one surviving vaccinated animal reported any recurrence at that time.
Fig. 3
Kaplan-Meier curves of canine breast cancer patient survival according to the treatment group. Kaplan-Meier survival plots were calculated for patients diagnosed with mammary carcinoma in each of the 3 treatment groups (percent survival vs. time in days), including the vaccine and Gemcitabine treatment group (cBC Vx - 4 animals total), control treatment group (Control - 6 animals total treated with surgical resection only), and vaccine and Gemcitabine treatment group for patients who progressed to inflammatory carcinoma during the vaccine trial (iBC Vx – inflammatory carcinoma progression before the second vaccination, 4 animals total). For each plot, the line ends where the data stream ended and there was no further contact with the owners (cBC Vx and control groups) or when all animals in the group were deceased (iBc Vx group).
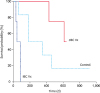
Table 3
Median percent survival of patient animals by treatment group

| Treatment group | Median survival* | 95% confidence interval | Log-rank significance |
|---|---|---|---|
| cBC Vx | 611 | 427 to 639 | p = 0.0019 (for all groups) |
| iBC Vx | 42 | 31 to 85 | |
| Control | 184 | 183 to 458 |
The patients were divided into 3 groups, mammary carcinoma controls treated with surgery only (Control); mammary carcinoma treated with the fusion vaccine and Gemcitabine (cBC Vx); and inflammatory mammary carcinoma treated with the fusion vaccine and Gemcitabine (iBC Vx).
*Survival was calculated in days to the end of the study where 2 treated cBC Vx patients and 1 control patient survived beyond termination of the study (Table 2).
Fig. 4
Median survival times for canine breast cancer patients. The median survival times were calculated for each of the 3 experimental groups – vaccinated mammary carcinoma (cBC Vx), vaccinated inflammatory carcinoma (iBC Vx), and control mammary carcinoma (Control). The 95% confidence limits are shown (vertical bars) and statistical significance was calculated from the data in all groups in Fig. 3 using the log-rank test (Table 3). The significance in pairwise group comparisons were: BrCa Vx vs. iBrCa groups (p < 0.0001), BrCa Vx vs. control groups (p = 0.18) (significant at 82% confidence), and iBrCa vs. control groups (p = 0.75). The 95% confidence level was not achieved in 2 of the pairings against the control group due primarily to the large variations observed in the control group survival even though significance at > 95% was achieved for the study overall (Table 3).

A comparison of the inflammatory mammary cancer group revealed a very short median survival time of 42 days, confirming the very poor prognosis for patients with such diagnoses (Figs. 3 and 4). This data also suggests that vaccination had little or no effect on the progression of disease in these breast cancer cases possibly because the rapid progression of disease may not have allowed for a treatment response.
DISCUSSION
Canine and human breast cancers are similar on many levels. The development of disease composed of malignant mammary carcinomas in patients in both species demonstrates similar age-associations, as well as nutritional, environmental, and reproductive factors that correlate with tumorigenesis [73839]. Patients in both species also share similar genetics, histologic appearance, biological behavior, molecular targets, and therapeutic response to treatment [739]. Both human and canine breast cancers exhibit cellular heterogeneity within the tumor and its surrounding environment, and tumors readily develop resistance to existing treatments. In addition, tumors in both species develop spontaneously in the context of an intact immune system. This study attempted to exploit the patient immune system using adjunct treatment along with surgery to develop patient-customized immune therapy for canine breast cancer that may have translational potential for human disease.
Canine mammary tumor (CMT) cell lines are stable lines of cells derived from malignant canine mammary cancers with a well-characterized cancer morphology and genetic defects [268323336]. A strategy and technology for high-speed cell sorting of primary canine DCs for construction of canine hybrid-DC fusion vaccines using these CMT cell lines were previously reported [34]. The resulting DC fusions were of high quality (fusion rates of 40%–70%) and vaccination induced significant enhancement of both cytotoxic T lymphocyte activity and serum immunity in normal healthy dogs with no observable general or immune-related adverse effects, even with repeated vaccination.
This study investigated patient dogs diagnosed with non-metastatic mammary cancer (grade 1–3), and evaluated the therapeutic outcomes following vaccination with these autologous hybrid-DC fusions in association with a non-specific immune-stimulant CpG oligonucleotide, which is known to act as a toll receptor 9 agonist, and adjunct Gemcitabine chemotherapy [5252728]. The intent was to enhance the patients' immunity by therapeutic vaccination to manage residual disease, following a surgical resection, as well as potential recurrent disease by establishing functioning immune memory to tumor-associated antigens (TAAs). Because these vaccine constructs were based on the patient’s own DCs, they have the potential for direct CMT cell antigen processing and presentation. The delivery of vaccine constructs directly into the draining popliteal lymph nodes was designed to promote and prime the local/regional immune responses enhanced by the CpG effect.
The histologic grade of the tumors in the cBC Vx group and the iBC Vx group reflected the severity of each disease. The cBC Vx group were composed primarily of grade 1–2 tumors with one grade 3 tumor evident, whereas the iBc Vx group was composed entirely of grade 3 tumors. Both vaccinated groups were composed largely of Luminal B phenotype tumors with one exception of one Luminal A tumor in the cBC Vx group. Most interesting was the presence of HER3 positive phenotypes in all but one cBC tumor and HER4+ phenotypes in all of the vaccinated tumors in both groups. This supports the correlation between the HER3/HER4 positive phenotypes in these tumors, as proposed previously [33].
Adjunct gemcitabine chemotherapy was administered approximately 24 h prior to vaccination following blood collection for vaccine construction. This treatment was designed to help promote Treg suppression in an effort to promote self-antigen recognition and a partial break in immune tolerance [252728]. Gemcitabine is a nucleoside analogue that is similar to 5-fluorouracil (5-FU) and can replace the nucleoside, cytosine, promoting the arrest of proliferating cells in the S phase. Antitumor recognition can be enhanced by selectively depleting myeloid suppressor (Gr-1+/CD11b+) cells and can result in an enhancement of apoptosis or programed cell death [25]. In humans, this treatment has fewer side effects compared to 5-FU (such as neutropenia), but this has not been confirmed in dogs. Moreover, it has been shown to be an effective anticancer chemotherapy on its own in the treatment of human non-small cell lung cancer, pancreatic cancer, bladder cancer, and breast cancer [313540]. The role of gemcitabine in modifying the immune response by promoting the breaking of tolerance to TAA(s) has been characterized in terms of the lower Treg populations but may act to increase the activation of helper and cytotoxic T cells [25262728]. The relatively low number of animals investigated did not allow an independent investigation of the individual vaccine components. Because they were not investigated independently, it is possible that some or indeed all of the improvements in the patient outcome were due to either the vaccine or gemcitabine treatment or were due to a combination of both treatments. Similarly, it is also possible that CpG alone could elicit at least some of this improvement, but this is unlikely because such adjunct treatments have not been shown to improve specific immune reactions independently [37]. Although the results of this preliminary investigation are quite promising, further investigation involving more cases will be needed to resolve the contributions of each component of the vaccine strategy.
As reported previously for laboratory beagles, living autologous DC/CMT cell fusion vaccines were synthesized successfully for each patient using freshly sorted patient DCs. The vaccine was applied to 2 different patient populations with clinically distinct diagnoses. The first was composed of patients with mammary carcinoma and the second was composed of those with inflammatory mammary cancer. The clinical outcomes in these 2 groups were compared with a third group of canine mammary cancer cases with diagnoses of mammary carcinoma who underwent a surgical resection but whose owners declined to participate in the vaccine treatment. No additional bias should have been introduced because this was the sole reason for the assignment of otherwise compliant animals to the control group.
The median survival time for each of these treatment groups was very different. The median survival of patient animals in the vaccine/gemcitabine group (cBc Vx) was 611 days, which was 3.3 times longer than the survival of the control group (184 days). Thus, vaccination and gemcitabine treatment together appeared to prolong survival from the date of the surgical resection for each patient. This represents a median increase in survival of approximately 14 months, possibly because the vaccine complex may have prolonged survival by increasing the number of CMT-specific T-cells or CMT-specific immunoglobulins. In addition, the owners of the longest lived animals anecdotally reported improvement in the patient's quality of life, including improvements in activity, diet, and demeanor compared to the period prior to treatment. No observable effects of excessive cytokine release associated with significant tumor cell lysis were observed, possibly due to surgery prior to administration of the vaccine. All patients demonstrated excellent tolerance of the treatment protocol with no general or immune-related adverse reactions reported, which are consistent with the previously published data [67]. This included a lack of change in the remaining mammary glands of any of the treated animals on follow-up gross examinations. Unlike previous investigations on healthy laboratory dogs, no histological analysis was possible in these client-owned animals [3].
Because the patient animals in this study could have shown more immune suppression than the healthy laboratory animals in previous experiments [34], there were some concerns that there was a greater potential for the CMT cell component of the vaccine to be tumorigenic. Unfortunately, the biopsy specimens needed to evaluate this concern could not be taken as these were client-owned animals with spontaneous disease. On the other hand, given the much longer survival time of the vaccinated animals in the breast cancer vaccine group with no gross evidence of recurrence and their evident quality of life, it is unlikely that this was a problem because there were no long-term adverse effects observed and no evidence of tumor growth, particularly near the site of injection.
A comparison of the outcomes with the inflammatory carcinoma group could not have been more in contrast because this group had a very short median survival time of approximately 42 days, which is consistent with the very poor prognoses for patients with such diagnoses [1]. Vaccination had no apparent effect on the inflammatory carcinoma cases and in some cases, death preceded completion of the trial vaccine treatment protocol, making these cases clearly very different from the other treatment groups. In these cases, the inflammatory carcinoma subtype is likely to be responsible for the short survival time because such cases in dogs also include the triple negative mammary cancer disease phenotype. Death in these cases may have involved enhanced inflammatory cytokine levels [29333940].
Because the numbers of cases were not large, and in some iBC Vx cases, the patients died before completing the vaccination protocol, there was some concern over the induction of an adverse reaction in this group. On the other hand, treatment was unlikely to have induced inflammatory carcinoma because 2 of these cases were diagnosed as inflammatory prior to administration of the first vaccine injection, indicating disease progression to this phenotype occurred prior to initiating the vaccine protocol. The remaining 2 cases were also diagnosed with inflammatory carcinoma early before the second vaccination. For these 2 cases, induction of an inflammatory carcinoma subtype by the first vaccination, albeit unlikely, cannot be ruled out.
In summary, further development of autologous DC-based vaccines in patient animals to improve the management of canine mammary tumors is warranted because of the success in extending the lifespan and improving the quality of life of these patients. On the other hand, it is unlikely such an approach could be developed successfully in a traditional practice setting without exceptional technical support. Despite this, these approaches could lead to the identification of antigens capable of eliciting an effective immune response that can lead to a more traditional antigen-based vaccine that could be delivered as a living cell vaccine, such as in the case for Sipuleucel-T in the treatment of human prostate cancer [41]. This approach to the treatment of canine breast cancers could also serve as an important intermediate model of human disease for the development of living immunomodulatory cancer treatments.
 XML Download
XML Download