

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The assessment of skeletal maturity in growing orthodontic patients is an essential step in treatment planning and in defining the appropriate treatment timing. Developmental, rather than chronological, age is used because of the diversity in individual growth patterns1; additionally, skeletal maturity is closely related to sexual maturity and somatic growth.2
The hand-wrist is the most commonly used site for evaluating skeletal maturity.3 Among the various methods using hand-wrist radiographs,456 determination of skeletal maturity indicators (SMIs) is an objective, reliable, and easy method of determining skeletal maturity.4 The Tanner–Whitehouse (TW) method is the most accurate, but it is somewhat complex and time-consuming and requires significant evaluator expertise.5 Meanwhile, when a lateral cephalometric radiograph is taken for diagnosis in a patient planned for orthodontic treatment, the skeletal maturity can also be determined based on the cervical vertebrae in the radiograph, with no need for a hand-wrist radiograph. Hassel and Farman7 proposed a cervical vertebrae maturation indicator (CVMI) based on the vertebral body of the cervical vertebrae, and the maturity of the hand-wrist is highly correlated with that of the cervical vertebrae.78
Regarding the relationship between vertical facial type and skeletal maturity, Nanda9 reported that the adolescent growth spurt was faster in a group with open-bite than in a group with deep-bite. Verulkar et al.10 also reported that skeletal maturity tended to be delayed in the horizontal grower than in the vertical grower, but the difference was insignificant. Apart from these previous studies, little is known about the relationship between vertical facial type and skeletal maturity. Furthermore, there have been only a few studies on the applicability of the mandibular plane angle, which is a simple measure for evaluating vertical skeletal patterns.
This study aimed to evaluate the differences in skeletal maturity in relation to vertical facial types and to compare differences in skeletal maturity between the cervical vertebrae and hand-wrist. The null hypothesis was that there is no difference in skeletal maturity between the cervical vertebrae and the hand-wrist in relation to vertical facial type.
MATERIALS AND METHODS
Study design and samples
Of the 95 females who visited Yonsei University Dental Hostpital (Seoul, Korea) from January 2005 to February 2018, 59 females who met the following criteria were included in the study sample: age 7 to 9 years (84 to 119 months) and skeletal Class I malocclusion (ANB [A point, nasion, B point] angle, 2.0 to 4.0°; Wits: −5.3 to −0.3 mm).
The exclusion criteria were as follows: craniofacial anomalies (e.g., cleft lip, cleft palate), growth disorders such as precocious puberty, previous history of growth hormone therapy, discovery of anomalies of the hand-wrist bone or the vertebrae in radiographs, radiographs with quality that was unusable for cephalometric analysis and/or evaluation of skeletal maturity, and a difference of more than 3 months between the acquisition of lateral cephalometric and hand-wrist radiographs.
With the mean mandibular plane angle defined as 37.0 ± 4.0° with reference to studies on the growth and development of normal Korean females,1112 the subjects were divided into three groups based on the mandibular plane angle to the cranial base (SN-GoMe; Figure 1C): low-angle group (mandibular plane angle < 33.0°); normal-angle group (33.0° ≤ mandibular plane angle < 41.0°); and high-angle group (mandibular plane angle ≥ 41.0°).
Based on a preliminary study, to measure the difference in the mandibular plane angle between groups with p value < 0.05, a power of 80%, and an effect size of 0.8, the minimum sample size required was 42 (G* Power 3; Universität Düsseldorf, Düsseldorf, Germany).
This study protocol follows the Declaration of Helsinki and has been approved by the Institutional Review Board of Yonsei University Dental Hostpital, Seoul, Korea (No. 2-2017-0050).
Radiographic analysis
The lateral cephalometric and hand-wrist radiographs were estimated by an orthodontist at Yonsei University Dental Hostpital, Seoul, Korea (Figures 1 and 2).
The craniofacial complexes were evaluated using lateral cephalograms (Figure 1). The lateral cephalograms were digitized using V-ceph software version 5.5 (Osstem, Seoul, Korea) by a calibrated expert (Y.S.L.) who was blinded to the patients' status. Thirteen landmarks were used for the cephalometric analysis (Figure 1A). In each group, the characteristics of the craniofacial complex were evaluated using eight linear (Figure 1B) and eight angular measurements (Figure 1C).
Assessment of skeletal maturity was performed by an observer who was unaware of the patients' status. When determining the SMIs, the thumb, third finger, fifth finger, and radius were evaluated in hand-wrist radiographs, and an SMI (graded from 1 to 11) was derived according to Fishman's SMI method.4 To determine the TW3 bone age, 13 bones on the hand-wrist radiographs were evaluated (Figure 2). Each bone was rated, and bone age was determined by converting the ratings into corresponding scores.5 When determining CVMIs, the second, third, and fourth bodies of the cervical vertebrae were evaluated in lateral cephalometric radiographs, and the CVMI was graded from 1 to 6 according to Hassel's classification method.7
Reproducibility
Reproducibility was verified by comparing the values acquired from the original examination with those acquired from the subsequent examination after 2 weeks; the same observer acquired both sets of measurements using the originally implemented protocol. The intraclass correlation coefficient was used to calculate errors and was > 0.90 for all cephalometric measurements and assessments of skeletal maturity.
Statistical analyses
All statistical analyses were conducted using IBM SPSS Statistics 20.0 for Windows (IBM Corp., Armonk, NY, USA). The Shapiro–Wilk test was used to verify the normalization of the data distribution. Normally distributed data were analyzed by one-way analysis of variance with the Bonferroni post-hoc test. The Kruskal–Wallis test was used for non-normally distributed data, and Bonferroni correction was performed for the post-hoc test.
Spearman's rank correlation coefficient was used for evaluating the correlations between skeletal maturity and mandibular plane angle (r < 0.4, weak correlation; 0.4 < r < 0.6, moderate correlation; r > 0.6, strong correlation).13 A p-value < 0.05 was considered statistically significant.
RESULTS
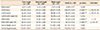
This study consisted of 59 females (low-angle group, n = 16; normal-angle group, n = 26; high-angle group, n = 17; Table 1). The mean mandibular plane angle significantly differed among the three groups (p < 0.001). The mean ages at the acquisition of lateral cephalometric and hand-wrist radiographs were almost the same (104.81 ± 9.18 and 104.98 ± 8.98 months, respectively) and did not differ among the three groups.
The total and lower anterior facial heights were higher in the high-angle group than in the other groups (p < 0.001) (Table 2). The posterior facial height and ratio of the posterior facial height to the anterior facial height were significantly higher in the low-angle group than in the high-angle group (p < 0.001). The gonial angle was higher in the high-angle group than in the other groups, and the lower half of the gonial angle was the greatest in the high-angle group, followed by the normal-angle group and then the low-angle group (p < 0.001) (Table 3).
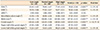
SMI and TW3 bone age were significantly higher in the high-angle group than in the low-angle group (p < 0.05; Table 4). The median SMI was 2 in the low-angle group and 3 in both the normal- and high-angle groups. The median value of CVMI was 1 in the low- and normal-angle groups and 2 in the high-angle group. The median TW3 bone age was 11.4 months higher in the high-angle group than in the low-angle group.
Skeletal maturity weakly correlated with the mandibular plane angle (SMI, r = 0.391; TW3 bone age, r = 0.333; CVMI, r = 0.259; Table 5). There was a strong positive correlation between SMI and TW3 bone age (r = 0.829; p < 0.001) and a moderate positive correlation between skeletal maturity of the hand-wrist (SMI and TW3 bone age) and CVMI (r = 0.580 and r = 0.463, respectively; p < 0.001).
DISCUSSION
The results of this study revealed that the median SMI was 2 in the low-angle group and 3 in both the normal- and high-angle groups, and the median TW3 bone age was 11.4 months higher in the high-angle group than in the low-angle group. Even considering the fact that the mean age at which hand-wrist radiographs were obtained was 4.22 months higher in the high-angle group than in the low-angle group, the results indicate a large difference in the TW3 bone age between the two groups. Thus, we can infer that skeletal maturation occurred more rapidly in the high-angle group than in the low-angle group.
The skeletal maturity in growing patients is an important factor influencing the decision to start orthodontic treatment and the selection of treatment modalities. The incidence of precocious puberty in children aged 7–9 years, especially in females, has been increasing recently due to the chemicals in cosmetic products and some pharmacological insecticides,14 and rapid maturation of the craniofacial structures and teeth was reported in females diagnosed with precocious puberty.15 However, if individuals show differences in skeletal maturity depending on the anteroposterior or vertical facial types, the facial type would have to be considered before discriminating growth disorders such as precocious puberty. Studies on the relationship between the anteroposterior facial type and skeletal maturity have reported no difference in skeletal maturity depending on the anteroposterior facial type or a slightly delayed tendency in skeletal Class II patients.1617 However, only a few studies have assessed the relationship between vertical facial type and skeletal maturity, and the results were inconsistent.910 Therefore, this study aimed to evaluate differences in skeletal maturity in relation to vertical facial type and compare the difference in the cervical vertebrae and hand-wrist in 7 to 9-year-old females.
Most previous studies classified their patient groups based on the ratio of lower anterior facial height to anterior facial height.918 However, in the present study, we classified our groups based on the mandibular plane angle, a widely used, simple index.
In the present study, there was no difference in the ANB among the three groups (Table 3). However, sella, nasion, A point (SNA) and sella, nasion, B point (SNB) angle were smaller and the lower half of the gonial angle was larger in the order of the low-angle, normal-angle, and high-angle groups. These results indicate that the direction of growth is clockwise and vertical, as the mandibular plane angle increases, resulting in an increased anterior facial height and a decreased posterior facial height (Table 2).
However, there was no difference among the three groups in facial depth and facial length. This finding was inconsistent with that of a previous study in which facial depth increased in patients with posterior downward growth and facial length increased in patients with anterior downward growth.19 This inconsistency may be due to the variations in measurements across individuals, and if we had evaluated the changes in measurements for each individual, the corresponding results may have been different from those reported herein.
In this study, two methods (SMI and TW3) were used to evaluate the skeletal maturity of the hand-wrist. The TW method was revised to the TW3 in 2001, and although originally developed for European and North American children, it is known to be suitable for Asians as well.20 Both the SMI and TW3 methods traditionally use images of the left hand, since one study reported that the dominant hand of tennis players shows faster skeletal maturity than the non-dominant hand and most people are right-handed.21 However, because several previous studies reported no difference in skeletal maturity between the left and right hands or between the dominant and non-dominant hands,2223 hand-wrist radiographs of the right hand could be used in the present study.
In this study, skeletal maturity of the hand-wrist (SMI and TW3 bone age) was higher in the high-angle group than in the low-angle group. According to Nanda,9 females with open bite showed the earliest timing of maximum growth. In many cases, patients with open bite have a smaller posterior facial height and shorter ramal height, which may be related to compensatory alveolar growth and eruption of the posterior teeth. Therefore, the high skeletal maturity in short posterior facial height observed in the present study seems to be consistent with the findings reported by Nanda.9 Verulkar et al.10 also reported a tendency for skeletal maturation to be delayed in patients with a horizontal growth pattern than in those with a vertical growth pattern, but the difference was nonsignificant.
Unlike previous studies that have established that the maturity of the hand-wrist and that of the cervical vertebrae are highly correlated,78 the present study did not show a strong correlation between the maturity of the hand-wrist (SMI and TW3 bone age) and CVMI. In addition, CVMI showed the lowest correlation with the mandibular plane angle in the skeletal maturity evaluation method. Therefore, it is recommended that skeletal maturity should be investigated by taking an additional hand-wrist radiograph when assessing growth and development in females.
Although we could not identify a clear association between vertical facial type and skeletal maturity, we observed higher skeletal maturity of the hand-wrist in patients with a high angle than in those with a low angle. Therefore, when determining the timing for orthodontic treatment, we may consider starting treatment earlier in patients with a high angle than in those with a low angle. It should also be noted that the same results were obtained for both methods (SMI and TW3) used to evaluate the skeletal maturity of the hand-wrist. Therefore, it seems logical to evaluate the skeletal maturity of the hand-wrist using the simple and fast SMI instead of the relatively complicated TW3 method in clinical scenarios.
This study had several limitations. This study is a retrospective cross-sectional study that included only a small number of Korean females. Therefore, generalization of the results derived from this study is difficult. Further assessment of the relationship between mandibular plane angle and skeletal maturity requires additional longitudinal studies involving a large number of subjects and both sexes.
CONCLUSION
Despite the limitations of this study, the skeletal maturity of the hand-wrist with a high angle was higher than that of the hand-wrist with a low angle in females. Taking an additional hand-wrist radiograph might be helpful for the precise evaluation of skeletal maturity when assessing growth and development in females. In females with a high mandibular plane angle, the time to commence orthodontic treatment might be earlier than that in females with a low mandibular angle.





 XML Download
XML Download