

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
A Class III skeletal pattern can be caused by maxillary hypoplasia, mandibular prognathism, or a combination of both.1 In cases of midface deficiency requiring maxillary protraction, orthopedic treatment has been shown to yield favorable results.2
The facemask is an effective device for the treatment of mild to moderate Class III skeletal malocclusion with maxillary retrusion; however, it can result in undesired effects such as molar mesialization and maxillary incisor proclination.34
Previous studies have reported the use of attachments with skeletal anchorage for maxillary protraction; these include ankylosed deciduous canines,56 onplants,7 miniplates,8 miniscrews,9 hybrid hyrax (HH)-mentoplate combination,1011 and even osseointegrated titanium implants.12 These provided skeletal outcomes similar to those obtained with the facemask, with the added advantage of no undesired dentoalveolar movements.
Generally, rapid palatal expansion (RPE) is used as an adjunct to maxillary protraction.4 Loosening of the circummaxillary sutures by alternate rapid maxillary expansions and constrictions (Alt-RAMEC) has also been reported to improve the mechanics of orthopedic treatment for Class III malocclusion.131415
Here we report the first case, to the best of our knowledge, involving the use of Alt-RAMEC with an HH-mandibular miniplate combination and simultaneous orthodontic treatment for the management of severe Class III malocclusion caused by maxillary hypoplasia in an 11-year-old girl.
DIAGNOSIS AND ETIOLOGY
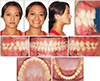
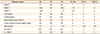
An 11-year-old girl presented with Class III malocclusion and facial and psycho-affective involvement. On examination, she exhibited skeletal Class III malocclusion, a concave profile, levognatism, and a severe anterior crossbite (Figure 1, Table 1). Panoramic radiograph, lateral cephalometry, and cone beam computed tomography confirmed the presence of Class III malocclusion (Figure 2, Table 1).
TREATMENT OBJECTIVES
The following treatment goals were established: correction of the Class III skeletal pattern, improvement of the facial profile, an increase in the overjet, correction of the posterior crossbite, and an improvement in facial esthetics.
TREATMENT ALTERNATIVES
Different treatment alternatives were considered for the correction of Class III malocclusion. The first option was maxillofacial surgery after skeletal growth completion. However, this would result in further deterioration of her facial appearance. The second option was orthopedic treatment involving RPE with a hyrax appliance and protraction with a facemask; this was ruled out because of the possible effects of dentoalveolar compensation and the severity of malocclusion. Considering the severity of the Class III malocclusion and the need to correct the maxillary sagittal position without undesired dental effects, we decided to use Alt-RAMEC with an HH-mandibular miniplate combination and simultaneous orthodontic treatment with passive self-ligation.
TREATMENT PROGRESS
After the patient's family approved the treatment plan, an 8-week ALT-RAMEC protocol13 involving expansion and constriction every alternate week was established. An HH appliance was used as proposed by Wilmes et al.10 As the first step of treatment, a silicone impression was recorded (Figure 3) and the appliance was fabricated using the Ortho-Easy Forestadent® system (Bernhard Foerster GmbH, Pforzheim, Germany) for skeletal anchorage (Figure 4).
The HH appliance was cemented with Band-Lok (Reliance Orthodontic Products, Itasca, IL, USA), and passive self-ligating brackets (Damon Q; Ormco®, Orange, CA, USA) were placed on the maxillary teeth for the initiation of simultaneous orthodontic treatment with a fixed appliance. The maxillary archwire was sectioned in the midline to facilitate transverse orthopedic movement. After the 8-week Alt-RAMEC protocol, a diastema between the maxillary incisors and a mild improvement in the overjet were observed (Figure 5).
Subsequently, mandibular miniplates were placed (Figure 6), following which passive self-ligating brackets (Damon Q) were bonded to the mandibular teeth. Intermaxillary elastics (2 oz; size, 3/16-inch; Ormco®) were used as part of the mechanics recommended with this type of bracket. In addition, 5/16-inch intermaxillary elastics (8 oz; Ormco®) were extended from the mandibular miniplates to the HH appliance (Figure 7).
RESULTS
After 20 months of treatment, the devices were removed and the family was instructed about a control and retention program that should be carefully followed in accordance with the patient's growth. The final result included the correction of Class III malocclusion with adequate function and excellent esthetics, which helped the patient in recovering her self-esteem and provided personal motivation (Figures 8 and 9).
Maxillary protraction was observed, with an improvement in sella-nasion-A point from 77° to 84°. Sellanasion-B point was controlled, with a minor increase of 1.5°, and A point-nasion-B point and the Wits appraisal value improved from −6.5° and −12 to −1° and −5 (Table 1), respectively.
The maxillary incisor inclination was maintained, although the mandibular incisors were retroclined by 5° (Table 1).
Superimposition of pre- (T0) and post-treatment (T1) lateral cephalograms revealed an improvement in the soft tissue profile, upper lip projection, maxillary advancement, and sagittal control of mandibular growth (Figure 9).
After 24 months of retention, the outcomes appeared stable, as confirmed by superimposition of post-treatment (T1) and post-retention (T2) lateral cephalograms (Figures 10 and 11, Table 1).
DISCUSSION
The use of an HH-mandibular miniplate combination has been shown to be effective for the correction of Class III malocclusion in growing patients.1011 Nevertheless, to the best of our knowledge, this is the first case report on the use of Alt-RAMEC with an HH-mandibular miniplate combination and simultaneous orthodontic treatment for the management of severe Class III malocclusion in a young girl in the growth phase.
Conventionally, the facemask is used for the treatment of patients with Class III malocclusion due to maxillary hypoplasia.4 A systematic review and metaanalysis evaluated skeletal and dental changes after facemask treatment and found that SNA improved by 2.1°.16 On the other hand, another study reported that RPE with an HH-mentoplate combination resulted in an improvement of 3.2°.11 Both values were considerably smaller than that observed for the present patient, who exhibited an improvement in SNA of 7° (Table 1). This finding is in agreement with that in a previous study,15 where maxillary advancement was greater with Alt-RAMEC and facemask treatment than with conventional RPE and facemask treatment or no treatment (control). We also observed an improvement in ANB (5.5°) and the Wits appraisal value (7 mm) in our patient. With regard to dental measurements, we observed stability in the inclination of the maxillary incisors (U1-PP, −1°) and retroinclination of the mandibular incisors (L1-PM, −5°) between T0 and T1; the retroclination probably occurred because of the use of Class III intermaxillary elastics extending from the brackets (Table 1).
Although the use of an HH appliance and mandibular miniplates is more invasive than conventional treatment, it may benefit patients who prefer to use intraoral devices. 11
De Clerck et al.8 previously reported the use of skeletal anchorage in both the maxilla and mandible for the correction of Class III malocclusion, with excellent skeletal results without dental compensation, including two miniplates in the maxilla and two in the mandible. Our patient received miniplates only in the mandible in accordance with previous reports.1011
The duration of conventional facemask treatment can vary from 12 to 15 months,16 and it can be decreased to 6 to 9 months with RPE using an HH-mentoplate combination. 10 In previous reports, however, a second phase of orthodontic treatment was required after the first phase of orthopedic treatment. This second phase can last for an average of 20 months (range, 14–33 months), as reported in a recent systematic review.17 For the present case, the overall treatment duration was 20 months; this indicates that our protocol involving the simultaneous use of orthopedic and orthodontic treatment was more efficient than previously reported ones. We used elastics extending from the miniplates to the HH appliance and from the maxillary to the mandibular brackets with a Class III vector. The use of passive self-ligation brackets minimized friction, facilitated physiological sliding of the teeth in their bony bases for the correction of malposition, and corrected the sagittal position of the jaws. The decrease in the duration of active treatment is the most important finding from the present case. Considering that facial esthetics in adolescence is a determining factor for the development of a personality and interpersonal relationships, we recommend the use of this protocol for growing patients, who will exhibit not only an improved physical appearance but also a better quality of life.
After 24 months of retention, our patient showed adequately stable dental and skeletal outcomes (Figures 10 and 11, Table 1). In addition, she experienced no complications or failure during or after treatment with the HH appliance and miniplates and showed excellent compliance with the treatment. At the time of writing this manuscript, she was still in the retention phase and regularly visited our clinic every 6 months for review of her growth. In case of significant relapse, we planned to prescribe intermaxillary elastics with a Class III vector to the retainers. Although both the patient and her parents were very satisfied with the treatment outcomes, we did not rule out the possibility of orthognathic surgery in case the patient requested further improvement in her facial esthetics in the future.
CONCLUSION
In conclusion, the findings from this case suggest that Alt-RAMEC with an HH-mandibular miniplate combination and simultaneous orthodontic treatment offers several advantages over other approaches, including direct application of forces to the skeletal structures, increased loosening of circummaxillary sutures, no requirement of extraoral devices, lesser invasiveness, and decreased treatment duration. Future studies should compare the effects of this treatment protocol with those in a matched control group and evaluate its long-term stability.










 XML Download
XML Download