

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Organic dust is an aggregate of viable and non-viable particulate matter from microbial (bacteria, fungi, viruses and protozoa), their metabolites (mycotoxins, peptidoglycans, endotoxins, glucans, enzymes, etc.), plant or animal origin (allergens including pollens, vegetal fibers, and epidermis).1 It is a well-established major air pollutant within different workplaces due to its containing of bacteria, moulds and pollens. Inhaled organic dust leads to respiratory inflammatory responses,2 with the potential mechanism of serving as a favorable medium for the numerous bacteria and microscopic fungi.3
However, epidemiological results are inconclusive. Several studies confirmed the asthma-inducing effect of organic dust exposure, while other articles reported the ambiguous results. A late recent meta-analysis similar to our topic also showed limited evidence of a causal association existing between long-term excess decline in pulmonary function and general exposure to organic dust.4
Given the inconsistencies of existing epidemiological studies, we performed the present meta-analysis to examine the association between organic dust and asthma among case-control studies. This is the first meta-analysis on this topic to our knowledge, using a unique manner to the existing literature by quantitatively synthesizing observational studies on asthma and organic dust.
MATERIALS AND METHODS
Data sources and searches
To estimate the odds of asthma associated with organic dust exposure, we searched EMBASE, PubMed and Cochrane Library databases, using the keywords “asthma” and “case-referent” or “case-control” and “organic dust” or “wood/paper/flour/grain/baker/agriculture/farm/soybean/textile dust” up to August 2018. We screened the list of references in previous reviews and selected papers to identify additional relevant studies besides databases searched above. The decision whether an identified article would be eligible for the review was made prior to initiating the search.
Study selection
Studies meeting the following criteria were included in the meta-analysis: case-control studies published in English that contained or reported the odds of asthma related to organic dust exposure with corresponding 95% confidence interval (CI). The control group of individual studies was from either healthy community members (population-based) or inpatients without asthma (hospital-based). The first 2 authors screened the titles and abstracts to identify relevant investigations independently according to the selection criteria, and resolved discrepancies on whether to include a study by consensus. We excluded the studies focused on childhood.
Quality assessment
The Newcastle-Ottawa Scale (NOS) was used to assess the quality of the studies enrolled. This tool comprises 3 parameters: selection, comparability and outcome.5 Each parameter consists of subcategorized questions: selection (a maximum of 4 stars), comparability (a maximum of 2 stars), and exposure or outcome (a maximum of 3 stars). A study can be awarded a maximum of 9 stars, indicating the highest quality. The authors independently evaluated the quality of all the studies.
Data extraction
The authors retrieved data from each article independently on the first author's name, the year of publication, source of controls, age, sex, country, organic dust type, case/controls, NOS score, asthma diagnosis, exposure duration and covariates/confounders. The adjusted odds ratio (OR) for asthma reported was used for this meta-analysis. Data from the more recent one was selected in the analysis if different studies share the same population.
Statistical analysis
ORs were combined by means of a weighted average to generate summary estimates by RevMan (version 5.2; The Cochrane Collaboration, Oxford, UK). The I2 was determined to quantify the percentage of variation across studies attributable to heterogeneity.6 We chose the fixed-effects model when I2 < 50%. In contrast, a random-effects model was applied. Studies were identified as outliers if the 95% CI of their effect size did not overlap with the estimate line of the summary estimate on the forest plot.7 Potential publication bias was evaluated using funnel plots.
RESULTS
The steps of our literature search are shown in Fig. 1. Briefly, the search yielded a total of 1,016 articles from EMBASE, PubMed, and Cochrane Library databases. No additional article was identified from articles' references screening. After full text screening, 17 studies89101112131415161718192021222324 containing 3,619 cases and 6,585 controls met our inclusion criteria. The studies included in this review were of the same case-control design and applied different types of organic dust exposure (Table, Supplementary Table S1).

Table
Characteristics of included individual studies
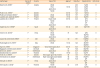
| Author/year | Source of control | Country | Type of OD | Age (yr) | Male (%) | Case/controls | NOS score |
|---|---|---|---|---|---|---|---|
| Beach et al. (2012)15 | P | Canada | Wood | 48.3 | 74/48 | 9 | |
| Flour | 18–65 | 93.4 | 30/28 | ||||
| Agriculture | 40.4 | 25/22 | |||||
| Textile | 21.7 | 27/19 | |||||
| Flodin et al. (1996)20 | P | Sweden | - | 20–65 | N/A | 79/304 | 9 |
| Flodin and Jönsson (2004)19 | P | Sweden | Wood | 20–65 | 57.7 | 53/156 | 7 |
| Jaakkola and Jaakkola (2007)21 | P | Finland | Paper | 21–63 | 45.4 | 133/316 | 7 |
| Jaakkola et al. (2003)22 | P | Finland | Paper wood | 20–64 | 42.2 | 9/14 | 8 |
| Textile | 9/13 | ||||||
| Flour | 7/7 | ||||||
| Agriculture | 15/35 | ||||||
| Kogevinas et al. (1996)23 | P | Spain | Wood | 20–44 | 48.2 | 136/1,799 | 8 |
| Agriculture | |||||||
| Flour | |||||||
| Krstev et al. (2007)9 | P | China | Wood | 37 | N/A | 6/24 | 8 |
| Textile | 183/732 | ||||||
| Agriculture | 143/572 | ||||||
| Lipscomb and Dement (1998)16 | P | USA | Wood | 40 | 97.1 | 109/225 | 8 |
| Grain flour | 12/19 | ||||||
| Mastrangelo et al. (1997)18 | H | Italy | Wood | 15–64 | N/A | 387/387 | 8 |
| 325/325 | |||||||
| Ng et al. (1994)8 | H | Singapore | Wood textile agriculture | 20–54 | 42.4 | 787/1,591 | 8 |
| Sigsgaard and Schlunssen (2004)25 | P | Denmark | Wood | 37 | 76.0 | 222/129 | 7 |
| Smit et al. (2014)24 | P | Netherland | Agriculture | 50 | 35.7 | 269/546 | 9 |
| Sripaiboonkij et al. (2009)13 | P | Thailand | Wood | 18–60 | 55.3 | 103/76 | 9 |
| Torén et al. (1999)14 | P | Sweden | Wood paper grain flour textile | 38 | 47.5 | 111/2,044 | 8 |
| Vermeulen et al. (2002)10 | P | Netherland | Paper wood agriculture textile | 48 | 47.0 | 274/274 | 8 |
| Wood | 50 | 45.6 | 8/4 | ||||
| Wang et al. (2010)12 | P | China | Agriculture | 40/7 | 8 | ||
| Textile | 9/4 | ||||||
| Wortong et al. (2015)11 | H | Thailand | Textile | 55 | 34.9 | 11/8 | 9 |
| Agricultural | 23/124 |
N/A, not available; OD, organic dust; H, hospital controls; P, population controls; NOS, Newcastle-Ottawa Scale.
![]()
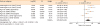
The studies that were included in our meta-analysis were published between 1994 and 2015. They were conducted mainly in Europe,10141718192021222324 but also in North America,1516 China,912 Thailand1113 and Singapore.8 The risk of asthma increased by 48% among those exposed to organic dust (OR, 1.48; 95% CI, 1.26–1.75; P < 0.00001) (Fig. 2). Subgroup analysis showed that the risk of asthma increased by 24% among population-based case-control studies (OR, 1.24; 95% CI, 1.13–1.35; P < 0.00001) (Fig. 3) and by 179% among hospital-based case-control studies (OR, 2.79; 95% CI, 1.27–6.12; P = 0.01) (Fig. 4). Agriculture dust exposure was not significantly associated with an increased/reduced risk of asthma (OR, 1.06; 95% CI, 0.72–1.56; P = 0.76; Fig. 5), while strong relationship was found between asthma and paper/wood (OR, 1.62; 95% CI, 1.38–1.90; P < 0.00001) (Fig. 6), flour/grain (OR, 1.48; 95% CI,1.11–1.97; P = 0.008) (Fig. 7), and textile dust exposure (OR, 1.50; 95% CI, 1.08–2.09; P = 0.02) (Fig. 8).
 | Fig. 2Summary of the OR of the association between the risk of asthma and organic dust exposure.SE, standard error; OR, odds ratio; CI, confidence interval.
|
 | Fig. 3Summary of the OR of the association between the risk of asthma and organic dust exposure among population-based case-control studies.SE, standard error; OR, odds ratio; CI, confidence interval.
|
 | Fig. 4Summary of the OR of the association between the risk of asthma and organic dust exposure among hospital-based case-control studies.SE, standard error; OR, odds ratio; CI, confidence interval.
|
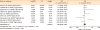 | Fig. 5Summary of the OR of the association between the risk of asthma and agriculture dust exposure.SE, standard error; OR, odds ratio; CI, confidence interval.
|
 | Fig. 6Summary of the OR of the association between the risk of asthma and paper/wood dust exposure.SE, standard error; OR, odds ratio; CI, confidence interval.
|
 | Fig. 7Summary of the OR of the association between the risk of asthma and grain/flour dust exposure.SE, standard error; OR, odds ratio; CI, confidence interval.
|
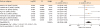 | Fig. 8Summary of the OR of the association between the risk of asthma and textile dust exposure.SE, standard error; OR, odds ratio; CI, confidence interval.
|
Other subgroup analysis according to asthma diagnosis revealed that organic dust exposure was closely associated with asthma diagnosed with classic symptoms and objective outcomes from pulmonary function (OR, 1.77; 95% CI, 1.19–2.62; P = 0.005). When we focused on the cases whose exposure duration was not less than 3 years, no positive relationship could be found between organic dust exposure and asthma (OR, 0.95; 95% CI, 0.62–1.46; P = 0.81), which may be due to different exposure extents and incomplete data.
DISCUSSION
Our results showed that organic dust exposure was positively associated with asthma, whether among population-based case-control studies or hospital-based case-control studies. Subgroup analysis indicated that paper/wood, flour/grain, and textile dust exposure, namely, most varieties of organic dust are related with asthma significantly.
Workers who are recurrently exposed to organic dust are at increased risk for several respiratory symptoms, including asthma.25 A recent research revealed that sensitization to dust extracellular vesicles was an independent risk factor for non-eosinophilic asthma (adjusted OR, 3.3; 95% CI, 1.1–10.0), and even chronic obstructive pulmonary disease and lung cancer.26 Agricultural work and multiple types of livestock are independent risk factors for developing asthma in adults.27 Self-reported exposure to any gas, smoke or dust, organic dust, dampness and mold, cold conditions and physically strenuous work, and jobs handling low molecular weight agents were associated with exacerbation of asthma. Reduction in such occupational exposures may help reduce exacerbation of asthma.28 A study from Norway revealed that dust exposure was associated with an increased incidence of work-related asthma-like symptoms.29 Garshick et al.30 reported exposure to vehicular emissions by living near heavily trafficked roadways might contribute to symptoms of chronic respiratory disease including persistent wheeze.
A previous study confirmed that exposure to inhaled organic dusts would activate inflammatory responses of monocyte, macrophages and epithelial cells through rapidly stimulating secretion of tumor necrosis factor.31 Neutrophil recruitment, pyrexia and airway epithelial cells activation could be induced by monocyte/macrophage-derived inflammatory mediators and lead to direct bronchial hyperreaction.32 Toll-like receptor 2,33 myeloid differentiation factor 88-dependent signaling34 and pattern recognition scavenger receptor A/CD204 all participate in the regulation of organic dust-induced airway inflammation. Robbe et al.35 demonstrated that exposure to agriculture dust would increase the proportion of interleukin-17 and interferon-γ positive T cells, with similar results presenting the increased frequency of activated lung macrophages (CD11c+/CD11b+) obtained from animal models exposure to organic dust extracts.3637 Poole et al.38 found that a mixed T helper cell (Th)1 and Th17 immune response was induced by repeated intranasal organic dust exposure in a murine model.
Guillam et al.39 found that Hatchery workers in sorting rooms were at increased risk of compromised respiratory health such as asthma and rhinitis due to dust exposure. Hinson et al.40 indicated that medical interventions and technical prevention should be encouraged in the place where textile industry upgrades the local economic status such as Benin. Christiani et al.41 conducted a longitudinal study of 445 cotton workers over 11 years and found a decrease in forced expiratory volume 1 in individuals exposed to cotton dust. Moreover, respiratory functions decreased depending on the concentration and time of dust exposure in the workplace.42 The higher risks for women compared to men for asthma onset were robust, regardless of work exposure categories.43 Poultry farm workers are more prone to suffer from respiratory disorders due to higher concentrations of particulate matter in dust.44
Different from our results, a recent cohort study from Canada provided further evidence that living in a farming environment during childhood is protective of asthma incidence in adolescence and adulthood and supports the protective effect of the farm environment on asthma.45 Furthermore, farm exposure may have immunomodulatory effects by decreasing mDC proportions and asthma incidence as well.46 We think the difference in inclusion criteria may have been responsible for the discrepancy. We enrolled the studies aiming at adulthood and failed to get the positive results because exposure during childhood may be a protective factor, whereas prolonged exposure during adulthood did not influence the risk of asthma.
Considering the harm brought by organic dust, intervention programs aimed at reducing exposure to dust will ameliorate occupational working conditions and improve health conditions. The value of measuring organic dust content in occupational settings was emphasized to make differences in health effects for exposed workers.47 Another recent study48 proposed the extraction method using Tris/EDTA to more accurately assess the endotoxin content and pro-inflammatory potential.
In conclusion, our meta-analysis revealed an overall asthma susceptibility rate in excess of 48% among individuals exposed to organic dust compared with controls, especially for those exposed to paper/wood, flour/grain and textile dust.
 XML Download
XML Download