

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
With advances in preterm neonatal care, the overall survival rate has been improved for even extremely preterm infants at the threshold of viability and late preterm infants with life-threatening congenital anomalies or inborn error of metabolism. However, the incidence of neonatal complications has remained stagnant for decades because intentions to actively treat more high-risk infants,12 and the demand and actual use of renal replacement therapy (RRT) is increasing in preterm neonates.345 However, peritoneal dialysis, the most commonly used RRT in the neonatal intensive care unit (NICU), is less efficient than hemodialysis or continuous RRT (CRRT) with regard to the removal of free water and ammonia.6 Infants who have undergone an abdominal surgery recently, many of whom might require RRT, are limited to peritoneal dialysis.7 CRRT, on the contrary, can achieve continuous ultrafiltration and solute clearance with less hemodynamic changes. CRRT is also known to be useful for the removal of inflammatory mediators, including proinflammatory cytokines, chemokines, and complements.89 However, only few reports have been published on the use of CRRT in the NICU,10111213 none of which thoroughly investigated the application and outcomes of CRRT exclusively for preterm infants. The purpose of this study was thus to evaluate the clinical characteristics and prognostic factors that affect mortality after CRRT in preterm infants born at a gestational age ≤36 weeks.
MATERIALS AND METHODS
This study was approved by the Institutional Review Board of Samsung Medical Center (SMC), which waived the requirements for informed consent for this retrospective chart review (IRB No. SMC 2018-08-031).
Patient population and data collection
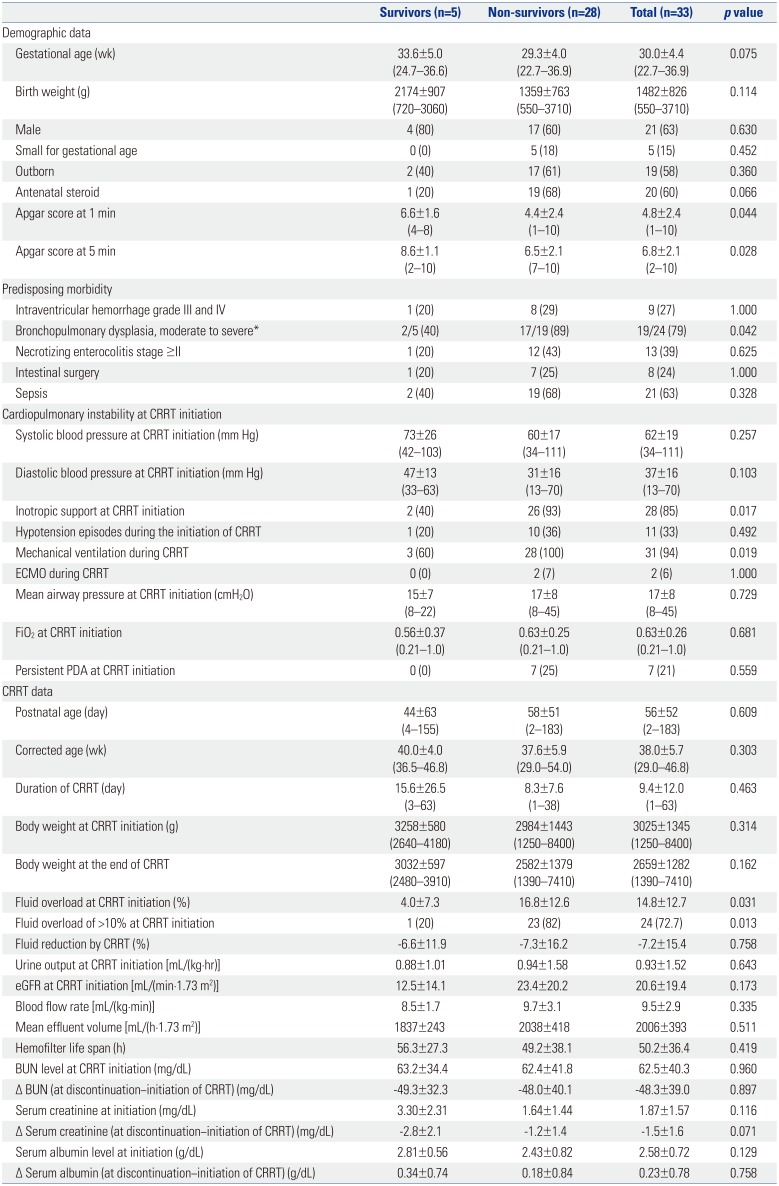
The medical records of 33 preterm infants who received CRRT at the SMC NICU between January 2008 and December 2017 were retrospectively reviewed. To investigate the clinical characteristics and risk factors of mortality after CRRT, data on demographics, predisposing morbidity, cardiopulmonary instability, and CRRT were collected and compared between the survivors and non-survivors (Table 1). The demographic data included gestational age, birth weight, sex, small-for-gestational age status, outborn status, antenatal steroid use, and Apgar scores at 1 and 5 minutes. Data on the predisposing morbidities included intraventricular hemorrhage grades III and IV, moderate to severe bronchopulmonary dysplasia, necrotizing enterocolitis stage ≥2, intestinal surgery, and blood culture-proven sepsis prior to CRRT. The CRRT data included postnatal and corrected age at CRRT initiation, CRRT duration, body weight at initiation and end of CRRT, degree of fluid overload at CRRT initiation, urine output and estimated glomerular filtration rate (eGFR) at CRRT initiation, mean effluent volume, and hemofilter life span. The laboratory measurements included serum blood urea nitrogen (BUN), creatinine, and albumin levels prior to and after the use of CRRT. The eGFR was calculated using the Schwartz equation.14 A weight-based method for percentage fluid overloading (FO) was defined as follows: % FO={[Body weight at CRRT initiation (in kg)−Ideal body weight (in kg)]/[Ideal body weight (in kg)]}×100%. Fluid reduction by CRRT was defined as follows: % Fluid reduction={[FO at CRRT initiation-FO at end of CRRT]/[FO at CRRT initiation]}×100%. Indications for CRRT were also reviewed and compared between the survivors and the non-survivors (Table 2).
Application of CRRT in the NICU
Continuous venovenous hemodiafiltration was performed as a CRRT modality using a PRISMA machine with a M10 hemofilter (Gambro Healthcare, Lakewood, CO, USA) from January 2007 to September 2010 and a PRISMAflex machine with a polyacrylonite hollow-fiber hemofilter (HF20; Gambro Healthcare, Lakewood, CO, USA) since October 2010. Commercially produced bicarbonate-buffered hemofiltration replacement solutions (Hemosol B0; Gambro Korea, Seoul, Korea) was used as the dialysate and replacement fluid. Vascular access was enabled with a double-lumen catheter (diameter 6.5-Fr; Gambro Healthcare) inserted into the internal jugular vein. All patients underwent insertion of the internal jugular vein catheter by a percutaneous puncture or cut-down method by a pediatric surgeon under general anesthesia in the NICU. Priming of the extracorporeal circuit was performed with red blood cells diluted with 0.9% saline to achieve a hematocrit of 30 to 40%.
Continuous RRT was initiated without anticoagulation. However, anticoagulation was subsequently started when the hemofilter life span was shortened within 24 hours. Unfractionated heparin was used as an anticoagulant with an initial bolus of 20 units/kg, followed by an initial continuous infusion rate of 10 units/kg/hr. The infusion rate was adjusted targeting the activated clotting time of 170 to 210 seconds. Close collaboration among neonatologists, pediatric nephrologists, and pediatric surgeons was maintained during the CRRT.
Statistical analyses
Data are expressed as a mean±standard deviation or as a number (percentage). Categorical variables were compared using the chi-square or Fisher exact test, and comparisons between continuous variables were evaluated using the Mann-Whitney U test. A p value of <0.05 was considered statistically significant. Binary logistic regression was used for univariable analysis to calculate the odds ratios (ORs) with 95% confidence intervals (CIs) of clinical covariates for mortality after CRRT (Table 3). Finally, for multivariable analysis, stepwise backward elimination was performed to calculate the adjusted OR for mortality for covariates selected as variables with p values <0.1 in the univariable analysis. However, because most of the patients (31/33) had ventilator dependency at CRRT initiation, mechanical ventilation was not included in the multivariable analysis. All analyses were performed using STATA 14.0 (StataCorp LP, College Station, TX, USA).
RESULTS
Patient characteristics
A total of 33 preterm infants were included in this study, of whom five survived and 28 died. Comparison of baseline characteristics between the survivors and the non-survivors is shown in Table 1. The mean gestational age at birth and birth weight were 30.0±4.4 weeks (range, 22.7–36.9 weeks) and 1482±826 g (range, 550–3710 g), respectively. No significant differences were found between the survivors and the non-survivors in terms of gestational age, birth weight, proportions of the sexes, small-for-gestational age status, and outborn status. However, the non-survivors showed lower use of antenatal steroid and lower Apgar scores at 1 and 5 minutes than the survivors. With regard to predisposing morbidity, no significant difference was observed between the survivors and the non-survivors. Most infants showed cardiopulmonary instability at CRRT initiation; 28 infants required inotropic support; and 31 infants required mechanical ventilation. However, the rate of inotropic use was significantly higher in the non-survivors than in the survivors (93% vs. 40%, p=0.017).
We found no significant differences in mean postnatal age and body weight at CRRT initiation between the survivors and the non-survivors. However, fluid overload at CRRT initiation was significantly higher in the non-survivors than in the survivors (16.8% vs. 4.0%, p=0.031). The incidence of fluid overload >10% at CRRT initiation was significantly higher in the non-survivors than in the survivors (82% vs. 20%, p=0.013). No significant differences in the reduction of free water and solutes, such as BUN and creatinine, were found between the survivors and the non-survivors.
Indications for CRRT in preterm infants
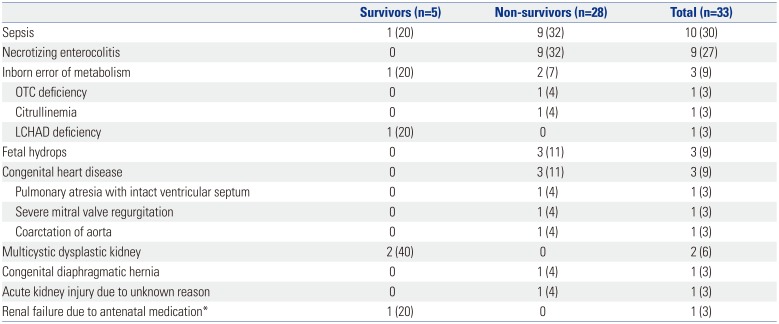
Table 2 shows the indications for CRRT. The most frequent indication for CRRT was severe systemic inflammatory response after sepsis or necrotizing enterocolitis (n=19); however, only one of these infants survived. Among three infants with inborn error of metabolism, one infant with long-chain 3-hydroxyacyl-CoA dehydrogenase deficiency survived. Two infants who received CRRT due to multicystic dysplastic kidney all survived. The other survivor received CRRT due to maternal medication of angiotensin-converting enzyme inhibitor during pregnancy. The latter patient progressed to end-stage renal disease during follow up at the outpatient clinic, while the remaining survivors are being followed up without renal dysfunction.
Univariable and multivariable analyses
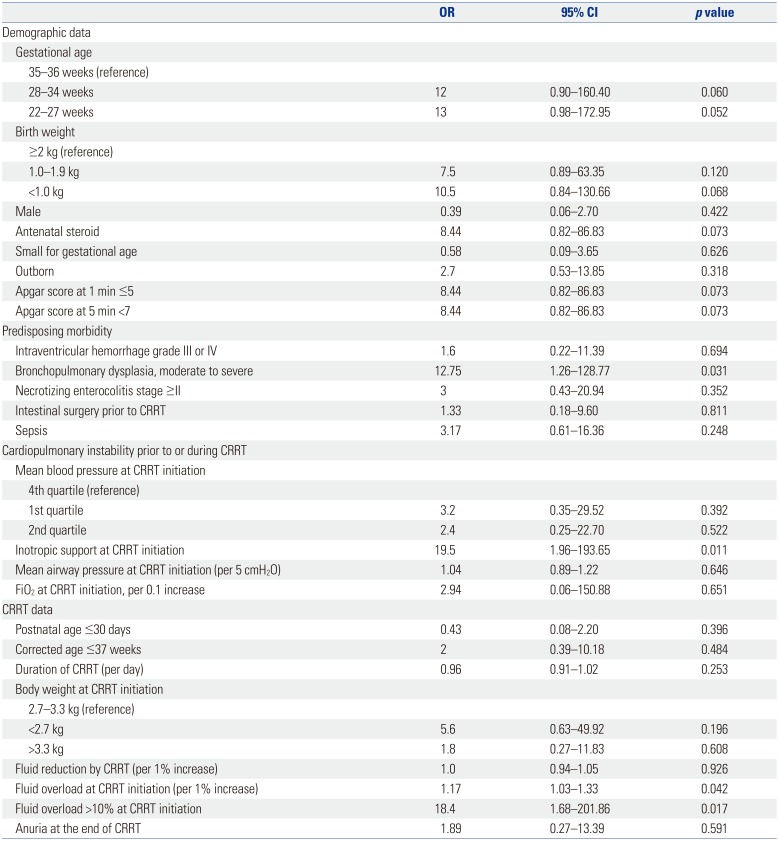
Table 3 shows the results of the univariable analysis for mortality after CRRT in the preterm infants. The presence of bronchopulmonary dysplasia, inotropic support at CRRT initiation, and fluid overload was associated with mortality after CRRT. The variables with p values <0.1 were selected for further multivariable analysis and included gestational age, antenatal steroid use, Apgar score of <7 at 5 minutes, inotropic support at CRRT initiation, and fluid overload >10% at CRRT initiation. Birth weight was not selected for further analysis because of collinearity with gestational age, nor was bronchopulmonary dysplasia because many patients died before the corrected age of 36 weeks. Finally, the multivariable analysis revealed that fluid overload >10% was associated with mortality (adjusted OR, 14.6; 95% CI, 1.10–211.29, p=0.049), while the other variables, including gestational age, Apgar score of <7 at 5 minutes, and inotropic use, were eliminated by stepwise backward elimination.
Fate of CRRT in preterm infants
The non-survivors died within 1 month of CRRT discontinuation (median 10.5 days, minimum 0 days, maximum 31 days) due to the progression of the underlying morbidity with comorbid renal dysfunction. The five survivors have remained under follow up at the outpatient clinic after being discharged, three of whom have good renal function but are undergoing rehabilitation due to developmental delay, and two who are on peritoneal dialysis due to progression to end-stage renal disease.
DISCUSSION
We evaluated the clinical characteristics and prognostic factors of survival in preterm infants who received CRRT in the NICU. For the preterm infants with azotemia, CRRT achieved high efficacy in lowering the serum BUN and creatinine levels, attaining mean reductions of 74.8% and 75.3% within 1 week, respectively. Fluid reduction was also achieved, with a 7.2% mean reduction in total body water. Our data, apart from the findings on survival after CRRT, showed that CRRT in preterm neonates with mean and minimum body weights of 3 and 1.25 kg, respectively, at CRRT initiation was feasible for fluid and solute reduction. Although the survival rate of 15% is grave, the demand for CRRT in preterm infants is expected to increase. Improvement of the CRRT technique with an appropriate machine for smaller infants and better understanding of CRRT for infants with immature organ function are urgent needs.8 In this regard, a new CRRT machine designed for term and preterm infants with smaller priming volume and an accurate handling system of very low blood and ultrafiltration flow has been developed in Italy and is under clinical trial in Europe.15 When the conventional machine for pediatric patients is used, special care for cardiopulmonary stabilization is needed for preterm infants undergoing CRRT with larger extracorporeal blood volumes and higher blood flow rates relative to their total blood volumes. The risk of catheter-related complications due to a relatively larger catheter size and higher blood flow rates, compared to their body size, may also be problems that need addressing. In our data, catheter-related complications occurred in four patients, including catheter-site bleeding (n=1) and occlusion (n=3).
Our results suggest that the prognosis of premature infants after CRRT depends on the degree of fluid overload at CRRT initiation rather than the degree of azotemia, premorbid renal function, or how much free water or solute was removed by CRRT. Accumulated fluids subsequently and rapidly aggravate cardiopulmonary function, which leads to renal dysfunction. Preterm infants are prone to fluid accumulation owing to the decreased free water clearance of the developing kidney, the dominance of antidiuretic hormones over natriuretic hormones, or comorbid conditions, including acute kidney injury, persistently patent ductus arteriosus, or septic shock.16171819 We speculate that the reason for the poor prognosis after CRRT is as follows: premature infants progress to multiorgan dysfunction rapidly once fluid overload and hemodynamic instability are aggravated to reach decompensation; therefore, prognosis cannot improve in most cases, even after successful removal of free water with CRRT. In previous studies, fluid overload was calculated using the difference between the daily input and the output volume or the weight difference.1820 For neonates, use of the weight difference is preferred because of high insensible water loss.21 However, especially for premature neonates, subtracting the estimated body weight from the increased body weight is more desirable than subtracting the body weight at admission because of the rapid daily weight gain in preterm infants and long hospital stay before CRRT (mean of 56 days in this study). If the fluid overload is not defined in consideration of the ideal lean body weight gain in premature infants, the degree of fluid overload may be overestimated, although other studies to date have not considered this. Nevertheless, previous studies by Askenazi, et al.22 and Sutherland, et al.20 reported that fluid overload >20% increased the risk of mortality in pediatric patients. In this study, fluid overload >10% was sufficient to lead to mortality in premature infants with severe infection, systemic inflammation, metabolic disorder, or life-threatening congenital anomalies.
In the present study, gestational age and body weights at birth were significantly lower in the non-survival group than in the survival group, whereas no significant difference was found between the groups in terms of corrected age, postnatal age, or body weight at the time of starting CRRT, which probably suggests that the impact of the degree of prematurity at birth on survival is greater than that of postnatal growth at the time of CRRT initiation. Likewise, the impact of low Apgar scores on survival was sustained until the time of CRRT. On the contrary, antenatal steroid use was higher in the non-survival group than in the survival group. This probably suggests that the non-survivors were more premature in terms of gestational age than the survivors, such that antenatal steroids were more frequently indicated in non-survivors, rather than suggesting a detrimental effect for antenatal steroids. On the other hand, preexisting morbidities, especially bronchopulmonary dysplasia, were associated with mortality in the preterm infants with CRRT. Other morbidities were also observed more frequently in the non-survival group than in the survival group, although this trend did not reach statistical significance. Taken together, along with the low quality of perinatal and respiratory care, more premature infants in terms of gestational age, birth weight, or fetal lung development were at higher risk of mortality after CRRT than the less premature infants.
Cardiopulmonary function at CRRT initiation was also instrumental: the non-survival group had more inotropic and mechanical ventilator support. Santiago et al. reported that hypotension associated with CRRT was detected in 30.4% of children.23 In our study, 85% of the infants underwent hemodynamic instability requiring inotropics at the initiation of and/or during CRRT and 33% of the infants experienced abrupt hypotension episodes during the beginning of CRRT, which remained a challenge in preterm infants with larger extracorporeal volumes and higher blood flow rates relative to the total blood volume.
The use of CRRT in the NICU has been reported in a few studies, and even fewer studies have provided data for preterm cases. The study population of the prospective pediatric CRRT registry in the United States included children weighing ≤10 kg (median, 4.4 kg) and showed a survival rate of 43%.22 Diane Mok, et al.24 reported a survival rate of 42% in term and preterm neonates during NICU hospitalization. The smallest neonate in their study weighed 1.9 kg at CRRT initiation.24 In this study, we provide additional data on CRRT performed in the NICU for which the survival rate was 15%, and the study population exclusively included preterm infants with a minimum body weight of 720 g at birth and 1.25 kg at CRRT initiation. Though not reported, application of CRRT for preterm infants is not a rare practice in some NICUs; therefore, more research is needed to improve the outcomes thereof. The limitations of this study included the retrospective nature of the study design, small sample size, and a heterogenous study population ranging from extremely preterm infants with severe infection to late preterm infants with life-threatening congenital anomalies. The relatively large extracorporeal circuit volume and hemofilter might have compromised outcomes. The limitation of this study in relation to statistical analysis was the concern for overfitting in the multivariable analysis due to the relatively large number of variables included in the analysis relative to the small number of patients. Further studies with larger sample sizes are needed to overcome this bias. In addition, considering that only survivors would have been referred to the NICU, there might be a selection bias in our results.
In conclusion, only 15% of the preterm infants who received CRRT in the NICU survived. Fluid overload >10% prior to CRRT initiation was independently associated with mortality after CRRT. Our data suggest that earlier initiation of CRRT before severe fluid overload, together with special care for premature multiorgan function, may help improve survival in high-risk preterm infants. Owing to the increasing demand for CRRT in preterm infants, future research with a larger sample size is urgently needed to improve outcomes.
 XML Download
XML Download