

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Since the discovery of the X-ray, dental radiology has played a vital role as an important diagnostic adjunct to the clinical assessment of dental patients, treatment planning, and prognostic evaluation of dental diseases.1 Intraoral and conventional radiographic procedures suffer from the limitations of 2-dimensional (2D) projections, which include magnification, distortion, superimposition, and misrepresentation of structures.1 Cone-beam computed tomography (CBCT) presents as a separate C-arm to conventional computed tomography (CT) and it has gained broad acceptance in dentistry in the last 5 years as it generates 3-dimensional (3D) data at lower radiation dose and cost and a higher spatial resolution than conventional CT.2
CBCT has revolutionized the imaging of the maxillofacial region due to its wide range of applications across the fields of dentistry, ranging from diagnosis to treatment planning. However, a lack of proper education and awareness among dentists is leading to unnecessary referrals for CBCT imaging. Early CBCT machines used image intensifiers with large fields of view (FOVs), thus exposing patients to higher doses of radiation, although these doses were still less than those associated with medical CT. Recently, advances in software have enabled the optimization of CBCT scanners via improvements that reduce the radiation dose, such as the incorporation of a small FOV, pulsed radiation exposure, and collimation. In addition, CBCT exposure should be clinically justified for each patient based on the principle of keeping radiation dose “as low as reasonably achievable (ALARA),” which is supported by the American Dental Association.3 CBCT should not be considered a replacement of panoramic or conventional projection radiographic applications, but rather a complementary modality used for specific applications.4 This review aims to emphasize the broad nature of CBCT usage in maxillofacial imaging. Additionally, it aims to discuss the non-dental applications of CBCT, the recently-introduced possibility for enhancement of CBCT using artificial intelligence or machine-based learning, and the combination of CBCT with optical imaging to facilitate the better diagnosis and treatment of complex dental pathologies. In addition, this review also focuses on optimization of CBCT with the goal of reconstructing each image at a low exposure rate. Table 1 details the clinical applications of CBCT in dental practice, while Table 2 summarizes studies from the existing literature that highlight the application of this emerging 3D imaging modality in dentistry.567891011121314
Applications of CBCT in dentistry
Endodontics
Intraoral radiography is the preferred imaging method for the evaluation of endodontically treated teeth. Recently, however, CBCT has proven to be a promising diagnostic aid for complex endodontic cases, including the detection and visualization of extra canals, lateral canals, perforations, obturations, canal shape, and vertical root fractures. 1516171820 High-resolution CBCT images, limited FOV, and small voxel sizes provide dentists better visualization of the full length of the root canal. Kottoor et al.17 used CBCT to detect 7 root canals in the maxillary first molar.
CBCT has superior diagnostic efficacy in the assessment of complex dental pathologies, malformed teeth, caries extension, differentiation of periapical pathologies, external and internal root resorption, and root fractures.181920 Patel21 reported a case of dens invaginatus in which a CBCT scan revealed no communication between the invagination and the main root canal, thus preventing unnecessary root canal treatment of the concerned tooth. Akgül et al.5 used CBCT scans to detect a relatively high frequency of enamel pearls in the maxillary second and third molars. Young et al.22 found that 3DX high-resolution CBCT images displayed better detection of proximal surface caries extension than digital intraoral 2D images. Root fracture is the most common cause of root canal failure that cannot be seen in conventional periapical radiographs due to the superimposition of anatomical structures. Conventional CT may detect around 70% of root fractures, but the higher cost and larger amount of radiation exposure limit the use of this technology by oral radiologists. For this reason, CBCT is currently thought to be superior to CT in diagnosing root fractures, visualizing external and internal root resorption, and visualizing the repair of resorptive defects accurately and with higher resolution.232425
Periodontics
CBCT is a more reliable and reproducible method of assessing incipient furcation involvement, buccal and lingual periodontal bone defects, and the extent of intrabony defects than 2D radiography. Volume rendering by CBCT can facilitate the assessment of preoperative alveolar bone volume and the postoperative adequacy of bone fill. Moreover, CBCT enables an accurate assessment of the outcome of regenerative periodontal therapy and bone grafts.262728 It has been suggested that, although CBCT has significant diagnostic applications in periodontics, conventional radiography can better depict bone quality, periodontal ligament space, and bone levels; accordingly, the decision to use CBCT imaging should only be made after careful consideration of its potential risks and benefits. In addition, differences in imaging protocol parameters can affect the reproducibility and reliability of CBCT used for the measurement of alveolar bone height and thickness.2829 Peterson et al.29 concluded that CBCT underestimated alveolar bone height; mean facial bone height on CBCT images ranged from 0.33±0.78 mm to 0.88±1.14 mm, which was less than the absolute bone height of 0.56±0.35 mm to 1.08±0.92 mm.
In the detection of fenestrations and dehiscence, the efficacy of CBCT was found to be poorer than that of conventional 2D radiography, although CBCT provided better image quality. It has been suggested that the lower accuracy of CBCT may be due to the presence of teeth, metallic dental fillings, or other beam-hardening artifacts. Full-scan CBCT (360°) with a 0.2-mm voxel size using a small FOV is more effective in the detection of both fenestrations and dehiscence, especially in peri-implant cases. Peterson et al.29 found that CBCT overestimated the presence of dehiscence and fenestration defects, and inter-examiner reliability ranged from poor to moderate (Cohen's kappa= − 0.09 to 0.66). In another study, Xu et al.30 found limited diagnostic value of CBCT in clinical practice, as the technique overestimated the presence of dehiscence and fenestrations in the maxillary anterior teeth of patients with Angle class III malocclusion; however, the level of agreement between clinical examination and CBCT imaging was higher for dehiscence than fenestration. Contrary to this observation, Leung et al.31 found a higher rate of diagnostic accuracy for the detection of root fenestrations than for the detection of dehiscence.
Mandibular canal assessment
Accurate assessment of the variation and position of the inferior alveolar canal relative to the mandibular third molar roots may reduce the risk of injury to the nerve during extraction and implant placement, thus preventing further complications.3233 Panoramic imaging may be adequate when the canal is relatively distant from the third molar, but in the case of radiographic superimposition, use of a 3D imaging approach is preferable. Lee et al.34 reported 4 cases and Villaco-Carvalho et al.6 reported 80 cases of bifid mandibular canal visualized using CBCT imaging. Lofthag-Hansen et al.35 suggested that the visibility of the mandibular canal and the marginal crest, as well as the level of observer agreement regarding the location of these structures, is higher with CBCT.
Implantology
CBCT provides cross-sectional images in several planes that help with the accurate assessment of the height, width, and angulation of bone, as well as with visualization of the position of the inferior alveolar canal and mental foramen in the mandible and the sinus in the maxilla. In edentulous patients, CBCT provides better visualization of buccolingual alveolar ridge patterns, such as irregular, narrow crestal, or knife-edge ridge, undulating concavities, and alveolar bone quality and quantity. In many situations, CBCT implantology has minimized or eliminated the need for procedures like bone and tissue grafts, as it enables precise measurement of the distance, area, and volume of the bone in which the implant is to be placed.3637 Computer-generated surgical guides (termed stereolithographic models) can be generated using Digital Imaging and Communications in Medicine data, thus eliminating the possible inaccuracy involved in making traditional guide stents. The use of software planning prior to implant placement helps surgeons position the implants more accurately and safely. Using this technology, minimally invasive surgery can be performed without raising a flap, thereby minimizing surgery time, postoperative pain and swelling, and recovery time. The stored information from the scan can be used pre-surgically to fabricate a master cast, and provisional restoration could be placed immediately after surgery (Teeth-in-an-Hour™; Nobel Biocare, Kloten, Switzerland).7363738
Studies have suggested that assessment of the course of the vascular canals in the maxillary sinus walls, as well as the distance between the sinus floor, the edentulous alveolar crest, and the vascular canal using CBCT, can prevent unnecessary bleeding during implant placement. This technique accurately measures the thickness of the hard palate and its overlying mucosa for the purpose of miniscrew placement.3940 However, the American Academy of Radiologists (AAOR) has recommended panoramic radiography as the primary imaging modality for the initial assessment of the implant site. Cross-sectional CBCT images should be considered only when clinical conditions require sinus augmentation procedures or bone grafting, or if the patient reports implant mobility post-surgery.39
Periapical and bony pathologies
The literature confirms that CBCT has higher diagnostic accuracy for the visualization of periapical lesions and their differentiation from other similar-appearing lesions.41 In clinical practice, radiological evaluation of periapical status is essential for both establishment of a treatment plan and better prognosis of the tooth. Intraoral periapical radiographs are routinely used in endodontics, but they present some limitations, such as the 2D nature of the produced images, geometric compression, and superimposition of anatomical structures, thus obscuring the area of interest; these limitations may lead to misdiagnosis or unnecessary exposure to radiation.842 New CBCT scanners that deliver a lower radiation dose have become an important diagnostic tool to address most endodontic problems, and these devices can be used in all phases of endodontic treatment. CBCT imaging is highly useful in the post-treatment assessment of endodontically treated teeth; it is also very helpful for the determination of the cause of a persistent periapical lesion, as well as the visualization of root canal morphology, the localization of accessory canals and calcified canals, the detection of acute root fractures, and the visualization of external and internal resorption.36373839 According to the recommendations put forth by the American Academy of Oral and Maxillofacial Radiology (AAOMR) for endodontic treatment, intraoral radiography should be considered the primary imaging modality, and CBCT should be recommended only if the patient's condition cannot be accurately diagnosed using intraoral 2D radiography or the patient presents with non-specific clinical signs and symptoms associated with untreated or endodontically treated teeth.3536 CBCT defines the extent and internal structure of large intraosseous pathologies such as cysts and tumors more precisely than intraoral radiography and also effectively analyzes the proximity of these lesions to vital structures.9 Thus, CBCT images can serve as a useful guide for surgeons as they carry out appropriate early surgical interventions, especially in the treatment of oral malignancies.43
Maxillofacial fractures
Evaluation of a fracture – especially in the maxillary complex region – using conventional 2D radiography is very challenging due to the overlapping of various structures. Additionally, radiographic evaluation of patients with maxillofacial injuries can be very difficult due to their clinical condition and the fact that these patients are often uncooperative. Instead, 3D CBCT is a cost- and dose-effective alternative to conventional 2D imaging for the diagnosis of complex maxillary fractures.44 It provides the surgeon with 3D-reconstructed images for analysis of the nature of the injury, the location of the fracture, and the degree of displacement of the fractured segments. These images guide the surgeon to plan the appropriate surgical approach for the reduction and stabilization of the fractured segments.45 Mandibular fractures are easily visualized on a panoramic radiograph in most cases; however, some cases require further confirmation by CBCT, including dislocation of fracture fragments in the mandibular corpus and split fractures in which the fracture line is not parallel to the X-ray beam.46 To facilitate better treatment of trauma patients, CBCT should be made mandatory in maxillofacial and suspected mandibular fractures. This technique should be used in conjunction with panoramic radiographs, which are useful for the initial screening of complicated fractures.4546
Temporomandibular joint disorders
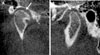
Temporomandibular joint disorders (TMDs) constitute the most common category of orofacial pain conditions of the temporomandibular joint (TMJ) and its associated musculature.47 As of now, CBCT has been found to be most useful in the evaluation of bony changes of the TMJ, such as fractures, ankylosis, dislocation, growth abnormalities, and various degenerative joint diseases including osteophytes, erosions, flattening, subchondral sclerosis, and pseudocysts (Fig. 1). Analysis of the dynamic relationship of the articular sufaces of the TMJ is necessary to determine the strain undergone by the articular disc while chewing; this strain, if high, may compromise the integrity of the disc. CBCT provides 3D images of the mandibular condyle and surrounding structures to facilitate the analysis and diagnosis of bone morphological features, joint space, and the dynamic function, which serve as the critical keys to treatment outcome in patients with signs and symptoms of TMD.104748 Studies have suggested that the diagnostic accuracy of CBCT in the evaluation of erosive changes of the condyle is influenced by FOV, with these studies utilizing FOVs of 12, 9, and 6 inches with voxel sizes of 0.6, 0.3, and 0.2 mm, respectively. It has been reported that a CBCT scanner with high resolution and the smallest FOV (voxel size, 0.2 mm) detected condylar defects with greater than 80% sensitivity.48 Previous studies have shown magnetic resonance imaging (MRI) to be the preferred imaging modatility for evaluation of anterior disc displacement without reduction, but this technique has low accuracy in diagnosing bony changes, which should be further examined using CBCT.47 Recently, automatic registration of CBCT scans with MRI has been developed to provide complementary images of the hard and soft tissues of the TMJ in a single picture frame, facilitating accurate diagnosis and optimal treatment outcomes. Al-Saleh et al.49 found that fused magnetic resonance imaging-cone-beam computed tomography (MRI-CBCT) registered images improved intra- and inter-examiner consistency and displayed better diagnostic value in the evaluation of internal derangement of the TMJ. More clinical research must be conducted to establish the reliability and accuracy of MRI-CBCT registration for TMDs.
Soft tissue assessment
In dentistry, CBCT scanners are exclusively used for imaging of the hard tissues of the oro-facial complex. These scanners have a limited ability to differentiate soft tissues. To address this issue, Januario et al.50 developed soft tissue CBCT that scanned the maxilla using an i-CAT™ scanner (Imaging Sciences International, Hatfield, PA, USA) for 40 seconds with a focal spot of 0.5 mm, voxel size of 0.2 mm, and grayscale 14-bit resolution. This technique improved the image quality of the soft tissue by reconstructing the images in all 3 orthogonal planes (axial, sagittal, and coronal). It allowed precise measurement of the thickness of gingival tissues, and i-CAT™ software was used to determine the relationship of the periodontal structures and dentogingival unit. According to the guidelines set forth by the AAOR, CBCT constitutes a valuable tool for determining the location of soft tissue calcifications by oral and maxillofacial radiology specialists.5152 Soft tissue calcifications are usually asymptomatic and appear incidentally on radiographs. One of the greatest difficulties in the diagnosis of soft tissue calcifications is the determination of their exact location. This is especially challenging when using panoramic radiographs, since 2D imaging techniques can create ghost images.5253 Nunes et al.11 reported that a higher prevalence of soft tissue calcifications was found on CBCT images as compared to conventional images.
Salivary gland pathologies
Imaging-based diagnostic measures for sialolithiasis include ultrasonography, panoramic radiography, sialendoscopy, sialography, MRI, and CT. Although CT and MRI are more advantageous in salivary gland evaluation, ultrasonography and 2D radiography are routinely used due to their cost-effectiveness and availability. Recently, superimposition-free, 3D CBCT images have shown higher sensitivity and specificity for salivary calculus diagnosis, stenosis, and dilatations of the salivary ductal system than images obtained with other diagnostic methods.125455 CBCT sialography is considered a noninvasive diagnostic tool used for the visualization of salivary glands and ductal pathologies. Drage and Brown54 first described the use of CBCT sialography for complex cases of salivary gland obstruction. They proposed that CBCT sialography would expose the patient to higher radiation doses than plain film sialography, and therefore it should be reserved for complicated cases. Jadu et al.55 suggested that the delicate secretory branches of salivary gland ducts and the parenchyma of the salivary glands were more easily detectable on CBCT images via the maximization of the image signal difference-to-noise ratio. They achieved moderate to very good inter-observer agreement in the visualization of normal gland structures and in the determination of abnormal findings (i.e., sialoliths, ductal strictures, and secondary inflammatory changes) by CBCT sialography than plain film sialography.
Orthodontics
Orthodontists routinely use 2D conventional radiographs (such as cephalometric and panoramic radiographs) to diagnose and plan treatment for patients with malocclusions and facial disproportions. However, many complex orthodontic and dentofacial orthopedic problems require 3D analysis. To address this, CBCT has been introduced as a technique for comprehensive orthodontic imaging and for the assessment of tooth movement in all 3 planes.3 Although it has numerous benefits, one major concern regarding CBCT is the higher radiation dose delivered from CBCT scanners with large FOV. Therefore, the decision to conduct CBCT imaging on an orthodontic patient should be solely based on the patient's history and on the clinical examination, where CBCT should only be used if these factors indicate that CBCT is required for proper diagnosis and optimal treatment outcome. Some CBCT scanners have a small FOV, which minimizes radiation exposure; in these scanners, the number of projection images still allows for adequate visualization of the region of interest.5657
CBCT imaging in orthodontics is selectively indicated for the assessment of complex dentoskeletal relationships and facial esthetics, for severe skeletal discrepancies requiring orthognathic surgery, and for the assessment of the position of impacted and supernumerary teeth and their relationships to adjacent roots and other anatomical structures, thus facilitating planning of the subsequent tooth movement.56 Compared to 2D radiographs, CBCT imaging better facilitates the accurate determination of tooth and root length, the assessment of the minute details of root resorption, the determination of available bone width (to evaluate the buccolingual movement of teeth), the assessment of tooth inclination, the calculation of torque, and the visualization of soft tissue relationships, and it provides detailed information regarding craniofacial morphology and maxillary and mandibular changes resulting from rapid maxillary expansion.57
Forensic odontology
Estimation of the ages of living or deceased individuals is an important aspect of forensic investigation. Several techniques to estimate the age of individuals by analyzing teeth have been reported in the literature. One avenue that offers new opportunities in dental age identification is examination of the pulp space. Various methods have been developed to study the size of the pulp chamber, including tooth cross-sections and radiographs; however, CBCT provides a 3D view of the pulpal cavity, facilitating a more accurate estimation of the dental age of an individual. CBCT is a reliable imaging technique for the analysis of secondary dentin apposition with advancing age, and it simultaneously measures both the buccolingual and the mesiodistal dimensions of the tooth.1458 Yang et al.58 developed a custom-made voxel-counting software that can be used to calculate the ratio of pulp canal volume to tooth volume based on CBCT tooth images, and they obtained promising results for non-invasive dental age estimation. CBCT also provides accurate and reliable measurements of soft tissue thickness for specific landmarks of the face and scalp by producing facial reconstruction at reduced exposure and increased speed, and it provides higher-quality images than spiral CT and other methods. Facial reconstruction requires knowledge of the average thickness of the soft tissues of the face, which varies among individuals from different geographical locations. This technique is very useful in forensic investigations for the identification of skeletal remains, and it aims to recreate the facial appearance of an individual using the skull.1359
CBCT is currently used in forensic investigations for postmortem imaging and for imaging high-density metal projectiles in cases of gunshot injury. Its use is mainly due to its small apparatus size, portability, low cost, and the reduction of metal artifacts on the images that it provides. CBCT showed superior results to multidetector CT in the detection of structural hard-tissue damage in the immediate vicinity of high-density metal projectiles and in the identification of the precise location of a projectile in the body.60
Future perspectives
Optimization of CBCT images
Compared with other modalities, CBCT has been documented to have high diagnostic efficacy in the accurate detection of complex oral and maxillofacial pathologies. This efficacy could be increased further by the optimization of CBCT with respect to various parameters, such as reduction in focal spot size, alteration of beam geometry, an increase in detector efficiency, and optimization of exposure and image reconstruction. Moreover, old CBCT scanners mostly have large FOV that results in the production of more scattered radiation, which contributes to an increased radiation dose delivered to the patient. Optimization of old scanners could be achieved by using a small-diameter FOV that covers only the region of interest.61 Table 3 shows the future innovations of CBCT.
Focal spot size was the first parameter of CBCT to be improved; it was decreased from the standard focal spot size of 0.5 mm, thus improving the image resolution. Another important improvement was the development of adaptive exposure, which enables the clinician to select the optimal exposure according to the size of the patient. In most CBCT machines, current and tube voltage is determined based on the gray values of scout images, which results in an automatic reduction of exposure levels for patients of small size and mass. Recently, some machines have utilized the concept of dynamic automatic exposure control, in which exposure is adjusted during acquisition of the image. Image performance could be increased by altering the geometric shape of the beam; this has been achieved by a technique termed off-axis scanning, which utilizes a half cone with a small overlap in the iso-center that increases the FOV to almost twice the diameter as that involved in full-cone scanning. This contributes to a reduction in the dose administered to the patient. It has also been reported that use of 180° rotation in comparison to 360° rotation led to a dose reduction of 40% in the anterior region and 60% in the posterior region. Off-axis scanning reduces the radiation dose, but its effect on image quality is still under study. Optimization could also be obtained by increasing the efficiency of the detector. Because most CBCT units use flat panel detectors consisting of a scintillator that transfers light energy into electrical energy, detector efficiency could be increased by decreasing the detector pixel size. In addition, doing this increases the temporal resolution, resulting in a shorter scan time and an improvement in image reconstruction.161
Several CBCT devices use pulsed exposure, resulting in a large discrepancy between scan time (the time between the first and last projection) and exposure time (the cumulative time over which an exposure is made). In contrast, some machines allow only continuous exposure, for which the total scan time and the exposure time are same. Pulsed X-ray systems have better spatial resolution than systems that rely on continuous exposure, owing to a reduced motion effect due to the movement of the gantry during each exposure in pulsed systems.362
Image reconstruction has been revolutionized by the use of the algebraic reconstruction technique, which requires almost half the number of projection images than that required by the Feldkamp algorithm. The algebraic reconstruction technique is most commonly combined with the metal artifact reduction algorithm, which reduces large amounts of scatter and absorption during the scan. One drawback of the algebraic reconstruction technique is its long computation time, which results in patient motion artifacts that have been reported to have a profound effect on the quality of the CBCT images. Motion artifacts can be corrected by comparing the consecutive projection images and removing those images which are non-diagnostic due to the patient's movement during the scan.60 Other recent software advancements involve artificial intelligence or machine-based learning, particularly the training and programming of machines to read radiographs and to predict the location of pathologies. Hiraiwa et al.63 applied deep-learning artificial intelligence to panoramic images of the mandibular first molar in which CBCT imaging had determined the presence of extra roots in 21.4% of the distal roots imaged. The artificial intelligence system displayed a diagnostic accuracy of 86.9% in the determination of whether the distal root was single or had extra roots. In the very near future, deep learning image analysis tools aim to improve the diagnosis of and treatment plans for periodontal diseases via detection of early bone loss and changes, early intervention of peri-implantitis, and even detection of early-stage oral cancer. Furthermore, to improve reconstruction efficiency, the standard filtered back projection method has been optimized by GPUs. Noel et al.64 found that computation time for 256 volumes was reduced from 25 minutes (using the standard reconstruction algorithm) to 3.2 seconds using GPU reconstruction, and GPU reconstruction time for 512 volumes was 8.5 seconds.
Another recent innovation is real-time dual-energy imaging, in which 2 sets of projections are made at 2 different energies. This allows broadening of the contrast range. Real-time dual-energy imaging has been applied in angiography due to its reduction of the superimposition of bone and blood vessels. Moreover, this technique reduces beam-hardening artifacts and provides energy-selective imaging. Although its application in dentistry still needs to be validated, it has the potential to improve contrast-based imaging, CBCT sialography, and the accurate identification of sialoliths based on their composition.61
Optical scanners with CBCT
Recently, the diagnostic process has been enhanced by the introduction of optical scanners, and combination of these techniques with CBCT could lead to improved treatment planning. Although CBCT can provide cross-sectional 3D images of the maxilla and the mandible for implant surgery, it cannot replicate the surface details and occlusal morphology of teeth. This task is accomplished by placing a stone cast into an optical scanner and then into a CBCT machine with same settings as the patient's scan; alternatively, intraoral scanners could be used to take virtual impressions of the occlusal surfaces of the teeth, thus precluding the use of regular impression materials. These digital technologies allow the clinician to clearly visualize the patient's anatomy when planning minimally invasive surgery.65 Another software advancement has merged optical facial scanning with CBCT, with the aim of evaluating the effect of orthodontic treatment or orthognathic surgery on the facial structures. However, this 3D representation of facial features should be validated by future clinical trials.6265
Non-odontogenic pathologies
While CBCT scans were initially used exclusively for imaging the dentomaxillofacial complex, the use of this technique has expanded to include the visualization of non-tooth-related pathologies and abnormalities in the head and neck region, mainly sinus pathologies, such as mucosal thickening, partial opacification with liquid accumulation, total opacification, and polypoidal mucosal thickening. Low-dose multidetector CT has long been used to image the sinuses, but this technique has several limitations. For instance, the resultant images are usually noisy due to metal artifacts, and they have lower spatial resolution. CBCT images provide complete diagnostic information regarding sinus pathologies with higher spatial resolution than multidetector computed tomography.6166
Tumors of the skull base are better visualized with MRI than with CBCT, but CBCT does play a crucial role in the detection of calcification processes, as well as in situations requiring sinus lifting or bone augmentation procedures. In addition, CBCT is used for 3D analysis of the upper airway dimensions of patients with cleft lip and palate or obstructive sleep apnea. CBCT scanning can also be used to assess swallowing function, particularly in cases when videofluoroscopy is not available. It is now increasingly used by orthopedic surgeons to image the upper and lower extremities, as well as by ENT clinicians to analyze sinus and ear infections at a low dose of radiation.66
Phase contrast tomography
The literature includes numerous studies investigating the X-ray absorption of the object under study in phase contrast tomography, but the phase nature of the X-rays still requires further exploration. Recently, researchers have introduced quantitative phase-contrast cone-beam tomography, in which the phase coefficient rather than the attenuation coefficient is used to reconstruct the image. This technique utilizes unfiltered radiation from a small polychromatic source, thus reducing high spatial frequency noise and contributing to high soft tissue contrast.6167
Discussion
CBCT has proven to be a promising advancement in imaging of the oral and maxillofacial region due to its many advantages compared with conventional CT, including lower cost, smaller radiation dose, and the need for less space. CBCT scanning is associated with a few disadvantages, including poor soft tissue contrast, image noise, and the presence of motion artifacts. However, the potential benefits of CBCT outweigh the risks. Future efforts to improve this technique should most likely be directed towards reducing the scan time; providing multimodal imaging (conventional panoramic and cephalometric, in addition to CBCT imaging); improving image fidelity, including soft tissue contrast; and incorporating task-specific protocols to minimize patient dose (for example, high-resolution, small FOV, or medium-resolution imaging for dentoalveolar imaging, or large FOV for dentofacial orthopedic imaging). The combination of CBCT with optical imaging and phase contrast tomography, as well as the extension of its application for non-dental pathologies would be revolutionary steps in the coming decades.



 XML Download
XML Download