

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Allergen immunotherapy is a treatment method of administering increasing doses of clinically relevant allergens to patients with allergic disease in order to decrease their hypersensitivity to the allergen.1 The clinical efficacy of allergen immunotherapy has been proven for the treatment of Hymenoptera hypersensitivity, allergic rhinitis (AR), allergic asthma, and atopic dermatitis (AD).2345
Despite the proven clinical efficacy, cost-effectiveness, and safety of subcutaneous allergen immunotherapy (SCIT) in the treatment of allergic diseases, SCIT has not been frequently applied in clinical practice for the treatment of patients with allergic diseases.678 In the conventional schedule of SCIT, weekly hospital visits are required for 12–16 weeks during the initial build-up phase, and this inconvenience is a major obstacle for starting SCIT in patients with allergic diseases.7 To overcome this disadvantage, accelerated schedules of SCIT have been developed to reduce the time and effort of the patient during the initial build-up phase.7910 The initial build-up phase of SCIT administering maximum maintenance dose of allergen extract can be completed within 2–3 days in the rush schedule of SCIT, or in one day in the ultra-rush (UR) schedule of SCIT (UR-SCIT).79101112 However, rush-SCIT or UR-SCIT are associated with higher incidences of systemic reaction (SR) (27%–100%) than the conventional schedule of allergen immunotherapy (0.84%–46.7%).79 There have been limited numbers of studies evaluating the safety of UR-SCIT in patients with AD.91112 In our previous study, the incidence of SR was 28.9% (13 of 45) in patients with AD during UR-SCIT with aluminum hydroxide-adsorbed house dust mite (HDM) extract.9 Due to a high risk of SR, UR-SCIT typically has been conducted in a hospital admission setting to monitor the development of SR.910
The severity and incidence of SR during SCIT are dependent on the allergenic potency of the allergen extract.13 We hypothesized that high incidences of SR during UR-SCIT in previous studies were originated from a high allergenic potency of the allergen extract used for UR-SCIT. The risk of SR during UR-SCIT might be reduced by using an optimal allergen extract with low allergenic potency but having reasonable evidence of clinical efficacy.614 In this study, we evaluated the safety of UR-SCIT with tyrosine-adsorbed HDM extract conduced in an outpatient clinic in patients with AD and AR.
MATERIALS AND METHODS
Study design
This study was designed as an observational cohort study with retrospective analysis to assess the safety of UR-SCIT with HDM extract in patients with AD and AR. This study was conducted at a single academic center (Ajou University Hospital, Suwon, Korea) and approved by the Institutional Review Board of Ajou University Hospital in 2018 (approval number: AJIRB-MED-MDB-18-037). Patients were recruited from February 2014 to September 2018 at an outpatient clinic. All patients were informed of the risk of SR during the UR-SCIT with HDM extract and provided written consents.
Patients
UR-SCIT was performed in 538 patients with AD and/or AR in this study. All patients were over 6 years of age (6–58 years). The patients were classified into the AD group and the AR group according to the patient's chief complaint. The AD group included 512 patients with moderate-to-severe AD and the AR group included 26 patients with perennial AR with persistent symptoms (Table 1). The patients with AD showed the typical clinical features compatible with the diagnostic criteria for AD suggested by Hanifin and Rajka,15 and their clinical severity of AD was moderate-to-severe according to the investigator global assessment.16 The perennial AR with persistent symptoms was classified according to the international guideline.17 All patients showed a strong positive result (≥ 3.5 kU/L) on the test for serum-IgE antibody to Dermatophagoides pteronyssinus (D. pteronyssinus) and/or Dermatophagoides farinae (D. farinae) by the ImmunoCAP assay (ThermoFisher Scientific, Waltham, MA, USA). The inclusion and exclusion criteria of patients for allergen immunotherapy were consistent with the international position papers on allergen immunotherapy.218 The patients who received UR-SCIT with HDM extract in this study were students, workers, or outdweller having difficulty for frequent hospital visits during the initial build-up phase.
Table 1
Baseline characteristics of patients with atopic dermatitis and allergic rhinitis who received ultra-rush subcutaneous allergen immunotherapy
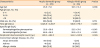
The patients were classified into atopic dermatitis group and allergic rhinitis group according to the patients' chief complaint. Data are expressed as means ± standard deviation or numbers with percentages.
![]()
Preparation of allergen extract for the UR-SCIT
A HDM preparation containing a mixture of D. pteronyssinus and D. farinae extracts (50%:50%) adsorbed to tyrosine (Tyrosine-S®; Allergy Therapeutics PLC., West Sussex, UK) was used for SCIT in this study. This HDM preparation was composed of 2 vials (No. 1 initial concentration vial and No. 2 maintenance concentration vial) with an 8-fold increase in allergen concentration between the 2 vials. The manufacturer recommends a schedule of weekly subcutaneous administrations of increasing doses (0.1, 0.2, 0.3, 0.5, 0.7 and 1.0 mL) of each vial (No. 1 and No. 2 vials) for 12 weeks, a maintenance dose (1 mL of No. 2 vial) at week 14, then the same maintenance doses at intervals of 4–6 weeks.
Procedure of UR-SCIT
All patients received premedication with antihistamines (levocetirizine 5 mg and/or fexofenadine 120 mg) at least 30 minutes prior to the start of UR-SCIT, and continued the antihistamines daily until the timing for administration of maximum maintenance dose (administration of 1 mL of maintenance HDM concentration) at 4–8 weeks after UR-SCIT. For UR-SCIT, patients received an intravenous administration of normal saline to obtain an emergency vascular access during the UR-SCIT in the day-care unit of the outpatient clinic (either on a bed or a comfort chair).
A maximum maintenance dose of tyrosine-adsorbed HDM extract (1 mL of maintenance vial) was divided into 4 increasing doses (0.1, 0.2, 0.3, and 0.4 mL) and administered to the patients by subcutaneous injection at 2-hour intervals for 8 hours (Table 2). Patients were observed by nurse and physician for at least 2 hours after the injection of the last scheduled allergen dose, then discharged from the day-care unit of the outpatient clinic.
Table 2
Schedules for the ultra-rush subcutaneous allergen immunotherapy and follow-up maintenance subcutaneous immunotherapy
![]()
To reach the maximum maintenance dose of the HDM extract, the administration of 0.8 mL of maintenance concentration vial (No. 2) was scheduled at 2–4 weeks (preferably at 2 week) after UR-SCIT, and then the administration of 1.0 mL of the maintenance concentration vial was scheduled at 4–8 weeks (preferably at 6 week) after UR-SCIT. After administration of the 1.0 mL of the maintenance dose or maximum tolerable dose without side effects, the same doses were administered at every 4–6 weeks as recommended by the manufacturer of the HDM extract for maintenance SCIT. If the patient experienced SR or clinical exacerbation developed after UR-SCIT or maintenance SCIT, the administration dose of allergen was reduced to a one-step lower dose from the last administered dose.
Assessment of SR
To evaluate the safety of the UR-SCIT, the type of SR, allergen dose-induced SR, and onset timing of SR were assessed. The detailed type of SR and onset timing of SR were recorded in electronic medical record system. The data were then retrospectively analyzed. The severity of SR associated with UR-SCIT was classified according to the World Allergy Organization grade system.19 When SR occurred during UR-SCIT, rescue medications (chlorpheniramine, dexamethasone, and/or epinephrine) were administered to the patients and UR-SCIT was discontinued at the physician's discretion.
Statistical analysis
Data on the baseline clinical characteristics are expressed as means ± standard deviation or numbers with percentages. Mann-Whitney U test (age, total IgE, and specific IgE) or χ2 test (gender) was used to compare the baseline characteristics of patients between groups. The incidence of SR was presented as absolute patient numbers and percentages among the total numbers of patients who received UR-SCIT. The Fisher's exact test was used to compare the incidence of SR of UR-SCIT between AD group and AR group. A P value of less than 0.05 was considered to be statistically significant.
RESULTS
Incidence, type and severity grade of SR during the UR-SCIT
SR was observed in 12 of 538 patients (2.2%) with AD and/or AR during the UR-SCIT. The incidence of SR was significantly higher in the AR group (3/26; 11.5%) than AD group (9/512; 1.8%) (P = 0.017) (Table 3). However, there was no significant difference in incidence of SR between AD patients with AR symptoms (4/286; 1.4%) and those without them (5/226; 2.2%) (P = 0.517). The incidence of SR was significantly higher in patients with AR symptom only (2/10, 20.0%) than those with AD symptom only (5/221, 2.3%) (P = 0.032). The incidence of SR was 0% (0 of 16) in the age group between 6–11 years, 4.8% (6 of 124) in the age group between 12–18 years, and 1.5% (6 of 398) in the age group between 19–58 years (Table 3).
Table 3
Incidence of systemic reaction (SR) in patients with atopic dermatitis and allergic rhinitis during the ultra-rush subcutaneous allergen immunotherapy classified by different age groups

The patients were classified into atopic dermatitis group and allergic rhinitis group according to the patients' chief complaint. Data are expressed as numbers with percentages.
![]()
The severity grades of the observed SR were mild-to-moderate (grade 1 in 7 patients, grade 2 in 4 patients, and grade 3 in 1 patient) in the 12 patients who experienced SR. Severe SR or near fatal SR (grade 4 SR or grade 5 SR) was not observed (Table 4).
Table 4
Type, severity grade and onset timing of systemic reaction (SR) in patients with atopic dermatitis and allergic rhinitis during the ultra-rush subcutaneous allergen immunotherapy

The patients were classified into atopic dermatitis group and allergic rhinitis group according to the patients' chief complaint.
UR-SCIT, ultra-rush schedule of subcutaneous allergen immunotherapy; C, intravenous administration of 4 mg of chlorpheniramine; D, intravenous administration of 5 mg of dexamethasone; E, intramuscular administration of 0.3 mg of epinephrine.
![]()
Grade 1 SR was spontaneously resolved in 6 patients of the AD group without rescue medications. Chlorpheniramine and dexamethasone was administered as a rescue medication in 1 patient of the AR group who showed grade 1 SR. Grade 2 and 3 SRs were resolved after the intravenous administration of chlorpheniramine and dexamethasone in 3 patients of the AD group and 1 patient of the AR group. One patient of the AR group who experienced a grade 2 SR showed improvement after an intramuscular administration of epinephrine and the intravenous administration of chlorpheniramine and dexamethasone (Table 4).
Maximum allergen dose administered during the UR-SCIT and the onset timing of SR
The scheduled 4 increasing doses of HDM extract could be administered in 535 of 538 patients (99.4%) with AD and/or AR except 3 patients who experienced SR before the administration of the last scheduled dose (0.4 mL of maintenance concentration) during the UR-SCIT (Table 4).
SR was observed within 2 hours in 11 patients during UR-SCIT after administration of the scheduled dose of HDM extract except 1 patient who experienced a grade 2 SR at 5.5 hours after the administration of the last scheduled dose (0.4 mL) of HDM extract (Table 4). This patient visited the emergency room of our hospital, and SR was resolved after the intravenous administration of chlorpheniramine and dexamethasone.
Short-term compliance during maintenance SCIT after the UR-SCIT
The compliance rate of maintenance SCIT at the second follow-up visit (at 4–8 weeks) after the UR-SCIT was 95.5% (489 of 512) in the AD group and 92.3% (24 of 26) in the AR group (Table 5).
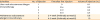
Table 5
Short-term compliance of patients for 2 follow-up visits over 4–8 weeks of the maintenance schedule of subcutaneous allergen immunotherapy after the ultra-rush subcutaneous allergen immunotherapy in patients with atopic dermatitis and allergic rhinitis

The patients were classified into atopic dermatitis group and allergic rhinitis group according to the patients' chief complaint. Data are expressed as numbers with percentages.
UR-SCIT, ultra-rush schedule of subcutaneous allergen immunotherapy; SCIT, subcutaneous allergen immunotherapy.
![]()
Maximum allergen dose administered during maintenance SCIT
The scheduled maximum allergen dose (1 mL of maintenance concentration) was administered in 89.6% (438/489) of the AD group and 83.3% (20/24) of the AR group at the second follow-up visit for maintenance SCIT (at 4–8 weeks after UR-SCIT) (Table 5). The administration dose of HDM extract was reduced from the scheduled dose (1 mL) in 3 of 489 patients (0.6%) in the AD group and 2 of 24 patients (8.3%) in the AR group who experienced SR during the UR-SCIT at the second follow-up visit for maintenance SCIT. The administration dose of HDM extract was reduced from the scheduled dose (1 mL) at the second follow-up visit for maintenance SCIT in 25 of 489 patients (5.1%) in the AD group and 1 of 24 patients (4.2%) in the AR group due to the development of clinical exacerbation at 12–48 hours after the UR-SCIT or the first maintenance SCIT (Table 5).
DISCUSSION
In this study, SR was observed in 12 of 538 patients (2.2%) with AD and/or AR during the UR-SCIT with tyrosine-adsorbed HDM extract conducted in an outpatient clinic. The severity grades of the observed SRs were mild-to-moderate (grade 1–grade 3). SR was observed within 2 hours after administration of the last scheduled dose of HDM extract in 11 of 12 patients who experienced SR. These results suggest that the UR-SCIT with tyrosine-adsorbed HDM extract is well-tolerated in patients with allergic disease and can be safely conducted in an outpatient clinic.
This report is the first clinical study evaluating the safety of UR-SCIT with tyrosine-adsorbed HDM extract in patients with AD and AR. We tried to find a safe HDM extract for SCIT with low risk of SR during UR-SCIT. The severity and incidence of SR during SCIT are dependent on the potency of the allergen extract.12 We searched for a HDM preparation for SCIT with a relatively low allergenic potency and low incidence of SR but having reasonable evidence of clinical efficacy in patients with AD and AR.61420 A previous study compared the immunological potencies of 3 kinds of commercially available HDM extracts for SCIT (aluminum hydroxide-adsorbed HDM extract, tyrosine-adsorbed HDM extract, and aqueous HDM extract) in patients with allergic diseases.21 That study showed that immunological potency inducing allergen-specific IgG4 antibody was the highest in aqueous HDM extract and the lowest in tyrosine-adsorbed HDM extract. Another previous study reported a very low incidence of SR (0.35%; 45 of 12,546 injections) during the conventional schedule of SCIT with tyrosine-adsorbed HDM extract in patients with allergic diseases.20 Therefore, in this study, we used a tyrosine-adsorbed HDM extract for UR-SCIT. As expected, the incidence of SR during the UR-SCIT (2.2%; 12 of 538 patients) with tyrosine-adsorbed HDM extract in this study was found to be lower than the incidence of SR during the UR-SCIT (28.9%; 13 of 45 patients) with aluminum hydroxide-adsorbed HDM extract reported in our previous study.912
The recently developed modified allergen extracts for SCIT (depigmented, glutaraldehyde-treated, polymerized, and aluminum hydroxide-adsorbed allergen extract) can be administered with the UR-SCIT schedule in an outpatient clinic, specifically by administrating a maximum allergen dose on the first day by 2 injections with a 30 minutes interval.12 A very low incidence of SR (0.7%; 8 of 1,068 patients) and low severity of SR (grade 1 or 2 only) were reported during the UR-SCIT with this SCIT preparation in a previous report.10 However, this modified allergen extract for SCIT is currently only available in limited area of the world (European countries), and there have been limited studies on the long-term clinical efficacy of SCIT with this allergen extract in patients with allergic diseases.22
UR-SCIT has several important practical advantages over a conventional schedule of SCIT in patients with allergic diseases: reducing the needs for frequent hospital visits and saving patient's time for the initial build-up phase of SCIT; better compliance; and probably a faster onset of clinical efficacy of SCIT.9101112 Therefore, the result of this study on the safety of the UR-SCIT with tyrosine-adsorbed HDM extract can be useful for the treatment of patients with allergic diseases.
In this study, we performed UR-SCIT in 512 patients with moderate-to-severe AD. We also evaluated the safety of SCIT in patients with AD during the maintenance phase for 4–8 weeks after UR-SCIT. In a previous study on the clinical efficacy and safety of SCIT in 101 patients with AD, clinical exacerbation of AD developed at 12–48 hours after subcutaneous administration of allergen extract (“delayed reaction”) was observed in 5 patients (5.0%) with AD.23 In this study, the delayed reaction was suspected based on a the physician's careful medical history in 5.1% (25 of 489) of patients with AD at second follow-up visit for the maintenance SCIT (at 4–8 weeks after UR-SCIT). However, this delayed reaction of SCIT in patients with AD has not been described in recent clinical studies.6222425 Confirmation of the cause-result relationship between SCIT and exacerbation of AD is difficult due to the fact that clinical exacerbations of AD can be frequently induced by multiple other triggering factors (air pollution, exposure to toxic chemical, and physical or emotional stresses) in patients with moderate-to-severe AD.26 To confirm the incidence of delayed reaction induced by SCIT in patients with AD, further clinical study on double-blind placebo-controlled SCIT challenge is required.
This study has several limitations, including the fact that it is an observational study with retrospective analysis, a single center study, and has of a relatively small number of patients with AR. In this study, the incidence of SR was higher in AR group (11.5%) than AD group (1.8%). However, there was no significant difference in incidence of SR between AD patients with AR symptoms (1.4%) and those without them (3.1%). Therefore, further clinical studies with larger numbers of patients with AD and AR will be needed to evaluate a possible existence of disease phenotype-related difference in incidence of SR during UR-SCIT.
The number of allergen preparations currently available for SCIT is limited.21 Moreover, these allergen preparations for SCIT have disadvantages in terms of a lack of standardized information on their allergenic potency, safety, and clinical efficacy for allergic diseases (objective clinical response rate).27 Although various trials have been performed to improve the clinical efficacy and safety of SCIT, the development of new allergen preparations for SCIT is difficult in these days due to strict regulatory restrictions by governments, the high costs of clinical trials, and the risks of unexpected side effects during clinical trials.27 Therefore, trials to modify and improve the application method of currently available SCIT preparations could be a reasonable approach to increase the application of SCIT in patients with allergic diseases.
In conclusion, the UR-SCIT with tyrosine-adsorbed HDM extract conducted in an outpatient clinic was tolerable in patients with AD and AR. The UR-SCIT can be a useful method to start a SCIT in patients with AD and AR.
 XML Download
XML Download