

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Enterobacteriaceae, which is generally transmitted from person to person via hand carriage or contaminated water, is a highly infectious agent causing pneumonia, cystitis, pyelonephritis, sepsis, peritonitis, and meningitis, and is closely associated with poor clinical outcomes [1]. Multidrug-resistant (MDR) bacterial strains are spreading worldwide, especially with the advent of extended-spectrum β-lactamases-producing Enterobacteriaceae. Carbapenem, a broad-spectrum antibiotic, has become the preferred agent for MDR Enterobacteriaceae [2]. However, the risk of carbapenem-resistant Enterobacteriaceae (CRE) infection has been emphasized recently due to the increase in CRE colonization. Enterobacteriaceae develops resistance to different types of antibiotics, including carbapenem, thereby becoming a challenge to treat, with a consequent increase in mortality rate. Since 2004, when the first case of carbapenem-resistant Klebsiella pneumonia was reported in China, the prevalence of CRE in Asia increased steadily until 2012 [13]. Due to the increase in the outbreak of CRE infection, predominantly at tertiary hospitals in Korea [4], CRE sentinel surveillance was commenced in 2011, to detect antibiotic resistance. From 2017, CRE became classified as a class 3 legal infectious disease, hence, requiring a mandatory surveillance.
In a previous study on the risk factors of CRE colonization, immunologically compromised state was reported as a factor of increasing risk for both CRE infection and mortality [5]. According to another study, risk factors for CRE colonization include the administration of antibiotics and the use of central line devices [6]. During the recovery phase of stroke patients, their immune system is suppressed, thereby enhancing their susceptibility to complications such as pneumonia and urinary tract infection [7]. These complications were thought to be related to CRE colonization because frequent infections secondary to compromised immune system exposes the patients to frequent use of antibiotics and indwelling devices.
It is known that the most stroke recovery occurs in the first 3 to 6 months after onset [8]; in particular, there is a 48%–91% functional recovery within the first 3 months and a continuous improvement up to 6 months except for the lower extremity [9]. Therefore, early intensive and comprehensive rehabilitation is believed to be important. However, if CRE colonization is confirmed in a stroke patient, the isolation of the patient should be performed in accordance with current infection control policy. This may limit the implementation of active rehabilitation. Till date, no study has been conducted on the risk factors and prevalence of CRE colonization in stroke patients. Thus, this study was limited to the subacute group where most of the post stroke recovery occurs and carried out specifically to examine the prevalence and the risk factors of CRE colonization in post-stroke patients who were to undergo rehabilitation in Busan, Korea.
Materials and Methods
Study design and patients
We conducted a retrospective case-control study based on the medical records of all admitted patients who presented with CRE colonization from January 2017 to December 2018 at a 482-bed, medical center in Busan, Korea. In cases in which Enterobacteriaceae was detected from several cultures, the first positive result detected was included. We included patients who: 1) were radiologically diagnosed with a first time ischemic or hemorrhagic stroke within 6 months, which was defined as I60, I61, I62, and I63 in the International Statistical Classification of Diseases and Related Health Problems 10th Revision codes, 2) were diagnosed with a stroke in this hospital, 3) were isolated due to CRE colonization during the period of hospitalization, and 4) had CRE colonization occurring more than 48 hours after admission. We excluded patients who: 1) had uncertain CRE colonization period and disease duration, 2) had recurrent ischemic or hemorrhagic stroke, and 3) had simultaneous onset of ischemic and hemorrhagic stroke. The control group included stroke patients who were admitted to the same ward at the same time period and who had carbapenem-susceptible Enterobacteriaceae (CSE) colonization. The patients were age- (± 3 years) and sex-matched to the patients with CRE colonization and the ratio of CRE:CSE group was 1:1.02. While we tried to match all patients with respect to sex and age, we have not been able to achieve this completely because of the difficulty in obtaining sufficient numbers of hospitalized patients. This study was approved by the Institutional Review Board of Dong-Eui Medical Center (IRB No. DEMC-2019-01).
CRE definition
This study determined the antibiotic resistance based on the ‘Clinical and Laboratory Standard Institute's recommendation’ (M100-S27) in accordance with the Korea Centers for Disease Control and Prevention (KCDC) guidance on laboratory-based tests for legal communicable diseases [10]. CRE was indicated when a low susceptibility to carbapenem by Enterobacteriaceae organisms occurred. The standard used to determine CRE is the minimum inhibitory concentration of > 4 µg/mL for imipenem, meropenem or >2 µg/mL for ertapenem. Rectal swab was performed for CRE screening and was cultured on chromogenic agar plate. When specimens showed a positive culture test, additional tests, using the disk diffusion method and MacConkey agar culture were conducted for the differentiation and confirmation of the colony. In addition, Vitek 2 automated system (bioMerieux, Marcy-l'Étoile, France) was used for the susceptibility test. If the cultured organism was determined to be CRE, respective specimens were sent to the KCDC for polymerase chain reaction test for the detection of carbapenemase-resistant genes (K. pneumoniae carbapenemase [KPC], imipenemase [IMP], New Delhi metallo-β-lactamase [NDM]-1, Verona integron-encoded metallo-β-lactamase [VIM], oxacillinase [OXA]-48, and Guiana extended spectrum β-lactamase [GES]-5). Finally, DNA sequencing was performed to confirm the sub-type of the carbapenemase genes in all carbapenemase-producing Enterobacteriaceae (CPE) organisms.
Clinical characteristics and demographics of CRE colonization
In order to identify the risk factors of CRE colonization, the following were compared between the CRE and CSE groups: age, sex, type of stroke, body mass index (BMI) at admission, National Institutes of Health stroke scale (NIHSS) at admission [11], Charlson Comorbidity Index (CCI) [12], admission to intensive care unit (ICU), use of enteral feeding tube, use of urethral Foley catheter, use of tracheostomy tube, use of central venous catheter, ambulatory ability, duration of antibiotic intake. The duration of antibiotic intake was divided into 3 groups; these were unused, used for 1 to 14 days, and used for 15 or more days. The use of enteral feeding tube, tracheostomy tube, central venous catheter, and the duration of antibiotic intake were counted from the day of admission to the day CRE colonization was first confirmed. Ambulatory ability was determined as the date when CRE colonization was confirmed. In this study, no detailed assessment of Ambulatory ability was made because a majority of patients were not able to walk.
Statistical analysis
Categorical variables were expressed as percentages and frequencies, and numerical variables as mean ± standard deviation (SD). To compare the clinical characteristics of patient groups, χ2 test or Fisher's exact test was used for categorical variables while Mann-Whitney's U test was used for continuous variables. We used Shapiro-Wilk's test to see if the data distribution was normal. The effect of independent variables on CRE colonization was analyzed using the univariate and the multivariate logistic regression analysis. For multivariate logistic analysis, variables with a p value of < 0.05 in univariate analysis were entered into the model selection procedure using a stepwise backward process. All statistical analyses were carried out using SPSS 24.0 (IBM Corp., Armonk, NY, USA) and p values < 0.05 was considered significant.
RESULTS
Prevalence of CRE colonization and microbiologic data
During the 105,327 patient-days, 105 cases of CRE were observed in 451 specimens detected in 3,657 inpatients; the prevalence of CRE was 2.9% (105/3,657). Of these, 105 patients were previously diagnosed with stroke, and only 53 of them had stroke within 6 months. In this study, however, only 43 patients met the inclusion criteria. Ten patients were excluded based on the following reasons: 8 patients, due to confirmed CRE colonization within 48 hours of admission and 2 due to simultaneous onset of ischemic and hemorrhagic stroke. The average period of CRE detection was 34.9 days from admission. CRE was cultured in stool (69.8%), urine (20.9%), sputum (9.3%), and blood (2.3%), whereas CSE was cultured in urine (77.3%), sputum (16%), and stool (2.3%). The distribution of CRE species are shown in Table 1. Most of the CRE strains detected were K. pneumoniae (34 specimens), Escherichia coli (4 specimens), and Proteus mirabilis (1 specimen). In the CSE group, those detected included E. coli (18 specimens), K. pneumoniae (11 specimens), Enterococcus faecalis (9 specimens), Enterobacter aerogenes (2 specimens), P. mirabilis (3 specimens), Proteus penneri (1 specimen), Citrobacter freundii (1 specimen), and Serratia marcescens (1 specimen). In total, there were 27 specimens of carbapenemase-producing CRE organisms: 24 specimens of KPC in K. pneumoniae, 2 specimens of KPC in E. coli, and 1 specimen of NDM in E. coli.
Table 1
Distribution of Enterobacteriaceae species isolated among CRE and CSE
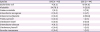
Values are presented as number (%).
There were concurrent isolates of Klebsiella and P. mirabilis (1 specimen), Klebsiella and C. freundii (1 specimen), and E. faecalis and S. marcescens (1 specimen) in CSE group.
CRE, carbapenem-resistant Enterobacteriaceae; CSE, carbapenem-susceptible Enterobacteriaceae.
![]()
Demographic data and comparison between CRE and CSE group
The study involved a total of 87 patients including 43 CRE patients and 44 CSE patients. As shown in Table 2, both groups had similar baseline characteristics including sex, age, and type of stroke. The mean CCI score in the CRE group was higher at 3.84 (SD, 1.82), but not significantly different from that of the CSE group; but the CRE group had a significantly higher incidence of renal failure (p = 0.012). In the CRE group, the use of enteral feeding tube (p = 0.07), urethral Foley catheter (p = 0.027), tracheostomy tube (p = 0.02), and central venous catheter (p = 0.02) were more than in the CSE group. Admission to ICU (p = 0.001) and use of antibiotics were more frequent in the CRE group than in the CSE group. Risk factors of CRE colonization in the univariate analysis included the use and duration of antibiotic intake, admission to ICU, and the use of enteral feeding tube, tracheostomy, and central venous catheter (Table 3). Tracheostomy was found to have a significant effect on CRE colonization in univariate analysis (odds ratio [OR], 14.78; 95% confidence interval [CI], 1.81–120.42, p = 0.012); however, the result should be interpreted with caution, because it only applied to one patient in the CSE group. Thus, tracheostomy was excluded from among the risk factors in the multivariate analysis due to the small sample size.
Table 2
Patient demographic and clinical characteristics by CRE colonization status

Data are presented as number (%) or mean ± SD. Shapiro-Wilk's test was employed for test of normality assumption.
CRE, carbapenem-resistant Enterobacteriaceae; BMI, body mass index; NIHSS, national institutes of health stroke scale; CCI, Charlson Comorbidity Index; DM, diabetes mellitus; SD, standard deviation; TMP-SMX, trimethoprim/sulfamethoxazole; ICU, intensive care unit.
*p values were derived from χ2 test; †p values were derived from Fisher's exact test; ‡p values were derived from Mann-Whitney's U test.
![]()
Table 3
Univariate analysis of patient clinical characteristics as potential risk factors for CRE colonization

For multivariate analysis, logistic regression analysis was used. Variables with a p value of < 0.05, on univariate analysis, were entered into the model selection procedure using a stepwise backward process. Variables were 2-sided, and p values < 0.05 were considered statistically significant.
CRE, carbapenem-resistant Enterobacteriaceae; TMP-SMX, trimethoprim/sulfamethoxazole; ICU, intensive care unit; OR, odds ratio; CI, confidence interval; Ref, reference group; N/E, not estimable since no CRE colonization was observed in a certain subgroup due to the small sample size.
![]()
In multivariate analysis, the use and duration of antibiotic intake (OR > 2 weeks vs. none = 9.82; 95% CI, 2.29–42.17; p = 0.002 and OR ≤ 2 weeks vs. none = 5.52; 95% CI, 1.28–23.75; p = 0.022) and admission to ICU (OR, 3.49; 95% CI, 1.05–11.63; p = 0.042) were the independent factors of CRE colonization (Table 4).
Table 4
Multivariate analysis of the association between patient clinical characteristics and CRE colonization

CRE, carbapenem-resistant Enterobacteriaceae; OR, odds ratio; CI, confidence interval; Ref, reference group; ICU, intensive care unit.
![]()
DISCUSSION
The prevalence of CRE is known to be affected by geographical factors and has been reported approximately at 10% in Uganda and Mexico [1314]; however, in Asia, the prevalence of CRE is as low as 0.6% [13]. In Korea, prevalence of CRE varies; 0.3% prevalence from rectal swab was reported among patients who were admitted to the ICU in a tertiary hospital [15]. In 2013, similar study on stool culture reported a prevalence of 7.5% [16]. Compared with the 2 former studies which involved ICU patients in tertiary hospitals only, Lee et al. reported CRE prevalence of 1.6% that included ICU and general ward patients in a mid-sized community-based hospital [4]. In this study, the prevalence of CRE in stroke patients was higher than that in all previous studies except for one. Because previous studies were for all patient groups, these results suggest that stroke may be one of the risk factors of CRE colonization; however, further research comparing CRE colonization in stroke patients and non-stroke patients is required to demonstrate the relationship between stroke and CRE colonization.
Previous studies report that the risk factors of CRE colonization include history of admission to ICU, abdominal invasive procedure, chemotherapy and radiation therapy, length of central venous catheter and biliary drainage catheter, tracheostomy, prior hospital stay, history of antibiotic intake, and old age [17181920]. Particularly, glycopeptides, cefoperazone, fluoroquinolone, and carbapenem were among the antibiotics listed as independent risk factors [19202122]. Asai et al. [23] evaluated the comorbidity and performance status (PS) based on the CCI and Eastern Cooperative Oncology Group (ECOG) PS, respectively. CCI score of ≥ 3 with PS of 2–4 (ECOG) were considered to be independent risk factors [23]. ECOG PS is a tool for quantification of activities of daily living and the degree of physical health during the clinical treatment of patients with cancer [24]. In this study, NIHSS score, CCI score, and ambulatory ability were not statistically significant; however, the use of enteral feeding tube, urethral Foley catheter, tracheostomy, and central venous catheter were statistically significant. In univariate analysis, cephalosporin, fluoroquinolone, and piperacillin/tazobactam showed significant association when the CRE group and the CSE group were compared. According to another study including ICU patients [25], the risk factors of CRE colonization included ≥ 15 days of cephalosporin or carbapenem intake. In this study, in multivariate analysis, statistically significant differences were found in those with antibiotics use for at least one or more days compared with the group with no antibiotic use. The OR of the groups with 1 to 14 days of antibiotic intake and those with ≥ 15 days of antibiotic intakes were 5.52 (CI, 1.28–23.75) and 9.82 (CI, 2.29–42.17), respectively. The results indicated that the duration of antibiotic intake was also a significant risk factor. However, due to the wide CI, there is need for caution in the interpretation. The use of antibiotic is inevitable for the treatment of infections, and stroke patients are at higher risk of infection in the first week post-stroke [26]. The most common infections found in acute stroke patients are pneumonia and urinary tract infection, and it takes ≥ 3 working days to identify the causative microorganisms. The delay while awaiting the result of diagnostic tests especially for patients with severe infection should be avoided because their prognosis is determined by the quick initiation of treatment; hence, patients are usually administered with empirical treatment [27]. Once the bacterial culture has established the causative microorganism, by principle, broad spectrum antibiotics should be replaced with narrow spectrum antibiotics. In actual clinical practice, however, there are many cases where the causative bacteria cannot be identified, hence, in such patients, the use of the initial antibiotics tend to be prolonged. Thus, overuse of broad-spectrum antibiotics results, eventually leading to antibiotic resistant bacteria [28]. In post-stroke infection, it may be important to apply a de-escalation strategy, with a shift in empirical antibiotics to the narrow-spectrum antibiotics after the identification of the causative microorganism following the culture test. In addition, antimicrobial stewardship, a systematic management of antibiotics to maintain the clinical outcome while reducing antibiotic resistance should be applied. To reduce the general use of antibiotics, it is also necessary to commence prevention intervention measures such as screening test for aspiration, video fluoroscopic swallowing study for the proper treatment of dysphagia, maintenance of good oral hygiene, frequent changes of patients positions to the sitting position, and replacement of indwelling catheters with intermittent catheters as soon as possible.
In a previous study, admission to ICU was reported as a risk factor for CRE colonization [17]. Furthermore, ICU stays and poor functional status were found to be risk factors of carbapenem-resistant K. pneumoniae acquisition [29]. Admission to ICU was also identified as an independent risk factor of CRE colonization in this study. In general, stroke severity is known as a factor in determining ICU admission [11], and another studies reported that the NIHSS score was an independent risk factor for ICU admission after IV thrombolysis in patients with acute ischemic stroke [30]. It was thought that stroke severity would also affect CRE colonization, but in this study the average NIHSS score was slightly higher in the CRE group, but not a significant factor. These results suggest that in stroke patients, admission to the ICU rather than stroke severity is important for CRE colonization. Therefore, if possible, reducing ICU admission and preventing CRE transmission in all stroke patients admitted to the ICU thought to be important to reduce CRE colonization. According to another study, ICU admission for mild and moderate stroke patients was not significantly different in treatment outcomes [11]. Therefore, admission to ICU in patients with mild and moderate stroke should be carefully assessed for the risk-benefit between the risk of CRE colonization and the need for intensive care. One study provided evidence that KPC-producing K. pneumoniae was successfully controlled based on the reduced prevalence of KPC-producing isolates from 21% to 0% in the long-term acute care hospital due to the interventions applied. Such interventions included decolonization of patients' skin, improved cleaning of environmental surfaces, admission and surveillance cultures and contact precautions [31]. In our study, 30 of 43 (70%) CRE colonization were identified in the ICU. If the interventions presented in the previous study are also applied to patients admitted to ICU, it is expected to be effective in reducing CRE colonization. Also, an analysis on the effect of further infection control is necessary.
According to the KCDC (2017), among CRE strains, 65.5% was identified as CPE, of which KPC was the highest in Korea at 69.9%, followed by NDM at 26.9%, OXA at 7.6%, GES at 1.4%, VIM at 1.3%, and IMP at 0.3% [32]. In our study, carbapenemases were noted in 62.8% (27/43) of CRE colonization cases, with a CPE colonization to CRE colonization ratio similar to that reported by the KCDC. However, apart from the detection of NDM, most cases of CPE were detected as KPC in the case of stroke patients. The difference found in the distribution of CPE colonization in this study compared with that in the KCDC report could have been influenced by the time of CRE colonization detection. Previous study detected CRE after an average of 34 days of hospital stay, which was determined to be the late-onset nosocomial complication [33]. Another study reported the average period of CRE detection to be after 25 days of hospital stay and suggested nosocomial bacterial infection because the genotyping of 8 CRE isolates were similar, although the patients were transferred from 7 different acute care hospitals [34]. In this study, the average period of CRE detection was 34.9 days, which is similar to that of previous studies, suggesting that nosocomial bacterial complication is the main cause. In the case of nosocomial outbreak of KPC in China, most of them have been caused by clonal expansion [35]. In another study, the main mechanism of CPE transmission the horizontal gene transfer based on the evidence of blaKPC gene transfer between plasmids and plasma mobility between bacteria [36]. In our study, the majority of patients with CP-CRE involved blaKPC-2 gene in K. pneumoniae, and the main mechanism of transmission was suggested to be clonal expansion, while some were influenced by horizontal transfer.
The present study had several limitations. First, this research was conducted in a single hospital. Secondly, this is a retrospective analysis. Thirdly, only a small sample size was included in the case control study, hence, it is difficult to generalize that the risk factors determined in this study pertain similarly to all other patient groups. Fourth, due to the limitations of cost, CRE organism screening test were only performed in high-risk patients (transferred from tertiary hospital, or nursing hospital, or previous history of CRE colonization) and patients who were admitted to ICU. If the screening test was positive for CRE organism, the specimens were then confirmed by culture test. This indicates that those patients without the screening test may have been CRE carriers from the day of admission. However, previous studies have shown that it is quite unlikely for low-risk patients to carry CRE strains at the time of admission [37]. Therefore, the impact of this factor on research output is thought to be minimal. This study is significant as the first study demonstrating the risk factors of CRE colonization in stroke patients within the first 6 months post stroke.
CONCLUSION
The use and duration of antibiotic intake and admission to ICU were determined as independent risk factors for CRE colonization in stroke patients within the first 6 months post-stroke. Hence, we suggest antimicrobial stewardship while avoiding unnecessary antibiotic administration, and activities to prevent post stroke infection. In addition, reducing ICU admission and preventing CRE transmission in all stroke patients admitted to the ICU thought to be important to reduce CRE colonization. Future prospective research involving a larger sample size, which strictly applies the screening test and active surveillance from the day of admission is essential for a better understanding of the risk factors.
 XML Download
XML Download