

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Asthma has a prevalence of 4.1%.1 The cost of asthma exceeds $8,800 per capita per year, and a recent investigation in Korea found that it costs affected patients more than $16,300 per year in work losses.2 The direct cost of asthma in severely affected patients is approximately 10-foldgreater than in those with mild asthma.34 Asthma requires significant medical resources, and as costs increase along with asthma severity, management of asthma is imperative.
Inhaled corticosteroids (ICSs) are critical in the treatment of asthma. ICSs are the first drugs of choice in the controller medication category recommended by the Global Initiative for Asthma (GINA) guidelines.5 ICSs improve lung function and quality of life, reducing asthma symptoms, disease progression, and related mortality.678 However, some drawbacks to ICS use have been reported; in particular, ICS use can increase the risk of pneumonia in patients with chronic obstructive pulmonary disease (COPD).9101112 Associations between ICS use and the risk of pneumonia have not been observed with all types of ICS. They have mainly been reported for fluticasone ICS, but not for budesonide.13 Studies also have not demonstrated that the increased risk of pneumonia is accompanied by increased mortality.14 Additionally, most studies of the relationship between ICS and increased pneumonia risk have been conducted on COPD patients, with fewer studies involving asthma patients, and the results of the studies remain controversial.1516 Some studies have reported that ICS use increases the risk of pneumonia in asthmatics,1617 while other studies have reported no association between ICS use and pneumonia.151819 Another suggested that ICS could act in a protective capacity against pneumonia.15 There is also very little data regarding ICS use and asthma in Korean patients. We evaluated whether the use of ICS increases the risk of pneumonia in asthmatic patients using data from the Asthma Management Adequacy Assessment performed by the Health Insurance Review and Assessment Service (HIRA) in Korea.
MATERIALS AND METHODS
Study design
Data from the Asthma Management Adequacy Assessment performed by the HIRA in Korea were analyzed. Asthma was the target disease, with disease codes J45.x and J46.x based on the Korean Standard Classification of Diseases version 6.0. Medical institutions were enrolled when primary to tertiary care institutions filed insurance claims for asthma (J45.x, J46.x) as a major disease code, or within the fifth minor disease codes, between July 2013 and June 2014. Claims data for medical care benefits for asthma (J45.x, J46.x) were analyzed, and study participants were the asthmatic patients on behalf of whom the claims were filed.
For the purpose of study participant selection, asthma was defined as follows: During the evaluation period, participants were aged 15 years or older with at least 2 outpatient visits, were treated with asthma medications or received inpatient care, and were using more than 1 systemic corticosteroid and at least 1 asthma medication at the time of the outpatient clinic visits. Asthma medications comprised ICS, long-acting β2-agonists (LABA), long-acting muscarinic antagonists (LAMA), short-acting muscarinic antagonists (SAMA), short-acting β2-agonists (SABA), leukotriene receptor antagonists (LTRA), and xanthine derivatives. This dataset also included age, sex, insurance type, hospital type, comorbidity and Charlson comorbidity index,20 outpatient or emergency department (ED) visit, hospitalization to the general or intensive care unit (ICU), and complications. ICS users and non-ICS users were defined as patients who were or were not prescribed ICS during the study period, respectively. Pneumonia occurrence was defined via the presence or absence of disease codes for pneumonia, which range from J12.x to J18.x. Types of health insurance were divided into 2 categories: medical insurance, a program that is eligible to all people in South Korea and is used by over 96.3% of the total population; or medical aid, a program in which the government pays on behalf of patients who are unable to pay their medical expenses. This study protocol was approved by the Institutional Review Board (IRB) of the Catholic University of Korea, Seoul St. Mary's Hospital (IRB No. KC16RESI0560).
Statistical analysis
All data were expressed as mean ± standard deviation, median value, or number (%). Continuous variables were analyzed by Student's t test or the Mann-Whitney U test, and categorical variables were analyzed by the χ2 test or Fisher's exact test. Multiple logistic regression analysis was used to determine if ICSs are an independent factor associated with pneumonia occurrence. Unadjusted or adjusted odds ratio (OR) and 95% confidence intervals (CIs) were presented. A P value of less than 0.05 was considered statistically significant. SAS ver. 9.2 (SAS Institute, Cary, NC, USA) was used for all statistical calculations and analyses.
RESULTS
Because we used data form Asthma Management Adequacy Assessment performed by the HIRA in Korea, the number of target organizations evaluated was limited to 16,804 sites, which accounted for 50.4% of a total of 33,341 sites. Forty-three sites were tertiary general hospitals (0.3%), 280 were secondary general hospitals (1.7%), and 14,745 were primary clinics (87.8%). The total number of asthma patients was 831,613, and among them, the number of patients using tertiary general hospitals was 43,471(5.2%), with 83,194 (10.0%) using secondary general hospitals, and 686,063 (82.5%) using primary care.
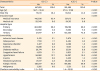
ICS users were older and more likely to be male than non-ICS users (P < 0.001). The proportions of ICS users who were medical aid patients and patients receiving care at secondary or tertiary hospitals were higher than those of non-ICS users (P < 0.001). All comorbidities, such as cardiovascular disease, diabetes mellitus, depressive disorder, allergic rhinitis, and malignancy, were more common in ICS users than in non-ICS users (P < 0.001), except for arthritis (Table 1). ICS users utilized more healthcare services: They visited outpatient clinics or EDs more often and were more frequently hospitalized to general wards or ICUs than non-ICS users (P < 0.001). The mean length of hospital stay was longer for ICS users than for non-ICS users, and the incidence of complications was higher in ICS users. Pneumonia, empyema, adult respiratory distress syndrome or acute respiratory failure, pneumothorax, and pneumomediastinum also occurred more often in ICS users than in non-ICS users (Table 2). ICS users received more prescriptions for respiratory drugs, including LABA, LAMA, LABA+LAMA, SAMA, SABA, SABA+SAMA, and LTRA as well as ICS and ICS+LABA, than non-ICS users. Conversely, the theophylline prescription rate was higher for non-ICS users than ICS users. LTRA and theophylline were most frequently prescribed in both groups (Table 3).
Table 1
Clinical characteristics according to inhaled corticosteroid use
![]()
Table 2
Asthma-related clinical characteristics according to inhaled corticosteroid use
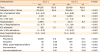
ICS, inhaled corticosteroids; ER, emergency room; ICU, intensive care unit; ARDS, acute respiratory distress syndrome.
![]()
Table 3
Prescribed respiratory medications according to inhaled corticosteroid use
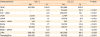
ICS, inhaled corticosteroids; LABA, long-acting β-agonists; LAMA, long-acting muscarinic antagonists; SAMA, short-acting muscarinic antagonists; SABA, short-acting β-agonists; LTRA, leukotriene receptor antagonist.
![]()
We selected among the previously analyzed factors to identify those associated with pneumonia. Asthma patients were divided into groups with pneumonia (pneumonia [+]) and without pneumonia (pneumonia [−]). The pneumonia (+) group was older and more likely to receive medical aid, utilized more secondary and tertiary hospitals, had a higher Charlson comorbidity index, had a higher hospitalization rate during the previous year, and had more ICS users than the pneumonia (−) group. In the univariate analyses, age, medical care, utilization of secondary and tertiary hospitals, Charlson comorbidity index, hospitalization due to asthma in the previous year, and ICS prescription were associated with an increased OR for pneumonia occurrence. Multiple logistic regression analysis showed that ICS prescription was associated with pneumonia (OR, 1.38; 95% CI, 1.36–1.41). In addition to ICS prescription, age, sex (female), medical care, use of secondary and tertiary hospitals, and hospitalization due to asthma in the previous year were all associated with pneumonia (Table 4).
Table 4
Risk factors for pneumonia in asthmatic patients
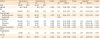
OR, odds ratio; CI, confidence interval; ICS, inhaled corticosteroids.
*Adjusted factors: age, sex, insurance type, hospital type, Charlson comorbidity index, hospitalization, and ICS use.
![]()
DISCUSSION
We found that ICS use was associated with pneumonia in our asthmatic patients even after adjusting for age, hospital type, comorbidity index, and medical use. ICS users were older, had more comorbidities, and had more medical use and respiratory medicine prescriptions than non-ICS users. They were more likely to be on medical aid and use secondary and tertiary hospitals. Pneumonia and other pulmonary complications were more common among ICS users. However, the high incidence of pneumonia in ICS users might be due to old age and severe disease status.
A previous study showed that chronic bronchitis, asthma, smoking, and ICS are all risk factors for community-acquired pneumonia (CAP) in the general population.21 Additional studies revealed that the use of ICS in asthmatic patients increased the risk of pneumonia and that the risk increased as the ICS dose increased; this association was most pronounced in patients receiving fluticasone propionate.22 In a Korean study, ICS use increased the risk of hospitalization or ED visits due to pneumonia. Conversely, the use of ICS + LABA reduced this risk, suggesting a protective effect against pneumonia.16
Many studies have shown that risk factors for pneumonia include age and chronic lung diseases such as COPD or asthma.212324252627 In a meta-analysis of patients with COPD, the risk factors for pneumonia were old age and low FEV1 (%).13 This suggests that increased pneumonia risk in patients with chronic lung diseases may be due to factors other than ICS, such as age and baseline lung function.
Several recent studies have suggested that ICS use may increase pneumonia risk in COPD patients.910111228 However, studies exploring the association of ICS with pneumonia in asthmatic patients are scarce. In one study, smoking and ICS use were risk factors for pneumonia in patients with COPD, but ICS was not associated with pneumonia in asthmatic patients. Use of inhaled anticholinergics is a risk factor for pneumonia in asthmatics18; however, in this study, anticholinergics referred only to ipratropium and may not be applicable to LAMA. In our study, the frequency of LAMA, LABA, and LTRA prescription was also significantly higher in ICS users than non-ICS users. Effects of LAMA, LABA, and LTRA on pneumonia risk cannot be ruled out and could confound an assertion of increased pneumonia risk solely associated with ICS. Nonetheless, another study, in COPD patients, showed that the risk of pneumonia in the LAMA use group was lower than in the ICS group and the LABA combined group,17 and that while the use of ICS without LABA increased the risk of pneumonia, patients using ICS with LABA had a lower risk of pneumonia among patients using ICS.16 As a result, although it is difficult to completely rule out the effects of LAMA, LABA, and LTRA, it is reasonable to assume that the increased risk of pneumonia in the ICS group is likely to be more strongly influenced by ICS than by other medications.
Two other studies have also shown that the use of ICS in asthmatic patients has no effect on CAP,15, 19 and a third reported that ICS use reduced pneumonia in children with asthma.29 Other studies also demonstrate contradictory results from ours. In a retrospective study of pooled randomized trials focusing on budesonide use, inhaled budesonide did not increase pneumonia risk compared to non-ICS treatment and, conversely, it seemed to protect against pneumonia. Further, no difference in pneumonia incidence between the budesonide low-dose and high-dose treatment groups or between the budesonide and fluticasone ICS treatment groups was observed.15 Of note, however, this study only examined data from trials sponsored by the pharmaceutical company AstraZeneca, so bias with regard to budesonide cannot be ruled out.
ICS may mitigate risk factors for pneumonia by reducing airway inflammation, improving asthma control, and reducing atelectasis due to mucus impaction, which can be misdiagnosed as pneumonia. Low FEV1 is also a risk factor for pneumonia in and of itself. One report suggested that pneumonia incidence is lower in asthmatic patients than in COPD patients because FEV1 values were higher in the asthmatic patients enrolled in that study than in the COPD patient populations enrolled in conventional studies.15 These findings are similar to those of a meta-analysis showing that the use of inhaled budesonide in COPD patients did not increase the risk of pneumonia.13 In most studies reporting an increased pneumonia risk with ICS use, the ICS was fluticasone.30 An indirect and comparative meta-analysis showed that budesonide/formoterol users had a lower pneumonia risk than fluticasone/salmeterol users, and indicated that difference in ICS type might contribute to differences in pneumonia risk.31
ICS-mediated pneumonia in COPD patients is thought to stem from ICS-related damage to the host mucosal defense system, as bacteria have been found colonizing the lower respiratory tract in 25% of COPD patients,32 suggesting that bacterial pneumonia may coincide somewhat with ICS use.15 In the case of asthma, opposing results have been observed; reportedly, the use of ICS reduced bacterial load and invasion,33343536 and was not shown to increase bacterial infection.37 In contrast, other studies have reported that ICS use reactivates chronic bacterial infection and induces bacterial colonization.383940 As such, the mechanistic relationship between ICS and pneumonia remains unclear. However, the risk of nontuberculous mycobacterial infection does increase when patients with chronic respiratory diseases use ICS,4142 and the airway microbiota is altered in ICS users compared to normal controls,43 offering the possibility that ICS could affect airway microbiota and thereby encourage the development of pneumonia. Although several studies have shown that the use of ICS in COPD patients increases pneumonia risk, it does not increase mortality or protect from death.911124445 ICS has even been reported to reduce the severity of pneumonia by decreasing airway inflammation, further confounding a definitive conclusion.
It may seem unusual that, in this study, the proportion of asthma patients using ICS was less than 50%. However, other studies have shown the ICS prescription rate for asthma patients to be only 20% to 30%, and lower still for those treated at primary care institutions,46474849 suggesting it is unlikely that the inhaler prescription rate in this study was abnormally low.
There are some limitations to our study that must be acknowledged. The cross-sectional study design made it difficult to support a causal relationship empirically. Because Asthma Management Adequacy Assessment data by the HIRA are limited to 1 year, it cannot be known how long the patients had been using ICS, nor was there information about whether ICS were started before or after pneumonia development. A prospectively designed study is warranted to evaluate the causal relationship between ICS and pneumonia in more depth. The definitions of asthma and pneumonia used in this study may not represent actual diagnosis, because pulmonary or imaging tests were not directly confirmed, and it is thereby possible that the control group included those with mild illnesses other than asthma, such as allergic rhinitis or chronic cough. These factors may have influenced the results by further reducing the risk of pneumonia in the control group, and these limitations also apply to the drug data. Also, there might be a discrepancy between drug prescription and actual drug use or compliance with the prescription. We could only identify the type of drug, but not the dose or generic prescription name, so assessments of the dose-response relationship between ICS use and pneumonia or differences in pneumonia risk according to specific ICS in use (fluticasone, budesonide, or beclomethasone) were precluded. Although statistically adjusted for other factors, the study results may have been confounded by disease severity. As asthma severity itself has been demonstrated as a risk factor for pneumonia in previous studies,2550 bias could be decreased in future studies by calibrating or measuring severity-related markers. Most importantly, the lack of information on patient smoking history and pulmonary function and the fact that the COPD disease code was not excluded from this study limit the appreciation of an asthma-COPD overlap, wherein COPD cannot be completely distinguished from asthma. In addition, it is possible that ICS/LABA might be prescribed without a pulmonary function test to confirm the diagnosis of asthma in the Korean National Health Insurance system. Specifically, it is possible that a claim for asthma was entered for the ICS prescription even if the patient was suspected of having COPD. Balancing these limitations, there was little possibility of selection bias because our study utilized a nationwide insurance assessment database. We also had the advantage of knowing that the asthma-related indicators in one country at a time.
Despite continued controversy regarding ICS use and pneumonia incidence, we found evidence to support the idea that ICS use might be associated with increased pneumonia in asthmatic patients in Korea. Therefore, it is important to acknowledge that ICS use in asthmatic patients may increase the risk of pneumonia and should be followed up for preventative purposes.
 XML Download
XML Download