

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cerebral white matter hyperintensity (WMH) is a usual finding on magnetic resonance imaging (MRI) in elderly persons and patients with cerebrovascular diseases. WMH is found in 21% of individuals 64 years of age, and 94% of individuals 82 years of age [1]. The etiology of WMH is secondary to small-vessel ischemic changes. Arteriolosclerosis, myelin pallor, and Braak score were significantly associated with increased WMH accumulation [2]. Previous studies have suggested that WMH is a risk factor dementia after stroke [3]. In addition, one study determined that WMH is related with executive dysfunction [4].
Stroke rehabilitation is a progressive, goal-orientated practice to achieve optimal physical, cognitive, emotional and functional activity level [5]. Many factors can affect the rehabilitation outcome after stroke such as medical history, site of lesion, age, sex, ethnicity, visual impairments, aphasia, depression, and cognition [6789].
There have been few studies investigating the association between WMH and functional gains during inpatient rehabilitation. We assumed that WMH causes cognitive and executive dysfunction that can affect functional outcomes in ischemic stroke patients. Therefore, the aim of the study is to examine the effect of WMHs on the functional improvement using the Korean version of Modified Barthel Index (K-MBI) during inpatient stroke rehabilitation.
MATERIALS AND METHODS
Subjects
This was a retrospective study of patients with middle cerebral artery (MCA) territory ischemic stroke. The data were collected from medical records of patients who were admitted to Kyung Hee Hospital for ischemic infarction, between January 2015 and May 2017. The patients were delivered from an acute care department (e.g., internal medicine, neurology, neurosurgery, and intensive care unit) at Kyung Hee Hospital or from other neighboring hospitals. This study was approved by the Institutional Review Board (IRB) of Kyung Hee University Hospital (IRB No. 2019-05-074).
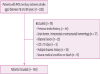
The inclusion criteria for the study were 1) MCA territory ischemic stroke confirmed by MRI; 2) Patients' age between 18 and 80 years; and 3) Stable medical status being able to receive active rehabilitation treatment (Fig. 1). Exclusion criteria were 1) Evidence of a previous stroke by patient's history or computed tomography scan; 2) Evidence of brain tumor, trauma, intracranial, or extracranial hemorrhage; 3) Bilateral lesions; 4) Length of stay (LOS) in the rehabilitation department less than 10 days assuming that the extent of rehabilitation in such a short period is limited; 5) Presence of other acute disabilities such as multiple trauma history; and 6) Presence of additional severe medical conditions restricting active rehabilitation (e.g., cardiac failure with New York Heart Association functional capacity stage III–IV, severe chronic lung disease necessitating a constant use of oxygen), or transfer to an acute care departments due to complications and/or death while hospitalized at the rehabilitation department.
The patients undergo, on average, 6 hours of physical therapy and 6 hours of occupational therapy a week (6 days/week). Demographic data and history of premorbid risk factors were collected from medical records.
Outcome measure
Functional and cognitive status assessment
Functional status was assessed by the K-MBI score. The K-MBI is a measure of the activities of daily living (ADL) scoring from 0 to 100 and is valid and reliable in a patient with stroke [10].
Cognitive status was evaluated by Korean version of Mini-Mental State Examination (K-MMSE) which score ranged from 0 to 30. This tool is a brief instrument used to assess cognitive abilities [11].
The K-MBI and K-MMSE were administered to all patients within 72 hours after admission by the rehabilitation team (composed of a physiotherapist, an occupational therapist). The same team evaluated K-MBI and K-MMSE 3 days before discharge. The team administering the K-MBI and K-MMSE did not include the treating physicians. Other variables that were examined included sex, age, the time interval from stroke onset to admission, laterality of stroke, LOS, National Institutes of Health Stroke Scale (NIHSS), and comorbidities such as hypertension, diabetes, dyslipidemia.
K-MMSE gain
The cognitive improvement was assessed by the difference between the K-MMSE score at admission and K-MMSE score at discharge.
Absolute functional gain (AFG) and absolute functional efficiency (AFE)
Functional gains were demonstrated by using absolute and relative methods determined from the K-MBI score. AFG is the K-MBI score gain (ΔK-MBI). AFE reflects AFG per day [12].

(DC, discharge; adm, admission)
Rehabilitation effectiveness (REs) and relative functional efficiency (RFE)
The REs was used to calculate relative gains. REs was suggested firstly by Heinemann et al. [13] expressed as a percentage indicating the proportion of potential improvement achieved during rehabilitation.


(max, maximum possible score)
WMH classification
Each MRI study included fluid-attenuated inversion recovery images at the acute stroke phase. We applied the simple modified Fazekas rating scale [14]. The modified Fazekas ranges from grade 0 to grade 3. Grade 1 was characterized by punctate lesions in the deep white matter. The maximum diameter is 9 mm for a single lesion and 20 mm for grouped lesions. Grade 2 was an early confluent lesion of 10–20 mm single lesion and grouped lesions with a diameter of > 20 mm with no bridges connecting individual lesions. Grade 3 was defined by single lesions or confluent lesions of ≥ 20 mm in diameter. All participants were divided into mild and severe groups based on the severity of WMH according to Fazekas scale. Patients with Fazekas scale 0, 1 was sorted as mild WMH group. Severe WMH group was classified by Fazekas scale 2, 3. It was performed by one skilled physician in the department of rehabilitation medicine.
Statistical analysis
Statistical analyses were carried out using the Statistical Package for the Social Sciences (SPSS) version 18.0 for Windows (SPSS Inc., Chicago, IL, USA). The Kolmogorov Smirnov test was applied to assess whether the parametric values were normally distributed. All parametric data were shown to be normally distributed.
We compared the values between the 2 groups (mild WMH group and severe WMH group) according to the severity of WMH. Independent t-tests were performed for continuous variables to compare values between the mild WMH group and severe WMH group. Chi-square tests were conducted for categorical variables. Association between the functional and cognitive outcomes and severity of WMH was analyzed using generalized linear model adjusted for age, sex, stroke lesion side, initial NIHSS, and LOS. A p value < 0.05 was considered significant.
RESULTS
General characteristics
A total of 559 patients were consecutively admitted to Kyung Hee Hospital between January 2015 and May 2017. Of 559 patients, 160 patients fulfilled the inclusion and exclusion criteria and were classified to mild WMH group (n = 80) and severe WMH group (n = 80). In a mild group, 16 patients were Fazekas scale grade 0 and 64 patients were grade 1. In a severe group, 59 patients were grade 2 and 21 patients were grade 3. There was no significant difference in age, sex, stroke lesion side, hypertension, diabetes, and dyslipidemia between mild and severe groups (Table 1).
Table 1
General characteristics between mild WMH and severe WMH groups
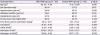
Values are presented as number of patients or mean ± standard deviation.
WMH, white matter hyperintensities; LOS, length of stay; NIHSS, National Institutes of Health Stroke Scale; K-MBI, Korean version of Modified Barthel Index; K-MMSE, Korean version of Mini-Mental Status Examination.
*Independent t-tests was conducted for continuous variables; †The χ2 tests was conducted for categorical variables.
The mean duration of time from the onset of stroke to admission was 29.5 ± 10.9 days in mild WMH group and 27.4 ± 10.3 days in severe WMH group. LOS was 31.67 ± 8.99 in mild WMH group and 31.58 ± 7.92 in severe WMH group. There were no significant differences between the 2 groups. Initial NIHSS score also showed no significant differences between the 2 groups (p = 0.730). In mild WMH group, admission K-MBI score was 27.08 ± 19.93 and admission K-MMSE was 22.18 ± 8.99. In severe WMH group, admission K-MBI score was 15.42 ± 13.13 and admission K-MMSE was 18.77 ± 7.13, which was lower than mild WMH group. However, there were no statistical differences. At discharge, K-MBI score is 47.75 ± 21.25 in mild WMH group and 22.83 ± 15.23 in the severe group. Discharge K-MMSE is 25.76 ± 5.07 in mild WMH group and 20.20 ± 6.84 in the severe group. There was a significant difference in discharge K-MBI and discharge K-MMSE between mild and severe WMH group (Table 2).
Table 2
Functional and cognitive outcomes between mild WMH and severe WMH groups
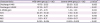
Values are presented as mean ± standard deviation.
WMH, white matter hyperintensities; K-MBI, Modified Barthel Index; K-MMSE, Korean Mini-Mental Status Examination; AFG, absolute functional gain; AFE, absolute functional efficiency; RES, rehabilitation effectiveness; RFE, relative functional efficiency.
*p < 0.05, between mild WMH and severe WMH groups.
Cognitive improvement between the mild WMH group and the severe WMH group
K-MMSE gain during inpatient rehabilitation was 3.57 ± 5.70 in mild WMH group and 1.43 ± 1.50 in severe WMH group, which showed significantly higher cognitive improvement in mild WMH group than severe WMH group (p < 0.05) (Table 2). The generalized linear model analyses showed association between discharge K-MMSE and severity of WMH. However, there was no significant association between K-MMSE gain and severity of WMH (Table 3).
Table 3
Generalized linear model on association of functional and cognitive outcomes with severity of WMH
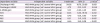
Adjusted by age, sex, stroke lesion side, initial NIHSS, and LOS.
WMH, white matter hyperintensities; CI, confidence interval; K-MBI, Modified Barthel Index; K-MMSE, Korean Mini-Mental Status Examination; AFG, absolute functional gain; AFE, absolute functional efficiency; RES, rehabilitation effectiveness; RFE, relative functional efficiency; NIHSS, National Institutes of Health Stroke Scale; LOS, length of stay.
*p < 0.05.
Functional outcome between the mild WMH group and the severe WMH group
AFG were 20.67 ± 10.48 in mild WMH group and 7.42 ± 6.46 in severe WMH group. AFG in mild WMH group was significantly higher compared to severe WMH group (p = 0.001) (Table 2). In addition, patients in mild WMH showed significantly higher AFE compared to severe WMH group (p = 0.003). RES and RFE showed a significantly higher score in mild WMH group compared to severe WMH group. In the generalized linear model analyses, there was an association between functional outcomes such as discharge K-MBI, AFG, AFE, RES, RFE and severity of WMH after adjusting age, sex, stroke lesion side, initial NIHSS, and LOS (Table 3).
DISCUSSION
This study demonstrated that functional improvement in ischemic stroke patients with severe WMH patients was significantly lower compared to those with mild WMH. The association between cognitive impairment and WMH has been reported [3]. However, there are few studies investigating the impact of WMH on the functional gain during inpatient rehabilitation. To our knowledge, this is the first study that examines the effect of WMH on rehabilitation outcomes of ischemic stroke patients during inpatient rehabilitation by using K-MBI for assessing outcome.
Clear evidence exists that WMH leads to cognitive decline and is associated with an increased risk of Alzheimer's disease in elderly persons [15]. WMH, together with lacunar infarcts and cerebral microhemorrhages, is considered to be the primary pathology in subcortical ischemic vascular dementia [16]. In non-demented elderly subjects, WMH has been associated with cognitive impairment. The Rotterdam Scan study examined the relationship between periventricular and subcortical WMH and cognitive function in 1,077 elderly population [17]. They suggested that both periventricular and subcortical WMH were related to all neuropsychological measures such as psychomotor speed, memory performance, and global cognitive function [17]. Our findings are also consistent with previous studies. In our study, discharge K-MMSE during inpatient stroke was higher in mild WMH group than severe WMH group. This result indicates that the severity of WMH may affect the cognitive improvement of ischemic stroke patient during inpatient rehabilitation.
One study investigated the impact of WMH on short-term functional outcomes at 3 months and long-term mortality in ischemic stroke patients with large artery atherosclerosis [18]. There was no significant difference in functional outcome between patients with and without severe WMH at 3 months [18]. To assess the functional outcome, they used the modified Rankin scale, which does not take into account specific basic ADL, as the K-MBI does. Moreover, they did not consider the presence of rehabilitation. In our study, we used K-MBI to consider ADL. The results showed that the functional gain of the mild WMH group was better than that of the severe WMH group after adjusting age, sex, stroke lesion side, initial NIHSS, and LOS.
In addition to cognitive impairment, global functional decline consistently has been reported to be associated with age-related changes in white matter [19]. The Leukoaraiosis And DISability study, a multi-center European collaboration established in 2000, investigated whether age-related groups in white matter are an independent determinant of functional decline in older people [19]. They used instrumental ADL scale that included eight items: the ability to use the telephone, shopping, preparation of food, housework, laundry, transportation, responsibilities for own medications, and ability to handle finances. This study suggested that age related changes in white matter independently predicted rapid global functional decline in non-disabling older adults. Other studies reported significant associations between gait and balance dysfunction and WMH [2021]. A 4-year-follow-up study suggested that in the eighth and ninth decades of life, gait and balance dysfunction and falls were associated with increasing periventricular WMH [22]. In this study, there was a difference in functional gain measured by K-MBI according to WMH severity. This suggests that the severity of WMH may affect daily living activity during rehabilitation in stroke patients.
In patients with the same diagnosis, the rehabilitation outcome varies [6]. Some patients show little improvement after comprehensive rehabilitation. On the other hand, some other patients show great functional recovery after the same treatment. This is because stroke rehabilitation can be affected by many factors such as medical comorbidities, site of lesion, cognitive status, and many demographic variables [6789]. In addition to this, our study emphasized that the severity of WMH must be considered when determining the rehabilitation aims and predicting the outcome.
In our study, risk factors that can affect the prevalence of WMH such as age, arterial hypertension, diabetes, and dyslipidemia showed no statistically significant differences between groups, so we assumed that their impact on functional outcome was little. In previous studies, cardiovascular risk factors such as age, hypertension, and diabetes have been reported to be associated with the presence of WMH [232425]. Our study did not divide the group into the presence of WMH. Because we divided the group according to the severity of WMH, we think that it differs from the previous study results.
A Korean study in patients with stroke found an association between the frequency of severe WMH and stroke subtype [26]. Patients with large artery disease had a higher prevalence (55.4%) of WMH than those with lacunar stroke (30.3%) or cardioembolic stroke (14.3%). Because stroke subtype may influence the presence of WMH in patients with ischemic stroke, we selectively analyzed patients who had ischemic strokes in the MCA territory, which is one of the strengths of our study.
This study has limitations. First, this is a single center study. The sample size in this study was small but the effectiveness was still significant according to the effect size. Second, all other potential correlates or confounding factors that could affect outcomes were not considered. Third, stroke lesion location and size affect stroke rehabilitation. To minimize this, stroke lesion was restricted to MCA territory. However, it was difficult to assess size of stroke lesion accurately. The lack of precise control of this point is a limitation of the study. Additional studies will be needed in the future. Finally, we focused on inpatient rehabilitation outcome, so long-term functional outcome needs to be assessed in future studies.
In conclusion, our study emphasized the impact of the severity of WMHs on functional improvement in ischemic stroke patients during inpatient stroke rehabilitation. The WMHs might be considered as one of many factors that can affect functional recovery in the rehabilitation of stroke patients.
 XML Download
XML Download