

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
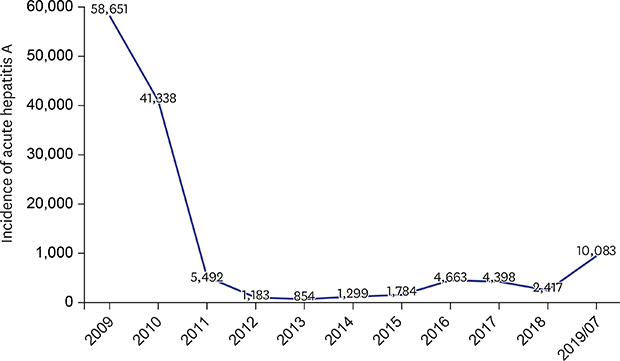
The number of patients with acute hepatitis A is increasing sharply in Korea. A total of 10,083 confirmed cases were reported for seven months in 2019 according to the Korean Centers for Disease Control and Prevention (KCDC) (Table 1).1 Although the government data testify the seriousness of the situation, we still have little indication of the possible cause of this abrupt epidemic. In fact, the number of annual reported cases of acute hepatitis A rapidly increased in the 2000s with a peak of 15,231 cases recorded in 2009.1 After the outbreak in 2009, the number of cases gradually decreased to a low of 867 cases in 2013. However, reported cases gradually increased from 2013 to 2016 with a maximum of 4,679 cases, followed by a subsequent decrease to 2,437 cases in 2018. The current resurgence may be attributed to the proportion of susceptible subjects in the Korean population, as about 10 years have passed since herd immunity was induced by the epidemic occurring during the late 2000s.
Table 1
Age-related incidence of acute hepatitis A according to KCDC
KCDC = Korean Centers for Disease Control and Prevention.
aAccording to National Health Insurance Service data.
![]()
TRENDS OF SEROPREVALENCE OF HEPATITIS A
A previous study reported the nationwide rate of seropositivity for anti-hepatitis A virus antibodies (anti-HAV) based on data from the Health Insurance Review and Assessment Service of Korea from 2005 to 2014.2 The age-adjusted, anti-HAV prevalence showed a gradual decrease from 65.6% in 2005 to 62.2% in 2014. Moreover, individuals in their 20s showed the lowest positivity for anti-HAV, which has not changed remarkably during the last 10 years. However, those in their 30s continuously decreased from 69.6% in 2005 to 32.4% in 2014, and positivity for anti-HAV in individuals in their 40s decreased more slowly from 97.9% to 79.3% during the 10-year period. In other words, the seroprevalence of hepatitis A has been changing in Koreans under 50 years of age, with persons aged 20 to 39 the most vulnerable to HAV infection. As shown in the previous study, the majority of young adults who have not yet experienced HAV infection and who did not receive a vaccination are still vulnerable to hepatitis A.3 This year's epidemic of acute hepatitis A could be the expected outcome of a vulnerable population. Effective acute hepatitis A control and prevention strategies for young adults, especially those in their 20s and 30s are necessary.
CLINICAL FEATURES AND SOCIAL BURDEN OF ACUTE HEPATITIS A
Acute hepatitis A is an infectious disease caused by the HAV, which is transmitted by the fecal-to-oral route, and a one-time infection can provide lifelong immunity.4 Although the distribution of hepatitis A is variable according to geographical region and population group, the epidemiology of hepatitis A is thoroughly related to socioeconomic factors, including density of housing, sanitation, poor hygiene, water quality, and income. Overall improvements of hygiene worldwide are leading to a shift of susceptibility to infection from early age to young and older adults.5 The disease typically presents as a mild disease with no overt clinical features in children, but the severity of the disease increases with age. It tends to show more severe symptoms, such as fulminant hepatitis, in the elderly and patients with underlying liver diseases. In the literature, 70% of adults infected with HAV develop symptoms, but less than 1% develop fulminant hepatitis.6 The rate of fulminant hepatitis due to acute hepatitis A in Korea is estimated to range from 0.67% to 1.4%.7,8 Overall, mortality due to fulminant hepatitis is rare. According to Chinese outbreak data, there were 47 deaths among > 300,000 infected patients.9 However, most of those infected in this outbreak were relatively young and healthy adults. The estimated case-mortality ratio of acute hepatitis A differs with age and ranges from 0.1% among children < 15 years of age to 0.3% among persons 15–39 years of age. In age groups > 50 years, it rises to 1.8%–5.4%. Fulminant hepatitis is rare but associated with mortality, especially when liver transplantation is not possible.
According to recent epidemiological data of patients diagnosed with acute hepatitis A from 2009 to 2013 in Korea, the hospital admission rate because of acute hepatitis A was highest in the 30–39 year age group, with 17,138 cases (42.5 cases; 100,000 of the population per year), and lowest in the 50–59 year age group, with 1,691 cases (4.3 cases; 100,000 of the population per year).10 The medical cost for admitted patients is 1,221,159 won, which is approximately 10 times more expensive than treatment of patients in outpatient clinics. Additionally, the total medical cost for acute hepatitis A increases because individuals in their 20s and 30s belong to the most active group in the workplace. The disease can lead to significant economic and social consequences as it can take weeks or months for patients recovering from the illness to return to work, school, or daily life.
STRATEGIES AND PREVENTION FOR ACUTE HEPATITIS A
First, protection against HAV infection is afforded by adequate sanitation. Suitable sanitation to prevent fecal-oral transmission through food, water or person-to-person contact is important for controlling the transmission of hepatitis A.
Next, acute hepatitis A is a vaccine-preventable disease. Administered as an intramuscular injection in a 2-dose series with the second dose 6–18 months after the first, the hepatitis A vaccine induces protective antibody levels in virtually all adults. One month after the first dose, 94%–100% of adults have protective antibody levels; and after a second dose, 100% achieve protective levels.11 The KCDC designated HAV infection as a national notifiable infectious disease and, for effective control, added hepatitis A to the national vaccination program for children beginning in May 2015. However, adolescents aged older than 12 years did not benefit. The seroprevalence rate of people aged 20–24 years is only 11%–18%. Fortunately, a routine medical checkup sponsored by the Ministry of Education is now available upon entrance to high school. The test for anti-HAV antibodies can be included in the checkup, and it can be determined if school-aged students require a vaccination.12 However, a national telephone survey of 800 mothers with children aged 7–18 years reported that only 68.4% of the parents were willing to vaccinate their children against HAV at the current cost (100,000 KRW for two shots), but 91.8% reported that they would vaccinate their child if the HAV vaccination cost less than half of the current price (40,000 KRW).13 Therefore, reducing the cost would considerably improve the vaccination rate in school-aged students.
Finally, until a decade ago, immunoglobulin G (IG) was the only recommended post-exposure prophylaxis against HAV. The effective post-exposure prophylaxis of HAV infection with inactivated HAV vaccines when administered > 2 weeks after exposure along with the high cost of IG and the short-term protection afforded through passive immunization, has led to the declined use of IG.14
 XML Download
XML Download