

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Chronic cough is one of the most common respiratory complaints in outpatient clinics worldwide,12 with cough variant asthma (CVA), non-asthmatic eosinophilic bronchitis (NAEB), upper airway cough syndrome (UACS), and gastroesophageal reflux-related cough (GERC) being the most common causes of chronic cough.23 Allergic rhinitis (AR) is a common disease affecting 30% of the global population and 9% of Asian-Pacific adults.456 Interestingly, AR patients often suffer from chronic cough.78 Some previous studies with small cohorts showed that in addition to UACS,9 chronic cough in AR patients is caused by CVA or NAEB.1011 However, large cohort epidemiological studies on the prevalence and etiology of chronic cough in AR patients are still lacking.
Additionally, accessible and noninvasive indicators are needed to accurately identify the causes of chronic cough in AR patients. A high fraction of exhaled nitric oxide (FeNO) indicates airway eosinophilic inflammation and has been recommended as a surrogate marker for the diagnosis of asthma.12 Thus, FeNO measurements may be useful for screening rhinitis patients with asthma-like symptoms.13 Indeed, it has been suggested that nasal nitric oxide (nNO) is also correlated with FeNO, bronchial responsiveness, and inadequate asthma control.14 Studies with small sample sizes have demonstrated that FeNO is a marker for eosinophilic inflammation caused by CVA and NAEB in chronic cough patients.1516 However, the diagnostic value of FeNO and nNO in assessing CVA and NAEB in AR patients with chronic cough remains unclear.1718 CVA is associated with airway hyper-responsiveness (AHR), which needs to be confirmed by the bronchial provocation test (BPT).19 The forced expiratory volume/1 second (FEV1, %) is regarded as the index of bronchial obstruction.20 However, it has been reported that small airways, which were usually defined as airways < 2 mm in internal diameter without cartilage, are the major site of airflow limitation in both asthma and chronic obstructive pulmonary disease.21 In this regard, forced expiratory flow at 25% and 75% of pulmonary volume (FEF25–75) is an approximate parameter that can reflect distal airway caliber and obstruction of small airways, particularly as several studies have demonstrated that a reduction in FEF25–75 can predict the presence of AHR,222324 in a more sensitive pattern than both FEV1 and FEV1/forced vital capacity (FVC). In other words, patients with mild asthma can exhibit normal FEV1, but impaired FEF25–75. To date, however, the diagnostic value of FEF25–75 for CVA in AR patients with chronic cough has not been determined.
In view of these findings, we hypothesized that FeNO, nNO, and FEF25–75 might serve as useful indicators for discriminating CVA and/or NAEB in AR patients with chronic cough. Therefore, in the current study, we recruited a large cohort of AR patients in order to evaluate the epidemiology and etiology of chronic cough in that population. Moreover, we also examined the potential diagnostic values of FeNO, nNO, and FEF25–75 in the etiological diagnosis of AR patients with chronic cough.
MATERIALS AND METHODS
Subjects and study protocol
The protocol for this study was approved by the local Ethics Committee of Beijing Tongren Hospital, Capital Medical University, China (approval number: TRECKY2013-KS-37), and a signed Informed Consent document was obtained from each participant prior to enrollment in the study. Patients who visited the Allergic Rhinitis and Rhinology Clinic at the hospital between July 2013 and June 2016 were consecutively screened for AR according to the 2008 international guideline of Allergic Rhinitis and its Impact on Asthma.4 AR was diagnosed based on its typical clinical features (Supplementary Data S1) and skin prick test (SPT) results. Each subject also underwent nasal endoscopy. Chronic cough was defined as a cough that was the sole or dominant symptom and had persisted for at least 8 weeks without any accompanying abnormal lung radiography results. Chronic cough patients with AR were eligible for enrollment if they met the following criteria: 1) age ≥ 18 years, 2) no previous diagnosis of asthma, and 3) non-smokers or ex-smokers who stopped smoking for at least 6 months prior to enrollment. Patients were excluded if they: 1) were in lactation and breastfeeding; 2) were in a pregnancy; 3) had significant psychological problems that may have caused an inability to comply with the study protocol; 4) had acute upper or lower respiratory tract infections within the previous 3 weeks; or 5) had taken systemic corticosteroids, antihistamines, leukotriene modifiers, medications for chronic cough, angiotensin-converting enzyme inhibitors, or any intranasal medication within the previous 2 weeks. Sixty AR patients without chronic cough symptoms and/or wheezing were randomly selected from the group of enrolled patients to serve as a control group (AR-only). An outline of the study protocol is illustrated in Fig. 1, and the detailed diagnostic criteria are summarized in Supplementary Data S1.
 | Fig. 1Schematic diagram of the screening and diagnostic protocol used for chronic cough in AR patients.AR, allergic rhinitis; BDT, bronchial dilation test; BPT, bronchial provocation test; CVA, cough variant asthma; Eos, Eosinophils; FEF25–75: forced expiratory flow at 25% and 75% of pulmonary volume; FeNO, fraction of exhaled nitric oxide; FEV1, forced expiratory volume in 1 second; GERC, gastroesophageal reflux-related cough; GERD, gastroesophageal reflux disease; GerdQ, gastroesophageal reflux disease questionnaire; ICS, inhaled corticosteroids; INCS, intranasal corticosteroids; LABA, long-acting beta2-agonist; NAEB, non-asthmatic eosinophilic bronchitis; nNO, nasal nitric oxide; PPI, proton pump inhibitor; UACS, upper airway cough syndrome; VAS, visual analogue scales; IgE, immunoglobulin E.
*If FEV1 ≥ 70% predicted value, then conducted BPT; otherwise conducted BDT. †Etiological treatment: CVA, ICS plus bronchodilators (budesonide/formoterol, 320/9 µg bid 4 weeks, then reduced to 160/4.5 µg bid for at least 4 weeks at the relief of symptoms); NAEB, ICS (budesonide, 400 mg bid for 8 weeks); GERC, 1) lifestyle modification (losing weight; avoiding snacks at night, acidic drink, coffee, alcohol, chocolate, oily foods, and so forth) and 2) PPI (omeprazole, 20 mg bid). All the above treatments continued for at least 12 weeks; UACS, INCS (budesonide, 128 mg bid for 12 weeks) and second-generation antihistamine po (loratadine, 10 mg daily for 4 weeks). ‡Besides the etiological treatment for CVA, NAEB, GERC and the managements for GERC, all chronic cough patients received targeted therapy for AR.
|
During the initial diagnosis of CVA, NAEB, and GERC, patients with chronic cough underwent spirometry, a BPT using methacholine inhalation, and an induced sputum examination as well as completed a gastroesophageal reflux disease (GERD) questionnaire (GerdQ). Subsequently, they received therapies (8–12 weeks) that included intranasal corticosteroids, antihistamines, and specific etiological treatments for CVA, NAEB, and GERC (Fig. 1). Finally, the diagnoses of CVA, NAEB, GERC, and UACS were confirmed by the responses to the above specific treatments at the end of the fourth week, based on a 100-mm linear cough visual analogue scale (VAS) which has been endorsed by the European Respiratory Society.25 Patients with a cutoff value of VAS reduction ≥ 50% were considered responsive to treatment.2627 Patients who failed to respond to all treatments (including treatment for UACS) were assigned to the “undefined group.” In all the patients, clinical parameters (including FeNO, nNO, and FEF25–75 levels) and the assessment of therapy responses were blinded to the investigators throughout the study.
Specific tests
The atopic status was measured by SPTs, using a panel of 21 aeroallergens (The corresponding details can be found in the Supplementary Data S1), and atopy was confirmed when a positive SPT was linked to at least 1 of the aeroallergens.28 FeNO and nNO were measured by a portable NIOX device (Aerocrine AB, Solna, Sweden) prior to the performance of induced sputum and pulmonary function tests, and BPT.29 Induced sputum was collected using previously described methods.30 Spirometry (Master Screen-body + Diffusion + APS; JAEGER, Hoechberg, Germany) and BPT were performed according to standardized procedures recommended by the American Thoracic Society.31 Peripheral blood eosinophil percentages and levels of total serum immunoglobulin E (IgE) were also measured. Detailed information concerning the aforementioned tests is provided in the Supplementary Data S1.
Statistical analysis
All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 19.0 (IBM Corp., Armonk, NY, USA). Values for continuous variables are expressed as the median with an interquartile range or as the mean ± standard deviation. Comparisons between continuous variables were made using parametric analysis of variance (ANOVA; for normal distributions) or the nonparametric Kruskal-Wallis test (for abnormal distributions). The nonparametric χ2 test was used to compare categorical variables. Pearson and Spearman correlation coefficients were applied to the correlation analyses of variables with and without a normal distribution, respectively. Receiver operating characteristic (ROC) curve, area under the curve (AUC), and the optimal cutoff value of FeNO, nNO, and FEF25–75, were calculated according to the method described by Hanley and McNeil.32 A P value of < 0.05 was considered statistically significant.
As continuous test variables, FeNO and FEF25–75, were converted to dichotomous state variables based on the ideal cutoff values and served as 2 new models. Subsequently, a multiple logistic regression was conducted to acquire a predictive equation for calculating a new variable (i.e., a combined model). ROC curves were then determined for the 3 dichotomous state variables. Finally, using the 3 dichotomous state variables, differentiation of CVA was performed by comparing their AUCs with the χ2 test.32
RESULTS
Prevalence of chronic chough in patients with AR
During the study period, a total of 1,680 AR patients were consecutively screened, of whom 324 (19.3%) met the diagnostic criteria for chronic cough. Overall, 8 patients were excluded because of unsuccessful sputum induction, and the remaining 316 patients with chronic cough were systematically investigated according to specific protocols for etiological analysis. We determined that 87 cases (27.5%) of chronic cough were induced by NAEB, 78 (24.7%) by CVA, 16 (5.1%) by GERC, and 81 (25.6%) by UACS. Patients with either NAEB or CVA (n = 165, in total) were assigned to the common group designated as CVA/NAEB, because they shared some common features such as airway eosinophilic inflammation and corticosteroid sensitivity. After treatment, 54 (17.1%) patients with decreased VAS values < 50% from baseline were categorized into the undefined group, and they were also found to not conform to the primary diagnostic criteria of CVA, NAEB, and GERC. Because AR-targeted therapy may improve cough in a subset of patients with AR, we speculated that AR patients diagnosed with NAEB, CVA, and GERC may also have UACS, indicating the double etiologies of chronic cough in these patients with AR. Indeed, 3 cases of patients with CVA were also diagnosed as GERC, thus indicating the presence of multiple etiologies of chronic cough.
Comparison of clinical characteristics among the studied groups
The demographic characteristics of AR patients with and without chronic cough are summarized in Table 1. Among the 316 subjects investigated, 66.1% ([53 + 52 + 58 + 9 + 37]/316) had persistent allergic rhinitis (PAR) and 89.9% ([69 + 79 + 77 + 14 + 45]/316) had moderate-to-severe AR. The ratios of intermittent allergic rhinitis (IAR) to PAR and mild to moderate-to-severe AR in individual groups were not statistically significant (P > 0.05). Also, no statistically significant differences were found in terms of sex and age among the different groups (i.e., AR patients without chronic cough [AR-only], AR patients with various etiologies of chronic cough, including NAEB, CVA, UACS, GERD, and the undefined group). Although there was a significant overall difference in body mass index according to ANOVA analysis (P = 0.04), further analyses using the Bonferroni test demonstrated no significant difference between any 2 groups (P > 0.05). Also, there were no statistically significant differences in other clinical parameters, including total serum IgE and nasal eosinophils grades among the different groups; however, the blood eosinophil levels were found to be significantly higher (P < 0.05) in AR patients with CVA as compared with AR-only patients.
Table 1
Characteristics of AR patients with different causes of chronic cough and without chronic cough (AR-only)
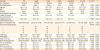
Data are expressed as the number (%), mean ± standard deviation or median (interquartile range).
AR, allergic rhinitis; BMI, body mass index; CVA, cough variant asthma; FEF25–75, forced expiratory flow between 25% and 75% of pulmonary volume; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; GERC, gastroesophageal reflux-related cough; IAR, intermittent allergic rhinitis; IgE, immunoglobulin E; NAEB, non-asthmatic eosinophilic bronchitis; PAR, persistent allergic rhinitis; UACS, upper airway cough syndrome; VAS, visual analog scale; nNO, nasal nitric oxide; FeNO, fraction of exhaled nitric oxide.
*There is significant difference (P < 0.05) between the marked group and the other groups (also including another marked group); †There is significant difference (P < 0.05) only between the 2 marked groups.
![]()
Comparison of sputum eosinophil percentages, FeNO levels, and nNO levels among the different groups of AR patients
AR patients with CVA and NAEB exhibited significantly higher (P < 0.05) sputum eosinophil percentages compared with those who had other causes of chronic cough or AR-only (Table 1 and Fig. 2A). The FeNO levels (50.2 [47.1–53.4] ppb) and NAEB (41.2 [39.0–43.3] ppb) were significantly higher in AR patients with CVA than in those with UACS (25.0 [23.3–27.8] ppb), GERC (24.0 [20.9–27.1] ppb), undefined cough (23.7 [22.1–25.3] ppb), and AR-only (23.8 [21.4–26.2] ppb) (all P < 0.01 (Fig. 2B). In addition, the nNO levels (366.7 [335.6–397.8] ppb) was significantly higher in AR patients with CVA than in AR-only (310.4 [291.9–328.9] ppb, P < 0.05), while there were no statistically significant differences among the other groups (Fig. 2C).
 | Fig. 2Comparisons of induced sputum Eos (%) (A), FeNO (ppb) (B), nNO (ppb) (C), FEV1 (D), and FEF25–75 (E) among the different groups.NS, not significant; AR-only, allergic rhinitis patients without chronic cough; CVA, cough variant asthma; Eos, Eosinophils; FEF25–75, forced expiratory flow at 25% and 75% of pulmonary volume; FeNO, fraction of exhaled nitric oxide; FEV1, forced expiratory volume in 1 second; GERC, gastroesophageal reflux-related cough; NAEB, non-asthmatic eosinophilic bronchitis; UACS, upper airway cough syndrome; nNO, nasal nitric oxide.
*Statistical significance at P < 0.05; †Statistical significance at P < 0.01.
|
Comparison of FEV1 and FEF25–75 among various groups of AR patients
The FEV1 and FEF25–75 values in AR patients with and without chronic cough are shown in Table 1 and portrayed in Fig. 2D and E. The FEV1 was significantly lower in the CVA group than in the UACS group (P < 0.05, Fig. 2D). Furthermore, the FEF25-75was significantly lower in the CVA group than in the other groups (P < 0.01, Fig. 2E).
Correlation of FeNO with sputum eosinophils, nNO, FEV1, and FEF25–75 in AR patients with chronic cough
The FeNO concentrations were positively correlated with the concentrations of sputum eosinophils and nNO in all AR patients with chronic cough (r = 0.885, r = 0.436, respectively; both P < 0.01, Fig. 3A and B). In contrast, FeNO was negatively correlated with both FEV1 (r = −0.221, P < 0.01, Fig. 3C) and FEF25–75 (r = −0.451, P < 0.01, Fig. 3D).
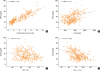 | Fig. 3Correlation of FeNO (ppb) with induced sputum Eos (%) (A), nNO (ppb) (B), FEV1 (C), and FEF25–75 (D). Pearson correlation coefficients were used for expressing the correlations.Eos, Eosinophils; FEF25–75: forced expiratory flow at 25% and 75% of pulmonary volume; FeNO, fraction of exhaled nitric oxide; FEV1, forced expiratory volume in 1 second; nNO, nasal nitric oxide.
|
FeNO and nNO levels for differentiating CVA, NAEB, and CVA/NAEB in AR patients with chronic cough
ROC curves were created to assess the diagnostic accuracy and optimal cutoff values of FeNO in patients with CVA (Fig. 4A), NAEB (Fig. 4B), and CVA/NAEB (Fig. 4C), and NAEB within the non-asthmatic chronic cough population (chronic cough without CVA, Fig. 4D). The AUC values of FeNO in diagnosing CVA, NAEB and CVA/NAEB, were 0.855, 0.699, and 0.923, respectively; that in diagnosing NAEB in chronic cough without CVA was 0.908 (Table 2). Similarly, the corresponding AUC values of nNO in diagnosing CVA, NAEB and CVA/NAEB were 0.564, 0.511, and 0.557, respectively; in diagnosing NAEB in chronic cough without CVA was 0.538. Specifically, FeNO at 43.5 ppb exhibited the optimal sensitivity (75.6%) and specificity (86.6%) for predicting diagnosis of CVA, together with the positive predictive value (PPV, 64.8%) and negative predictive value (NPV, 91.6%). FeNO at 32.5 ppb revealed the optimal sensitivity (81.6%) and specificity (64.2%) for predicting a diagnosis of NAEB, along with the PPV (46.4%) and NPV (90.2%). FeNO at 32.5 ppb showed better sensitivity (84.8%) and specificity (91.4%) for identifying patients who suffered from CVA/NAEB. Also, it demonstrated better PPV (91.5%) and NPV (84.7%), as compared with those calculated for the diagnosis of NAEB. In addition, FeNO at 32.5 ppb exhibited the optimal sensitivity (81.6%) and specificity (91.4%) for predicting diagnosis of NAEB in chronic cough without CVA (Table 2), together with PPV (84.5%) and NPV (89.6%).
 | Fig. 4ROC curves of FeNO, nNO, FEV1, and FEF25–75 for assessing diagnostic accuracy. ROC curves of FeNO and nNO for assessing the diagnostic accuracy for CVA (A), NAEB (B), CVA/NAEB (C), ROC curves of FeNO and nNO for assessing the diagnostic accuracy for NAEB in chronic cough without CVA (D), FEV1 and FEF25–75 for assessing the diagnostic accuracy for CVA in all chronic cough patients (E), for CVA only in CVA/NAEB patients (F), and FeNO model, FEF25–75 model, and combined model for assessing the diagnostic accuracy for CVA (G).ROC, receiver operating characteristic; CVA, cough variant asthma; CVA/NAEB, either NAEB or CVA; FEF25–75, forced expiratory flow at 25% and 75% of pulmonary volume; FeNO, fraction of exhaled nitric oxide; FEV1, forced expiratory volume in 1 second; NAEB, non-asthmatic eosinophilic bronchitis; nNO, nasal nitric oxide.
|
Table 2
Differential diagnostic values of FeNO and FEF25–75 in detecting CVA, NAEB and CVA/NAEB

The percentage value in the parentheses represents the prevalence of the specific disease.
FeNO, fraction of exhaled nitric oxide; FEF25–75, forced expiratory flow between 25% and 75% of pulmonary volume; AUC, area under the curve; CVA, cough variant asthma; NAEB, non-asthmatic eosinophilic bronchitis; NPV, negative predictive value; PPV, positive predictive value; ROC, receiver operating characteristic.
![]()
FEV1 and FEF25–75 for differentiating CVA in chronic cough
All the data on FEV1 and FEF25–75 obtained from the patients with chronic cough (n = 316) were used to accurately assess the values of FEV1 and FEF25–75 the diagnosis of CVA. The AUC values of FEF25–75 and FEV1 for diagnosing CVA in chronic cough were 0.860 and 0.625, respectively (Fig. 4E), and a cutoff value of 74.6% for FEF25–75 (Table 2) demonstrated the best sensitivity (80.8%) and specificity (72.7%), together with the values of PPV (49.2%) and NPV (92.0%). Because patients with NAEB or CVA (n = 165) share some common features (i.e., airway eosinophilic inflammation and corticosteroid sensitivity), we investigated whether FEF25–75 and FEV1 could differentiate patients with CVA from those in the CVA/NAEB group. As shown in Fig. 4F, the AUC values corresponding to FEF25–75 and FEV1 were 0.858 and 0.604, respectively. A cutoff value of 74.6% for FEF25–75 indicated the best sensitivity (80.8%) and specificity (69.0%), combined with the PPV (70.0%) and NPV (80.0%), for discriminating CVA from CVA/NAEB (Table 2). Based on the results mentioned above, the diagnostic efficacy of FEF25–75 for CVA in the CVA/NAEB group was not inferior to that for CVA in chronic cough, indicating that FEF25–75 could be used to further differentiate CVA from NAEB as the cause of chronic cough in AR patients.
FeNO Combined with FEF25–75 for differentiating CVA in chronic cough
The AUCs of FEF25–75 combined with FeNO, FeNO, and FEF25–75 models were 0.856 (95% confidence interval [CI], 0.812–0.893), 0.811 (95% CI, 0.763–0.853), and 0.767 (95% CI, 0.717–0.813), respectively. The AUC of FEF25–75 combined with FeNO predicted better diagnostic accuracy compared with FeNO (P < 0.05) or FEF25–75 alone (P < 0.01), respectively (Fig. 4G).
DISCUSSION
The prevalence of chronic cough in our large consecutive cohort of AR patients was 19.3%, which may be an underestimation due to the exclusion of patients with previously diagnosed asthma. Despite this, however, the current study still showed that the incidence of chronic cough in AR patients was higher than the global incidence of chronic cough (9.6%).1 Indeed, as patients with persistent and moderate-to-severe AR accounted for the majority of the patients in our chronic cough cohort, extra attention and care should be given to especially persistent and moderate-to-severe AR patients exhibiting chronic cough.
Furthermore, we conducted a systematic investigation on the causes of chronic cough in AR patients and found that in addition to UACS, NAEB and CVA acted as the common causes of chronic cough, followed by GERC. Notably, we hypothesized that UACS may co-exist with NAEB and CVA to jointly lead to chronic cough in AR patients, which is possibly veiled by AR-targeted therapy. Additionally, we found that 3 cases of AR patients with CVA who were concurrently diagnosed with GERC, suggesting that there may be multiple and complex etiologies of chronic cough in individual AR patients.
We found that 24.7% of chronic cough in AR patients were caused by CVA, indicating that CVA is an important cause of chronic cough in AR. Interestingly, we found that NAEB was the most common cause of chronic cough, with an incidence of 27.5% in our cohort of AR patients. This was much higher than what has been reported in a previous study, which indicated the incidence of NAEB in the entire population of patients with chronic cough in China to be 17.2%.33 This finding suggests a close correlation between NAEB and AR. It has been clearly established that asthma and AR share a common atopic status, certain onset risk factors, epidemiological features, and eosinophilic inflammatory processes, thus indicating a “unified airway” system.41034 In the current study, we found that NAEB often co-exists with AR, which further builds upon the concept of “unified airway” beyond that of asthma and AR. In view of this, the need for the diagnosis of NAEB should be emphasized in AR patients with chronic cough, especially in those who are resistant or have only partially responded to treatments for AR.
While it is possible that NAEB may be under-diagnosed in daily clinical practice, due to the absence of tests such as induced sputum examinations,33 it should be noted that conducting an induced sputum examination is time-consuming, manpower-dependent, and requires specialized equipment, all of which restrict its daily use in clinic. In contrast, FeNO measurement is simple to perform, noninvasive, and could be used as a reproducible tool to monitor type 2 immunity-driven eosinophilic airway inflammation.12 Some studies have previously shown that there is a statistically significant correlation between FeNO level in chronic cough and the percentage of sputum eosinophils.1635 In the current study, we found a close correlation (r = 0.885) between the percentage of sputum eosinophils and FeNO concentration in chronic cough patients with AR as the atopic background. Westerhof et al.36 have suggested that FeNO has comparable diagnostic accuracy with blood eosinophils in identifying sputum eosinophilia in adult asthma patients. In our study, consistent with the percentages of sputum eosinophils, the levels of FeNO were significantly higher in AR patients with CVA and NAEB (P < 0.05) than in the other groups, suggesting that FeNO levels may reflect the amount of eosinophilic infiltration in the lower airways of AR patients with chronic cough.
Although some studies have reported the presence of high levels of FeNO in AR subjects with CVA or NAEB,101637 to date the precise role of FeNO has not been well established in the diagnosis of NAEB. FeNO is usually used to exclude NAEB at low levels.38 A meta-analysis has suggested that while the FeNO levels could be used to discriminate CVA in adult patients with chronic cough, the diagnostic accuracy of FeNO was relatively low in patients with NAEB.39 Indeed, based on a few preliminary studies with inconsistent diagnostic accuracy and specificity of FeNO, the 2018 guidelines for chronic cough issued in Korea have conditionally recommended the use of FeNO for diagnosing NAEB.40 Since NAEB and CVA are 2 common causes of chronic cough in patients with underlying airway eosinophilic inflammation, an initial measurement of FeNO for identifying possible CVA or NAEB and for eliminating other causes of chronic cough in patients with AR may be desirable in a diagnostic protocol, particularly as both entities respond to inhaled corticosteroid therapy. In the current study, we examined the diagnostic value of FeNO levels in identifying CVA and CVA/NAEB in a well-defined cohort of AR patients. Specifically, a level of FeNO at 32.5 ppb identified CVA/NAEB with optimal sensitivity (84.8%) and specificity (91.4%), together with PPV of 91.5% and NPV of 84.7%. This is in keeping with some previously published studies, which suggest that an FeNO level at 31.5–33.9 ppb can be used for the diagnosis of corticosteroid-responsive coughs (mainly CVA and NAEB).163541 A level of FeNO at 43.5 ppb in the current study was also found to have the best ability to identify patients with CVA; with a sensitivity of 75.6%, specificity of 86.6%, PPV of 64.8%, and NPV of 91.6%. In line with this finding, a recently released study has shown that FeNO levels > 43 ppb could predict positive AHR (i.e., CVA) in Chinese patients with chronic cough.42 Collectively, these studies suggest that FeNO is a reasonable indicator for initially diagnosing CVA/NAEB in AR patients with chronic cough.
AHR is a pathophysiological feature of CVA and is confirmed by a positive reaction to the BPT. However, the BPT is not extensively used in clinical practice, due to its high cost and complicated nature to use. As a result, simple alternative parameters of pulmonary function are usually measured to identify AHR, especially during an initial investigation for the cause of chronic cough. FEF25–75 is an index of small airway function and can indicate the presence of AHR.2223 A previous study showed that the reduced FEF25–75 values suggested early bronchial involvement in patients with AR.43 Another study indicated that low FEF25–75 values may predict severe AHR, and are inversely associated with FeNO levels in adolescents.23 In our current study, we found that both FEV1 and FEF25–75 (especially FEF25–75) were negatively correlated with FeNO, suggesting that lower airway eosinophilic inflammation can negatively impact pulmonary ventilatory function, especially on functions performed by small airways. We also found that the values for FEF25–75 were significantly lower in CVA patients than in other groups of patients (P < 0.05), suggesting that FEF25–75 may be useful for identifying CVA in chronic cough patients with AR. The ROC results showed that FEF25–75 was more accurate than FEV1 in diagnosing CVA. In keeping with a previous study on Chinese population with chronic cough, which showed that FEF25–75 < 78.5% strongly predicted positive AHR,42 we showed that a cutoff value of FEF25–75 at 74.6% (slightly lower than the research mentioned above, which may be attributed to the atopic nature of the enrolled population in our study) exhibited good diagnostic sensitivity, specificity, NPV, and PPV for CVA in both chronic cough and CVA/NAEB groups. Based on these results, we propose that FEF25–75 values less than 75% may indicate CVA as a potential cause of chronic cough in patients with AR. By using the combined AUC curve model, we also showed that the combination of FeNO and FEF25–75 has a better predictive effect for CVA when compared with either FeNO or FEF25–75 alone.
Considering the diagnostic value of FeNO in CVA/NAEB and FEF25–75 in CVA, we suggest that first, we should use FeNO to discriminate CVA/NAEB from AR patients with chronic cough and then use FEF25–75 to further discriminate CVA from CVA/NAEB for the etiological diagnosis of chronic cough in AR patients. The combination of FeNO and FEF25–75 could be an effective measurement for the diagnosis of CVA. This may reduce the missed diagnosis rate of NAEB, promote timely diagnosis of CVA for asthma treatment in AR patients, and preserve clinical resources.
In addition, in the non-asthmatic chronic cough population (chronic cough without CVA), FeNO at 32.5 ppb exhibited the optimal sensitivity (81.6%) and specificity (91.4%) for predicting diagnosis of NAEB, together with PPV of 84.5% and NPV of 89.6%. Therefore, FeNO might be useful for further differentiating NAEB from chronic cough without CVA and for reducing the missed diagnosis rate of NAEB. Moreover, FeNO at 43.5 ppb and FEF25–75 at 74.6% had the best ability to identify patients with CVA. Based on these results, another strategy on the diagnosis of NAEB can be provided, namely, first identifying CVA from chronic cough using FeNO or FEF25–75, and then diagnosing NAEB in chronic cough without CVA.
Previous research has reported that there was an association of higher nNO levels with AHR and increased FeNO levels.14 In our study, nNO was correlated well with FeNO (r = 0.436, P < 0.05), and AR patients with CVA had a significantly higher (P < 0.05) nNO level than AR-only patients. However, nNO failed to discriminate CVA, NAEB, and CVA/NAEB from other causes in AR patients with chronic cough, due to AUC < 0.7.
Moreover, we observed that 5.1% of the patients enrolled in our study suffered from GERC as seen by their scores on a GerdQ and clinical responses to the management of GERC. This percentage was higher than previously reported,3344 which implied that allergic disease of the upper airway may increase the risk of GERD.45 It can be vice versa or a coincidence.
The current study demonstrated that 17.1% of the cases had decreased VAS scores < 50% from baseline and, therefore, did not meet the primary diagnostic criteria of CVA, NAEB, and GERC. Thus, this set of individuals was categorized as the “undefined group”, which may comprise 1 or more further sub-categories. However, 2 possibilities, may explain the limited improvement of the VAS score in these patients. First, they did not receive ICS treatment because atopic cough was not diagnosed. Secondly, they may suffer from GERC without acid reflux symptoms and were therefore undiagnosed according to GerdQ scores; which subsequently led to the patients not receiving any GERC-targeted treatment. Thus, capsaicin stimulation test, gastroesophageal manometry, and pH-metry with conventional methodology may be helpful in distinguishing the other category/categories in the undefined group.
There are several limitations of our study. First, the prevalence of chronic cough might have been underestimated, due to the exclusion of patients who were previously diagnosed with asthma. Secondly, a diagnosis of GERC based only on responses on a GerdQ may underestimate the prevalence of GERC. Thirdly, we did not consider the confounding effects of psychological factors (e.g., anxiety and depression).46 Thus, in some patients with AR, the causes of chronic cough may have remained undefined. Finally, we did not arrange to perform capsaicin provocative test in patients whose VAS reductions were less than 50% from baseline after treatment and that may have left their atopic cough undiagnosed. Also, a 4-week treatment window for the response assessment is relatively short. Thus, we categorized these treatment-unimproved patients (n = 54) into the undefined cough group, rather than categorizing it as unexplained cough.
In conclusion, our study found a high prevalence of chronic cough among patients visiting an allergy clinic for AR. In addition to UACS, NAEB and CVA were the leading causes of chronic cough in these cases. FeNO can be applied as a marker for identifying CVA/NAEB, and then FEF25–75 (or combined with FeNO) can be used to further differentiate CVA from CVA/NAEB as the cause of chronic cough in AR patients. Moreover, FeNO and FEF25–75 can provide another strategy for the diagnosis of NAEB, based on prior identification of CVA. Taken together, our results provide new insights into the etiological spectra of chronic cough in patients with AR and suggest a relevant and clinically applicable diagnostic protocol.
 XML Download
XML Download