

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cerebral palsy (CP) is currently the most common neurodevelopmental disorder, causing disability and chronic functional impairment worldwide. This disorder results from injury to the brain during the fetal period or early childhood, leading to persistent abnormal muscle tone, motor skills, and cognitive impairment [1].
CP is diagnosed through neurological examination based on a stable course and the absence of an underlying genetic disorder. Diagnostic and interventional strategies in children with CP are largely empirical. Although there is broad agreement on the definition of CP, attempts to classify and measure the severity of motor impairment in children with CP have been less successful [1]. Additionally, conventional magnetic resonance imaging may provide information regarding underlying brain pathology of CP, but anatomical imaging has limited value in quantifying motor deficits [2]. Deficits of motor skills in children with CP are associated with functional abnormalities of motor circuits within the central nervous system. Therefore, the evaluation of motor function in CP patients is indispensable.
Transcranial brain stimulation delivered using several forms of noninvasive electrical cortical stimulation is actively used as an investigation method to probe the pathophysiology of child neurology [3]. Over the past few decades, various studies have proven how transcranial magnetic stimulation (TMS) shows promise for the diagnosis of neurological disorder in children through the application of stimulation to the primary motor cortex as a means to monitor changes in corticospinal excitability [45]. TMS utilizes electromagnetic induction as a highly effective non-invasive method to generate a suprathreshold current in the brain for evaluation of corticospinal tract function by eliciting motor evoked potentials (MEPs) in contralateral limb muscles [3]. In addition, evidence has indicated that MEPs are a valuable indicator for corticospinal excitability at the time of stimulation, and the amplitude of MEPs can be compared at different moments between different states [67].
Spastic hemiplegic CP is the most common type of CP encountered in a clinical setting. A recent study reported that TMS provides objective measurements of the severity of motor impairments which can be used for making inferences from which to classify pathology type in children with CP [8]. Friel et al. [9] used single-pulse TMS to evaluate topography and excitability of motor cortex mapping after bimaual skilled training, and Weinstein et al. [10] and Eng et al. [11] reported that the TMS could reveal bilateral connectivity of corticospinal tract projection and its interhemispheric interaction. However, the differences of each parameter through age and side of hemispheres, especially in contralateral MEPs, have not been studied.
The aim of this study was to investigate the parameters of MEPs in order to evaluate corticospinal tract function in children with spastic hemiplegic CP.
MATERIALS AND METHODS
Subjects
For this study, we enrolled 32 patients with spastic hemiplegic CP [6]. For all children younger than age 6, we fully informed their parents of the study protocol, and they gave their written consent before the evaluation. The study was approved by the Institutional Review Board (IRB) for clinical studies (Chonbuk National University Hospital IRB protocol 2012-12-012).
This study consisted of 17 male and 15 female patients whose average age was 7.5 ± 4.6 years (mean ± standard deviation [SD], range: 2–17 years). We defined the affected hemisphere as the side contralateral to the hemiplegic side and the unaffected hemisphere as the hemisphere on the hemiplegic side. The right hemisphere was affected in 15 patients and the left hemisphere was affected in the remaining 17 (Table 1). Exclusion criteria were as follows: 1) bilateral cerebral lesions, 2) high risk of seizures, 3) poor cooperation during MEP studies, and 4) presence of an indwelling metal or incompatible medical device. Ten patients had congenital malformations, 5 had periventricular white matter lesions, 16 had cortico-subcortical infarction, and according to Krägeloh-Mann's classification, 1 patient was categorized as other [7]. Assessments of hand function using bimanual fine motor function (BFMF) showed that 10 patients had grade I functioning; 8 had grade IIa, 9 had grade IIb, 5 had grade IIIb, and none had grades IIIa or IVb. Based on previous studies, we classified the patients into 1 of 3 age groups; younger than 5 years, 6–12 years, or older than 13 years [121314].
Methods
We used the Medtronic Keypoint® (Medtronic Inc., Skovlunde, Denmark) TMS with a 70 mm figure-of-8 shaped coil to stimulate the cortex at the right and left optimal stimulus areas. The sensitivity was adjusted to range from 50 μV to 1 mV per division. The sweep speed was 50 ms, and filters were applied at 2–2,000 Hz. Patients were evaluated in a relaxed supine position, accompanied by their parents. Using a bipolar configuration, electrodes were placed on the first dorsal interossei (FDI), biceps brachii (BB), and deltoid (DEL) muscles of each arm. The active electrodes were placed on the belly of each muscle with at least a 1 cm inter-electrode distance with the reference was placed on the sternum. The coil was held tangentially to the scalp, with the handle angled backwards and 45° away from the midline. The minimal time interval between stimuli was 10 seconds and the coil temperature was kept < 35°. Initially, we searched for the motor hotspot, which was the point where TMS produced the largest MEP, using a fitting cap pre-marked with sites at 1 cm spacing in the latitude-longitude coordinate system to navigate. Then, we measured the resting motor threshold (RMT), which was defined as the minimum stimulation intensity required to evoke an amplitude of > 50 μV in at least 5/10 consecutive trials. We identified the RMT using incremental 5% increases in stimulation intensity starting at 30% stimulator output. We calculated the onset latency and peak-to-peak amplitude by averaging the values from 4 stimuli at 110% of RMT. To evaluate the central motor conduction time (CMCT), we stimulated the cervical spine (over C5–6) with a 140 mm diameter round coil whilst recording from the FDI. Stimulation intensity was defined using the supramaximal method. CMCT was defined as the difference in latency to the FDI between motor cortical and cervical spinal cord stimulation.
Statistics
We used SPSS version 18.0 for Windows (SPSS Inc., Chicago, IL, USA) for statistical analyses. The χ2 test was chosen to compare the frequency of MEPs elicited in each upper extremity muscle, hemisphere, and different age group. Wilcoxon signed-rank test was used to determine differences between groups in the latency, amplitude, CMCT, and the frequency at which MEPs were evoked for each muscle. Statistical significance was set at p < 0.05.
RESULTS
Frequency of obtaining MEPs in children with spastic hemiplegic CP
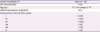
Contralateral MEPs were evoked more frequently in older children than younger children in all muscles examined. In the affected hemisphere, MEPs were evoked more frequently in FDI and DEL in children aged 13 and older compared to children aged 6 to 12 years (p values: 0.036 in FDI and 0.019 in DEL). However, in the unaffected hemisphere, MEPs were evoked more frequently in FDI and BB in children aged 6 to 12 years than children aged 1 to 5 years (p values: 0.003 in FDI and 0.001 in BB). In comparison to the unaffected hemisphere, MEPs were evoked significantly less frequently in the affected hemisphere in FDI and BB in children age 6–12 years (p values: 0.002 in FDI and 0.027 in BB) (Table 2).
Table 2
Frequency of MEP recordings by age in children with spastic hemiplegic cerebral palsy
Data are shown as number (%).
MEP, motor evoked potential; AHS, affected hemisphere stimulation; UHS, unaffected hemisphere stimulation; FDI, first dorsal interossei; BB, biceps brachii; DEL, deltoid.
*The p < 0.05 between 1–5 years and 6–12 years; †p < 0.05 between 6–12 years and ≥ 13 years.
![]()
Latency, amplitude, and CMCT of MEPs in children with spastic hemiplegic CP
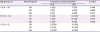
MEP onset latencies showed no significant differences between any of the age groups for any muscle recorded. MEPs evoked from the affected hemisphere showed slightly longer onset latency than those in the unaffected hemisphere, but the difference was not statistically significant difference (Table 3).
Table 3
Onset latencies of motor evoked potentials by age in children with spastic hemiplegic cerebral palsy
Data are shown as mean ± standard deviation.
AHS, affected hemisphere stimulation; UHS, unaffected hemisphere stimulation; FDI, first dorsal interossei; BB, biceps brachii; DEL, deltoid.
![]()
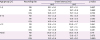
The CMCT in patients with spastic hemiplegic CP was longer when evoked from their affected hemispheres (mean ± SD: 10.4 ± 2.0 ms) than their unaffected sides (9.3 ± 3.0 ms) in all age groups. Children over 13 years old showed a shorter CMCT in both the affected and unaffected hemispheres than children younger than this (Table 4). However, there were no significant differences in these CMCT findings.
Table 4
CMCTs in children with spastic hemiplegic cerebral palsy

| Age group (yr) | Recording site | CMCT (ms) | p value | |
|---|---|---|---|---|
| AHS | UHS | |||
| ≤ 12 | FDI | 10.4 ± 2.2 | 9.5 ± 3.4 | 0.604 |
| ≥ 13 | FDI | 10.5 ± 1.8 | 8.7 ± 0.4 | 0.792 |
| Total | FDI | 10.4 ± 2.0 | 9.3 ± 3.0 | 0.563 |
Data are shown as mean ± standard deviation.
CMCT, central motor conduction time; AHS, affected hemisphere stimulation; UHS, unaffected hemisphere stimulation; FDI, first dorsal interossei.
![]()
MEP amplitude from affected hemispheres was lower than from the unaffected sides in all age groups. However, there were no statistically significant differences in MEP amplitude between different sides. MEP amplitudes were higher in FDI than in DEL and BB, which are located more proximally (Table 5).
Table 5
Amplitudes of MEPs by age in children with spastic hemiplegic cerebral palsy
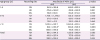
Data are shown as mean ± standard deviation.
MEP, motor evoked potential; AHS, affected hemisphere stimulation; UHS, unaffected hemisphere stimulation; FDI, first dorsal interossei; BB, biceps brachii; DEL, deltoid.
*The p < 0.05 between 6–12 years and ≥ 13 years.
![]()
DISCUSSION
We have demonstrated in previous studies that MEPs could be an efficient tool for investigating motor development in healthy children aged 13 months [15]. In this study, we further investigated contralateral MEPs in children with spastic hemiplegic CP, which has been rarely reported. We obtained MEPs from the proximal upper extremity muscles BB and DEL less frequently than we did from the distal FDI, although these differences varied depending on the children's age. We observed contralateral MEPs in the FDI evoked from the unaffected hemisphere beginning at 30 months, and in children > 5 years old, the frequency of obtaining MEPs from the FDI was 100%. We obtained MEPs from BB and DEL in all children aged 13 and older. These findings suggest that the motor systems innervating proximal muscles have delayed maturation compared with those of distal muscles. However, this result could also be due to technical difficulties in the accurate determination of the hot spot for proximal and distal muscles in children, which is due to their small brain volume and therefore smaller representations within the motor homunculus. In the unaffected hemispheres of children with spastic hemiplegic CP, maturation of the corticospinal tract tends to be similar to that in healthy children, but the results require several considerations that mentioned below [15].
Our results showed a positive correlation between the frequency of MEPs and age in both the unaffected and affected hemispheres in children with spastic hemiplegic CP. Weinstein et al. [10] demonstrated that the use of TMS and brain imaging modalities in children with unilateral motor impairment can be useful for understanding brain-reorganization. In healthy children, the lower frequency of MEPs at the proximal muscle is correlated with the late maturation of the corticospinal tract to proximal muscles or a higher cortical excitatory threshold caused by lower excitability, compared to the distal muscle [15]. Also, the frequency of MEPs in proximal muscles, such as BB, DEL, in more than 5 years aged group increased, because the corticospinal tract maturation and myelination in the upper extremity proximal muscles with aging. Garvey and Mall [12] reported that RMT in children decreased with age, and Koh and Eyre [14] observed MEPs in children > 6 years old.
In the affected hemispheres, we obtained MEPs less frequently than in the unaffected hemispheres. Traversa et al. [16] showed similar patterns in stroke patients where the frequency was also reduced on the affected side. The age-related increase in the frequency of obtaining MEPs in affected hemispheres might reflect progressive recovery of the corticospinal tract and reorganization in children with spastic hemiplegic CP. Therefore, observing MEPs in these patient groups could give us useful information about neuroplasticity, and could play useful roles in the follow-up examinations of these children. In addition to the affected hemisphere, the frequency of the unaffected hemisphere in obtaining MEPs increased in more distal muscle, such as FDI, and the older group, which was consistent with the previous healthy children group study [15]. However, the results of the unaffected hemisphere in the current study, especially 1–5 years group, were lesser evoked, compared to healthy children [15]. Rich et al. [17] stressed the importance of the less-affected hand function and interhemispheric inhibition (IHI) in patients with hemiparetic unilateral CP through the comparison with children with typical development, although the motor threshold in TMS were not significantly differ among the less-affected hand and dominant and non-dominant hand in healthy children. The IHI occurred after age 5 years via connectivity of corpus callosum, so the disappearance of difference between the unaffected hemisphere and healthy children after 6 years group might be associated with the additional neuroplasticity in unaffected hemisphere though IHI.
Pennisi et al. [18] reported the CMCT in stroke patients after the acute phase could be normal, and in this study, onset latency and CMCT in both affected and unaffected hemispheres showed no statistically significant differences. We found that CMCT in children aged 13 years and older was shorter than in children aged 1–12 years, though this was not statistically significant. This is in agreements with the findings of Nezu et al., [19] who showed that by age 13, children's MEPs were similar to those of adults. The differences in children with CP were smaller than those same differences in healthy children [15]. This finding implies delayed maturation of the corticospinal tract in children with spastic hemiplegic CP, and could reflect factors such as an increase in and growth or the reorganization of descending motor pathways. In the unaffected hemisphere, the CMCT showed less than 1 ms differences, comparing to the healthy children [15].
The relationship between onset latency and age has been controversial. Claus [20] reported that the onset latency in upper extremity muscles did not correlate with age. However, Chu [21] and Katz et al. [22] stated that onset latency correlated with subjects' height, which increased with age, and Koh and Eyre [14] stated that as children aged, latency decreased. In our study, there were no statistically significant differences between onset latency and age in children with spastic hemiplegic CP. This result might have been caused by the late maturation of the corticospinal tract in these children. It could also have been influenced by increasing nerve conduction velocity given that synapse growth and decreasing nerve conduction time are associated with an increase in height as children with CP grow taller. Clarifying the correlations between maturation of descending motor pathways, latency, and CMCT through sequential MEP studies in children with spastic CP is an ongoing task. Regarding the mean onset latency of the unaffected hemisphere in patients with hemiplegic CP showed more delayed results of BB and DEL, particularly in 1–5 year group (BB 16.7/13.0 and DEL 15.7/12.9 ms), compared to the healthy group [15].
Traversa et al. [16] reported that amplitudes of MEPs evoked in the affected hemispheres of acute-phase stroke patients were lower than those from unaffected sides, and in the subacute and chronic phases, the amplitudes on the affected sides increased as the patients recovered. In this study of children with spastic hemiplegic CP, MEP amplitudes in the affected hemispheres were lower than those on the unaffected sides. These findings might correspond with brain damage recovery patterns of the immature corticospinal tracts in spastic hemiplegic CP patients and in the mature motor systems of adult stroke patients. Additionally, Eng et al. [11] reported that the interhemispheric ratio, which calculated mean conditioned MEP amplitude/mean test MEP amplitude, in prenatal stroke patients at baseline were increased in both affected-to-unaffected and unaffected-to-affected hemisphere, compared to healthy subjects [23]. In our study, the mean amplitude of tested MEP in both unaffected hemisphere and healthy children showed similar values and tendency that increase following the older group and more distal muscle.
Carnahan et al. [23] suggested that gross motor function and manual ability were frequently discrepant in children with CP [24]. Hand function is closely correlated with cognitive ability and voluntary motor control, and children with unilateral impairment will sometimes not use the affected arm, leading to a lack of bimanual function [24]. In our study, there were no significant differences in the frequency, CMCT, onset latency, or amplitudes of MEPs between the different BFMF grading groups. These findings suggest that MEP studies in children with spastic hemiplegic CP could potentially provide further information related to gross motor function as well as additional components of their functional status including cognitive ability, voluntary motor control, and recognition and use of their affected arm.
However, there are study limitations that we require further investigation. First, the small number of patients was participated. Secondly, we limitedly collected the data of the patients' motor threshold and other functional or activity of daily living scales, including the Assisting Hand Assessment, the Melbourne Assessment of Unilateral Upper Limb Function, the Jebsen-Taylor Test of Hand Function, the Gross Motor Function Measure, Functional Independence Measure for Children, and Manual Ability Classification System (MACS). Lastly, we analyzed contralateral MEPs only, but ipsilateral MEPs from unaffected hemisphere in patients with hemiplegic spastic CP are common and correlated with poorer motor function [11]. However, Eng et al. [11] reported that the contralateral motor network in patients with unilateral CP played a significant role in functional abilities, which were not limited by those in ipsilateral side.
In conclusion, we conducted this study to reveal the maturation of the corticospinal pathways to upper extremity muscles and identify reorganization patterns in children with spastic hemiplegic CP using TMS. In the present study, there were difference in MEP presence and parameters according to the recorded muscles and children's age. Therefore, analyzing MEPs in these patients might reflect the development and reorganization of descending motor pathways and could serve as a useful tool for follow-up examinations in children with spastic hemiplegic CP.
 XML Download
XML Download