

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Dementia has emerged as one of the most critical health challenges throughout the world. By the World Health Organization report, the number of people with dementia worldwide in 2010 was an estimated 35.6 million and will increase to 115.4 million in 2050 [1]. Also in Korea, the estimated prevalence of dementia was 9% in 2012, it will become 15% by 2050 [2].
Swallowing function in elderly was known as physiologic decrement; reduced tongue driving force, pharyngeal shortening, and impairment of pharyngeal constriction [345]. Moreover, swallowing function in patients with dementia were reported by the higher incidence of clinical or subclinical dysphagia [67]. Previous study showed the oral phase dysfunction was important patho-mechanism in progression of dysphagia in dementia [7]. Delayed oral transit based on a decrease in the perception in mouth and motor dysfunction of the tongue were typically reported in dysphagia with dementia [7]. Among the oral phase dysfunction, higher frequency of oral transit delay of liquids but a lower frequency of difficulty in mastication and bolus formation were typically reported in dysphagia with Alzheimer's disease (AD), may be based on sensory dysfunction and difficulty in movement of the tongue [78]. Dysphagia in early-stage AD is characterized by delayed onset of the pharyngeal swallow and reduced lingual movement [9], while moderate AD adds difficulty with oral preparation of the bolus, pharyngeal clearance, upper esophageal sphincter opening [10]. In contrast with AD, more difficulty in bolus formation and mastication frequently occurred in dysphagia with vascular dementia (VaD) based on disruption of the corticobulbar tract [711]. In late stage of dementia, the pseudobulbar palsy, orofacial apraxia and loss of desire would contributed the progression of dysphagia in AD and VaD [1213].
Although dysphagia is an important heath problem and one of determinant of quality of life in patients with dementia, the neurophysiologic changes of dysphagia in dementia have not been fully uncovered, yet. Considering previous reports, dysfunction in oral phase would be a key factor of pathophysiology in dysphagia with dementia [7]. Thus, we investigated the changes of strength of tongue lip and pharyngeal muscles for revealing the changes in oral phase dysfunction in patients with dementia and dysphagia.
MATERIALS AND METHODS
Study design and participants
For this retrospective cross-sectional clinical study, 30 right-handed subjects with dementia and dysphagia were recruited from a rehabilitation clinic between January 2016 and May 2019. All subjects were diagnosed with dementia and were referred for recent developing dysphagia symptoms to the Rehabilitation Medicine of St. Vincent's Hospital of the Catholic University of Korea, and met the following criteria: 1) The patients with Alzheimer dementia were diagnosed by the National Institute of Neurologic and Communication Disorders and Stroke/Alzheimer Disease and Related Disorders Association criteria for probable AD and had a score on the Clinical Dementia Rating (CDR) scale of 1 [141516], or the patients with VaD met the diagnostic criteria for VaD as determined by the Diagnostic and Statistical Manual of Mental Disorders–fourth edition and fulfilled imaging criteria for subcortical VaD proposed by Erkinjuntti et al. [1718] and 2) ability to follow verbal instructions. Exclusion criteria were 1) Surgical history or disease of head and neck and 2) other neurologic or psychiatric conditions (including other forms of dementia or depression). The control data were collected from normal healthy volunteers for establishing normal reference values of our clinic, previously. The study protocol was reviewed and approved by the Institutional Review Board (IRB) of Catholic University, College of Medicine the need for informed consent was waived by the board.
Assessment
The demographic and clinical data of all subjects were assessed; cognitive function was assessed using the Mini-Mental State Examination (MMSE) and CDR [19], clinical assessments consisted of the Iowa Oral Performance Instrument (IOPI) and surface electromyography (sEMG) with Vital stim plus. The IOPI Model 2.3 use to measure pressure in tongue and lip by 10 years experienced occupational therapist with routine protocol [20]. The sEMG was tested for the suprahyoid muscle complex during swallowing with routine protocol via VitalStim®plus (Performance health, Warrenville, IL, USA) [21].
Statistical analysis
All variables were presented as mean ± standard deviation. Mann-Whiney U test and χ2 test were used to characterize variables according to dementia type. Kruskal-Wallis test and Mann-Whitney U test with the Bonferroni correction were used for comparisons between dementia subgroups and control. The Kruskal-Wallis test was 2-tailed, and p values < 0.05 were deemed significant. The Mann-Whitney U test with the Bonferroni correction were 2-tailed, and p values ≤ 0.0166 were deemed to be significant. All statistical analyses were performed using SPSS software for Windows (ver. 21.0; SPSS, Chicago, IL, USA).
RESULTS
The demographic and clinical characteristics in all subjects were shown in Table 1. The mean age of dementia was 76.87 ± 7.30 and mean of MMSE was 14.90 ± 6.75. The age of dementia group was older than those of control group. The demographic and clinical characteristics according to dementia type were shown in Table 2. There was no statistically significant difference between dementia types for all variables.
Table 1
Demographic and clinical characteristics in all subjects
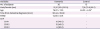
Values are mean ± standard deviation or number (%). The age between dementia and control was analyzed by Mann-Whiney U test.
MMSE, Mini-Mental State Examination; CDR, Clinical Dementia Rating.
*All p < 0.05.
![]()
Table 2
Comparisons according to dementia type
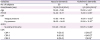
Values are mean ± standard deviation or number (%). Age, MMSE, IOPI, and sEMG values were analyzed by Mann-Whiney U test. The distribution by sex and CDR were analyzed by the χ2 test.
MMSE, Mini-Mental State Examination; IOPI, Iowa Oral Performance Instrument; sEMG, surface electromyography; CDR, Clinical Dementia Rating.
*All p > 0.05.
![]()
There was no difference between IOPI and sEMG of Vital stim plus among 3 groups of dementia (p > 0.05, Table 3). The values of tongue and lip IOPI from all 3 dementia groups were significantly lower than values of control (Table 3). The comparisons for values of tongue and lip IOPI among 3 dementia group were not significantly different from each other. The values of sEMG for suprahyoid muscles were not different between 3 dementia groups and control (Table 3).
Table 3
Comparisons among all 3 dementia group with control

Values are mean ± standard deviation or number (%). The p values of comparison between dementia and control group was analyzed by the Mann-Whiney U test. The p values of comparison 3 dementia sub-groups (by CDR) was analyzed by the Kruskal-Wallis test and the Mann-Whitney U test with the Bonferroni correction.
CDR, Clinical Dementia Rating; MMSE, Mini-Mental State Examination; IOPI, Iowa Oral Performance Instrument; sEMG, surface electromyography.
![]()
DISCUSSION
We investigated the changes of strength of tongue lip and pharyngeal muscles for revealing the changes in oral phase dysfunction in patients with dementia and dysphagia. Our results demonstrated that the strength for tongue and lip by IOPI were significantly reduced in patients with dementia. And, the values for sEMG of suprahyoid muscles was not significantly changed. However, analysis of sub-groups by CDR did not reveal significant differences for the strength of tongue, lip and suprahyoid muscles. In summary, the strength of tongue and lip were decreased rather than pharyngeal muscles in dysphagia with dementia based on our results. These findings are consistent with previous researches for dysphagia with dementia, which showed motor dysfunction of a rostral movement of the tongue, difficulty in bolus formation and mastication [67811].
Dysphagia occurs in the early stage of all type of dementia, and it may be associated with functional changes in the brain network [22]. In addition, dysphagia of dementia would be progressive [6]. The dysphagia of AD may be related to dysfunction of the network and resulting in disruption of sensory perception, weakness of tongue motion [78]. The dysphagia of VaD might be associated with disruption of the corticobulbar tract and resulting in difficulty with bolus formation and mastication [723]. The swallowing function in patients with dementia were reported by the higher incidence of clinical or subclinical dysphagia [67]. Our results did not uncover the difference in oral phase function between AD and VaD. However, our findings revealed the decrements of strength for tongue and lip in patients with dementia and dysphagia, was supportive of our previous hypothesis, which the oral phase dysfunction rather than pharyngeal dysfunction would be the causative mechanism of dysphagia in patients with dementia.
The previous research showed the reduction of tongue driving force in even normal elderly [35]. In addition, the post-swallowing remnants can be caused by reduced tongue driving force in healthy elderly [3]. However, most elderly did not recognize their dysphagia despite of increasing oral and pharyngeal residue [24]. Swallowing function in elderly was known as physiologic decrement; reduced tongue driving force, pharyngeal shortening, and impairment of pharyngeal constriction [345]. Another study showed the oral health status and oral sensorimotor alterations are associated with a higher prevalence of oropharyngeal dysphagia in elderly [25]. In addition, the age of control was younger than dementia group. Our control groups were recruited previously for setting the reference of our clinic, not recruited for control of this study. Our control consisted of a usual old healthy volunteer, not age-matched control. Thus, we cannot rule out the just age factor rather than dementia. Our results showed the strength of the tongue and lip more decreased in dementia than normal elderly. Taking together, the dysfunction in the oral phase may usually occur in normal elderly, will become worse in patients with dementia.
The present study was limited by its small sample size (n = 30), and it is not possible to generalize the weakness of tongue was a key of dysphagia in dementia. However, the oromotor facilitation and strengthening tongue based on our results may be important therapeutic strategies for dysphagia in dementia. The second limitation was the age difference between dementia and control, previously mentioned. Thus, additional large-scale, prospective trials with age-matched control would be necessary to address any remaining questions regarding the pathophysiology of dysphagia in dementia or the limitations of ours.
In conclusion, the strength of tongue and lip were decreased rather than pharyngeal muscles in dysphagia with dementia. These findings are supportive for rehabilitation of oral phase function would be necessary for treatment of dysphagia with dementia. These findings would be useful for making therapeutic strategies for dysphagia in dementia.
 XML Download
XML Download