

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
The clivus is a bony surface, the name of which means “slope.” The fusion of the basisphenoidal and basiocciput bones results in the middle portion of the skull base. This fusion usually takes place before the age of 18 years.12 Fossa navicularis is an anatomical variation of the bone in the lower part of the clivus, as well as a notch in the basiocciput bone. This variation has also been referred to as fossa pharyngea, large pharyngeal fossa, keyhole defect, longitudinal or transverse segmentations, fossa navicularis magna, and canalis basilaris medianus. Generally, fossa navicularis is an incidental finding in radiological examinations and has clearly visible cortical margins.3
Since cone-beam computed tomography (CBCT) has a lower radiation dose and higher resolution than conventional computed tomography (CT) scans, its usage has become more common in recent years. CBCT can provide a 3-dimensional morphological evaluation of dental and maxillofacial anatomy.4 Therefore, due to its widespread use, increasing interest is emerging in the anatomical features and anatomical variations of the human skull.
Dentomaxillofacial radiologists must be familiar with all the craniofacial structures and anatomical variations in the imaging field. Therefore, the anatomical variation of the fossa navicularis within the clivus must be identified and reported. In the literature, there are limited studies evaluating the prevalence and morphometric properties of the fossa navicularis.1235 In this context, the aim of this study was to determine the prevalence and morphometric properties of fossa navicularis within the clivus in a Turkish subpopulation using CBCT.
Materials and Methods
A total of 168 patients (71 males, 96 females) who were admitted to the Faculty of Dentistry of Necmettin Erbakan University, Konya, Turkey between June 2016 and May 2017 and received CBCT scans for the purpose of diagnosis and treatment were included in this study. The Necmettin Erbakan University Research and Ethics Committee approved this retrospective study (decision no. 2019/05). High-quality CBCT images of patients without a syndromic condition or a history of neurological disease or surgery were included in the study.
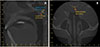
CBCT images were obtained using a Morita 3D Accuitomo 170 device (J Morita MFG Corp., Kyoto, Japan) according to the manufacturer's recommended protocol, using 90 kVp and 5 mA, a rotation time of 17.5 seconds, a voxel size of 0.25 mm, and a 140-×100-mm field of view. A total of 168 CBCT images were analyzed using i-Dixel software (J Morita Manufacturing Corp., Kyoto, Japan) by the same oral and maxillofacial radiologist. The contrast and brightness of the images were adjusted using the software's image processing tool to ensure optimum viewing. Axial and sagittal images at different levels were visualized on the monitor. Fossa navicularis was detected in the sagittal plane on the anterior side of the clivus. The depth and length of the fossa navicularis were measured from the deepest part in the sagittal plane (Fig. 1A). The width of the fossa navicularis was then measured on the axial plane in the same cross-section as the software's router (Fig. 1B). All measurements were repeated twice, with 3 weeks between each measurement by the same observer.
Statistical analysis was performed using IBM SPSS® version 21.0 (IBM Corp., Armonk, NY, USA). The descriptive statistical values were given. The normality of the data distribution was assessed by the Kolmogorov-Smirnov test. The measurements were statistically compared by sex using the Mann-Whitney U test. Correlations between age and measurements were evaluated using the Spearman correlation test. Intraobserver agreement was evaluated using the intraclass correlation coefficient, with results between 0.86 and 0.91. Statistical significance was set at P<0.05.
Results
Fossa navicularis was identified in 46 (27.5%) patients. Among these patients, 22 were female (22.9% of all female patients), whereas 24 were male (33.8% of all male patients). The mean age of patients with fossa navicularis was 31.8±16.4 years (range, 18–80 years).
The mean length, depth, and width of the fossa navicularis in the 46 patients in whom it was present were 8.55 mm, 2.22 mm, and 5.37 mm, respectively (Table 1). Sex was not significantly related with the depth, length, and width of the fossa navicularis (P>0.05). A significant positive correlation was found between age and length of the fossa navicularis (P=0.005; rho=0.408).
Discussion
In the present study, the prevalence and morphometric properties of fossa navicularis within the clivus were evaluated in a Turkish population using CBCT. Our study showed that the prevalence of fossa navicularis was 27.5%. The mean length, width, and depth of the fossa navicularis in the 46 patients with fossa navicularis were 8.55 mm, 5.37 mm, and 2.22 mm, respectively.
Fossa navicularis is very important because it is close to various anatomical structures, such as the nasopharynx and sphenoid sinus. Various pathological lesions, such as local or metastatic tumors, adenoid retention cyst, adenoid hypertrophy, Rathke pouch cyst, and dermoid teratoma of the posterior nasopharyngeal wall, may mimic its anatomy or vice versa.678 For this reason, it is important to know this anatomical variation in detail.
In some studies, it was stated that fossa navicularis was the route through which an infection of the oropharynx spread to the skull. Surgical obliteration of this defect resulted in complete recovery.91011 Therefore, understanding the anatomy of embryology and bone variations may help to diagnose conditions affecting this region.3
In the literature, fossa navicularis has generally been analyzed in dry skulls or CT images.121314 There are a limited number of studies using CBCT.13 Therefore, we preferred to use CBCT images in this study. The prevalence of fossa navicularis was found to be between 0.9% and 5.3% in studies using dry skull. In the study of Cankal et al.,13 it was found to be 3% in CT images. Ersan3 and Bayrak et al.1 also evaluated fossa navicularis on CBCT images in the same population. Ersan3 reported the prevalence of fossa navicularis to be 6.6% in 732 patients. Bayrak et al.1 studied 1,059 patients, and found the prevalence to be 7.6%. In this study, the prevalence of fossa navicularis was 27.5%. This result is markedly higher than other studies in the literature. This discrepancy might be due to different methodologies, ethnic differences, and different sample sizes. In a recent study conducted by Ersan,5 it was reported that the prevalence of fossa navicularis was 28.8% in cleft palate patients, similar to our result.
In this study, the mean length, width, and depth of the fossa navicularis in 46 patients were 8.55 mm, 5.37 mm, and 2.22 mm, respectively. In the literature, it has been reported that the length varies from 7 to 13 mm, the width from 6 to 8 mm, and the depth from 2 to 5 mm.15 Bayrak et al.1 reported a length of 7.15 mm, width of 5.23 mm, and depth of 2.76 mm in CBCT measurements of 59 patients with fossa navicularis. In addition, they also studied CT scans and found that the length, width, and depth of the fossa navicularis in 22 patients were 4.12 mm, 4.08 mm, and 4.17 mm, respectively.
Ersan3 reported no difference in the length of the fossa navicularis between age groups, while Bayrak et al.1 stated that there was a statistically significant difference between age groups in terms of the length of the fossa navicularis. In this study, a significant positive correlation was found between age and the length of the fossa navicularis (P=0.005; rho=0.408). There was an increase in the size of the fossa navicularis as age progressed.
In the literature, it has been reported that infections are carried through caudocranial structures via the fossa navicularis.101116 Therefore, it is important to know this anatomical variation in detail. Insufficient studies have been conducted on this area in the field of dentomaxillofacial radiology. Therefore, it is necessary to increase the number of studies of such anatomical variations, in particular by conducting studies with larger samples and in more ethnically diverse populations.
In conclusion, the prevalence of fossa navicularis in this study was higher than reported in the literature. However, it was still an uncommon variation. The anatomical structures of the fossa navicularis can be studied effectively on CBCT images. Because CBCT findings include areas at the base of the skull, which are not intended to be displayed, dentomaxillofacial radiologists have an obligation to identify, examine, and report anatomical variations of the skull base and to prevent unnecessary requests for further imaging by dental practitioners. The findings of this study may be useful for radiologists, anatomists, and surgeons interested in the base of the skull.

 XML Download
XML Download