

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Bilateral thalamic gliomas (BTGs) are one of the rarest types of brain tumor. Primary thalamic gliomas account for about 1%–1.5% of all intracranial tumors, and BTGs are even rarer [1]. Most BTGs occur in adults, with only 25% of such tumors found in patients younger than 15 years [123].
Magnetic resonance imaging (MRI) with contrast is the best method for a preoperative diagnosis of brain tumors, as many brain tumors have characteristic radiographic features. A more accurate diagnosis and optimal treatment selection require further histopathological and molecular studies following a stereotactic biopsy. According to World Health Organization (WHO) grades, tumors are graded from I to IV [4]. BTGs differ clinically and radiologically from other gliomas and present clinically with personality changes, mental decline, memory impairment, emotional lability, and cognitive and behavioral impairments, with relative sparing of motor and sensory functions [56].
Recent advances in cancer treatment have improved the survival rate of brain tumor patients [7]. However, patients with brain tumors experience more residual neurological sequelae, such as weakness, and cognitive, psychological and behavioral impairments, than those with other types of cancers [7]. These disabling sequelae often interfere with daily life, including work-related activities, resulting in poor health-related quality of life. Unlike patients with strokes or traumatic brain injuries, there are little published research data or clinical guidelines available on rehabilitation of brain tumor patients [7].
In the present study, we report a case of a 17-year-old female patient with a BTGs with cognitive dysfunction and personality changes and subsequent rehabilitation treatment.
CASE REPORT
In September 2017, a 17-year-old female presented with bradykinesia, daytime somnolence, apathy, and insidious personality changes that had been ongoing for 1 month. The patient had been an outgoing and active person, but had gradually become less talkative, passive, and apathetic, with depressed mood and, decreased responses to external stimuli. In the previous 2 weeks, she had begun to show decreased verbal fluency. These symptoms progressed gradually until the patient was no longer able to perform normal activities of daily living (ADL).
Brain MRI showed an enlarged bilateral thalamus with an iso-signal intensity lesion on a T1-weighted image and a hyper-signal intensity lesion on a T2-weighted image. The MRI examination revealed the involvement of the thalamus, hypothalamus, right midbrain, and partial frontal lobes, but no hydrocephalus involvement (Fig. 1). Magnetic resonance (MR) spectroscopy of both thalami showed an increased choline/creatinine ratio, with a decreased N-acetyl aspartate peak (Fig. 2).
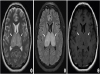 | Fig. 1(A) T2-weighted magnetic resonance imaging sequences show hyperintensity of both thalami. (B) Axial fluid-attenuated inversion recovery sequence shows prominent bilateral hyperintensity of both thalami. (C) T1-weighted image shows isointensity of both enlarged thalami.
|
 | Fig. 2(A) MR spectroscopy of the normal right frontal white matter (for comparison) shows a normal NAA peak. (B) MR spectroscopy of the thalamic lesions shows an increased Cho peak with a decreased NAA peak.MR, magnetic resonance; NAA, N-acetyl aspartate; Cho, choline.
|
The patient underwent a stereotactic biopsy. A histopathological examination revealed a high-grade glioma (WHO grade III). The patient was treated with dexamethasone and was referred for radiotherapy with 1,000 cGy (4 fractions) and 4,000 cGy (20 fractions), followed by chemotherapy. After radiotherapy and chemotherapy, the patient showed poor oral intake, fatigue, and general weakness. During 5 months of clinical follow-up, the patient was relatively stable and showed no significant changes in her clinical status, except for right visual disturbance and left hearing impairment. Chemotherapy, intensive rehabilitation, and follow-up brain MRI were planned.
The patient was admitted to the Rehabilitation Department for comprehensive rehabilitation. The results of a neurological examination at the time of admission revealed aphasia, disorientation, recent memory impairment, dyscalculia and left side dominant motor weakness. A language and cognitive evaluation, based on the Korean version of Western Aphasia Battery scores, suggested transcortical sensory aphasia with an aphasia quotient of 72.8 (56th percentile). The patient's score on the Korean version of the Montreal Cognitive Assessment was 10 points. On the manual muscle test (MMT) of the Medical Research Council, the patient was classified as grade II to III on the left side and MMT grade III on the right side. As the patient's standing balance was impaired due to left-sided weakness and lack of muscle endurance, she required assistance for ambulation.
A few months later, the patient underwent a gynecological evaluation, including a blood hormone level test for continued amenorrhea, and was diagnosed with hypogonadotropic hypogonadism. Thus, estrogen and progesterone therapy were started.
The patient underwent rehabilitation treatment for 5 weeks. The treatment included strengthening exercises, balance training, robotic-assisted gait training for left-sided weakness, especially hip abductor muscles, occupational therapy for ADL training, cognitive rehabilitation for memory deficits and speech therapy for aphasia. The patient's MMT grade, standing balance, and gait endurance improved as compared with these parameters upon admission. In terms of ADL, hygiene, dressing, ambulation, and chair/bed transfer improved and the patient's Modified Barthel Index score increased from 49 to 65. Furthermore, the patient's score on the Korean Mini-Mental State Examination increased from 17 to 23, showing improvement in orientation, calculation and memory functions.
The patient had showed low compliance with treatment on admission. In contrast, she exhibited increased motivation for treatment during and after rehabilitation therapy. In terms of language, there were improvements in responses to questions, frequency of spontaneous speech, comprehension, and phonation. There were also some improvements in symptoms of depression, anxiety, poor oral intake, and lethargy. After hospitalized rehabilitation, the patient was discharged home and performed everyday activities with the help of a caregiver.
DISCUSSION
BTGs are very rare brain tumors. Due to the prototypically large lesion size of BTGs, it can produce severe symptoms. Unlike patients with unilateral thalamic tumors, patients with BTGs show personality changes, cognitive impairment, and behavioral problems, although focal neurological deficits are generally rare. Early diagnosis is challenging, as the initial symptoms are relatively mild. Characteristic clinical presentations, a neurological examination, and an imaging evaluation are important in the differential diagnosis [56].
Clinical manifestations of BTGs can vary significantly, depending on the types and areas of the involved thalamic tracts. In the present case, personality changes, memory deficits, and cognitive impairment were observed and attributed to the involvement of mediodorsal thalamic nuclei, which receive inputs from the amygdala and temporal lobe [56]. These inputs are then projected to the frontal cortex, and anterior thalamic nuclei [56]. In general, motor deficit is rare in BTG case. The involvement of ventral lateral and ventral anterior nuclei of the thalamus is related to motor function. However, in the present case, we attributed left hemiplegia mainly to the lesion in the right midbrain, as the MMT score of right side markedly improved (grade 4) during hospitalization rehabilitation. In addition, the general condition of the patient recovered after rehabilitation, which included nutritional support and exercise. By contrast, the left side showed no significant improvement. A poor general health due to insufficient oral intake, cancer treatment, and long-term steroid administration may have affected the patient's motor grade at the time of admission. Hypothalamic lesions may lead to hormonal abnormalities, and the latter may explain the patient's hypogonadotropic hypogonadism [8].
BTGs show characteristic radiological findings, and MRI with contrast is more useful than computed tomography for the preoperative evaluation. Typical MRI features of high-grade gliomas are hypointense masses on T1-weighted images that enhance heterogeneously following contrast infusion, and hyperintense signal changes in the white matter on T2/fluid-attenuated inversion recovery (FLAIR) weighted imaging. These findings, including minimal focal gadolinium enhancement, were seen in the present case (Fig. 1) [5]. In general, MR spectroscopy is not routinely performed for the evaluation of brain tumors, but it can be useful when an imaging result is equivocal. MR spectroscopy may aid the differentiation of primary brain tumors from other non-neoplastic conditions (e.g., vascular diseases, infections, and inflammatory diseases) by analyzing the chemical composition in an anatomical area of interest. The presence of decreased N-acetyl aspartate and increased choline levels are suggestive of a neoplasm [9]. These findings were detected on MR spectroscopy in the present case.
The complex anatomy, deep location, and functional significance of the thalamus limit surgical approaches for a biopsy for histopathological confirmation, as well as for surgical resection [10]. Adjuvant therapies, including radiotherapy and chemotherapy, can be performed. However, no effective treatment has been reported to date and the prognosis remains poor for patients with BTGs. An analysis of 55 BTG cases published between 1967 and 2017 revealed a mean overall survival time of 13.0 months and a median overall survival time of 4.0 months [11]. Further analysis of prognostic factors indicated a significant correlation between overall survival and various factors such as the duration of symptoms (defined as the time between the first onset and diagnosis; ≥ 2 or < 2 months), glioma type (astrocytoma or glioblastoma multiforme), and WHO grade (low or high) [11]. The symptom duration in the present case was more than 2 months, and the patient was diagnosed with a high-grade glioma (WHO grade III). Thus, her prognosis was not good. However, the patient remained stable 9 months (May 2018) after her initial diagnosis in September 2017, except for some neurological symptoms (i.e., visual disturbance in her right eye and hearing impairment in her left ear).
The role of surgical and adjuvant therapies, such as radiotherapy and chemotherapy, in BTG cases remains unclear, and these do not tend to improve the survival of patients [1112]. In previous studies, the results of nonsurgical treatments, such as radiation therapy and chemotherapy, on patients with primary thalamic low-grade tumor and median age of 8 years at the time of diagnosis showed good prognosis [13]. The 10-year progression-free survival rate was 53% in the radiotherapy group and 34% in the chemotherapy group [13]. In the case of high-grade tumor patients, however, the effect of nonsurgical treatments on improvement of survival rate lacks evidence. And more recently, researches have shown that BTGs are thought to be molecularly distinct entities from unilateral high-grade glioma [14]. Therefore, further understanding of this rare type of tumor and its prognostic factors are essential and will require multicenter studies with larger populations. Such studies will need to include an analysis of molecular markers.
Patients with brain tumors experience multiple disease- and treatment-related complications, such as fatigue, sleep disturbance, cognitive impairment, memory deficit, motor weakness, and seizures [7]. The frequency and severity of disabling sequelae are high, especially in patients with WHO grade III or IV brain tumors, and the prognosis is poor [7]. As numerous adverse outcomes arise from active cancer treatment including surgery, radiotherapy, and chemotherapy, rehabilitation therapy is needed to maintain the patient's general health and ADL. According to a 2015 Cochrane review, rehabilitative exercise interventions improved health-related quality of life during and after active cancer treatment in cancer patients [15]. Although the study did not include patients with brain tumors, the complications (e.g., fatigue, sleep disturbances, depression, and physical functioning) reported were similar to those found in patients with brain tumors. The adage that medicine adds years to life and rehabilitation adds life to years applies in patients with a malignant brain tumor [16].
In conclusion, the clinical and radiological features of BTGs differ from those of unilateral thalamic tumors. Although BTGs are extremely rare, differentiation of patients with BTGs from those with other brain tumors is important. Personality changes and memory impairment can be indicators of BTGs. MRI is essential in the diagnosis of BTGs and reveals a hypo-intense to an isointense lesion on T1-weighted images and a hyper-intense lesion on T2/FLAIR images. Rehabilitation therapy can improve the patient's health-related quality of life by reducing cancer-related complications during or after active cancer treatment and maintaining independence in daily life as much as possible during the life span.
 XML Download
XML Download