

 PDF
PDF ePub
ePub Citation
Citation Print
Print


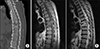
An 83-year-old man presented to our hospital with acute back pain. Vital signs were normal. Laboratory evaluation showed a normal leukocyte count and a C-reactive protein (CRP) of 0.6 mg/dL (range <0.3). However, computed tomography revealed destruction of the Th7–Th8 vertebrae (Fig. 1A), and magnetic resonance imaging showed an epidural lesion with anterior dural compression (Fig. 1B). He had well-controlled type 2 diabetes mellitus with hemoglobin A1c up to 6.5% and had taken neither steroids nor immunosuppressive agents.
Histological evaluation of specimens obtained by needle biopsy confirmed necrosis and neutrophil infiltration (HE stain; Fig. 2). Tuberculous spondylitis was diagnosed by a positive culture for Mycobacterium tuberculosis complex; unexpectedly, the interferon-gamma release assay (T-SPOT. TB) was negative. Detailed inquiries on his medical history revealed that 8 months previously, he suffered from severe systemic reaction after intrarenal Bacille Calmette-Guerin (BCG) therapy for upper tract urothelial carcinoma in situ (CIS). These findings were compatible with a disseminated BCG infection. Due to progressive weakness of the legs, he was referred to a specialized hospital for posterior spinal fusion and antituberculosis treatment.
BCG is an attenuated strain of Mycobacterium bovis. BCG therapy is considered to provoke local immunological responses. Intrarenal BCG is effective in the treatment of upper urinary tract CIS in a long-term follow-up.1 Although BCG therapy is the gold standard of care for high-risk patients intolerant to resection, it can cause rare but serious complications, including sepsis, miliary tuberculosis and spondylitis.2
The timeframe for BCG spondylitis onset varies considerably (0.5 months–12 years).2 Leukocyte counts are usually normal, and CRP levels are lower than those seen in pyogenic vertebral infections. In addition, T-SPOT.TB negative results are likely to indicate BCG infections with a deletion of region of difference 1 (RD1), which is present in the DNA of M. tuberculosis complex except with BCG.2 BCG spondylitis should be considered in patients with back pain who have received BCG therapy, even when the treatment was performed several months to several years previously.2

 XML Download
XML Download