

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Lung cancer is the leading cause of cancer-related mortality worldwide, developing in more than one million new patients annually. Small cell lung cancer (SCLC), accounting for about 15% of lung cancers,1 is the most aggressive subtype, with a 2-year survival rate in less than 15% of cases. It is well-characterized to have high sensitivity to first-line, platinum-based chemotherapy; rapid emergence of resistance; and rapid progression, culminating in patient death.2 Although topotecan has been approved for relapsed SCLC, since its efficacy was demonstrated in a phase III trial in patients who progressed after platinum doublet chemotherapy, the survival benefit was only modest.3 Hence, there is a clearly an unmet need for new therapeutic options for this highly lethal malignancy.
Sonic hedgehog (Shh) signaling pathway regulates cell growth and differentiation during embryonic tissue patterning, and it may also play a role in maintenance of stem cell compartments in adults.4 An association between Shh signaling and human cancer was first identified by the mapping and cloning of patched as the gene responsible for heritable basal cell nevus syndrome (Gorlin syndrome).56 After that, visdemogib, an orally active small molecule targeting Shh pathway, has demonstrated efficacy in treatment of Gorlin syndrome7 and sporadic basal cell carcinoma. In recent years, several studies have shown involvement of Shh signaling pathway in the development and progression of numerous sporadic cancers, including basal cell carcinoma,4 medulloblastoma,8 prostate cancer,910 pancreatic cancer,11 cancers of the gastrointestinal tract,12 and SCLC.13 Furthermore, it has been shown that Shh pathway is also associated with resistance to platinum-based chemotherapy in non-small cell lung cancer (NSCLC).14 Moreover, it has been suggested that activation of Shh signaling pathway is associated with poor prognosis in patients with a number of malignancies, including head and neck cancer,15 human glioma,16 bladder cancer,17 and NSCLC.18 To date, little is known on the relationship between Shh signaling pathway and prognosis in patients diagnosed with SCLC. Hence, based on previous studies, we investigated the value of components of Shh pathway as prognostic markers in extensive stage small cell lung cancer (ES-SCLC) patients.
Go to : 
MATERIALS AND METHODS
Patients and data collection
We retrospectively analyzed data from 36 patients who were participating in a phase II trial of belotecan plus cisplatin for newly diagnosed ES-SCLC between 2008 and 2012 at a single center in Korea.19 Key eligibility requirements of the trial were as follows: 1) histologically confirmed ES-SCLC, 2) age between 18–75 years, 3) no previous history of chemotherapy or radiotherapy, 4) at least one measurable disease according to the Response Evaluation Criteria in Solid Tumors (RECIST) version 1.0 (https://academic.oup.com/jnci/article/92/3/205/2965042), 5) an Eastern Cooperative Oncology Group (ECOG) performance status (PS) of 0 to 2, 6) life expectancy of at least three months, and 7) adequate organ and marrow function.
Out of 42 patients participating in the trial, samples from 36 patients were available for the analysis, and we retrospectively reviewed their clinical information using medical records. Clinico-pathological information on sex, age at diagnosis, disease status, extensiveness of disease, metastatic organ, first-line and second-line chemotherapy regimens, and treatment duration were reviewed and documented. The overall response to treatment was evaluated using the Response Evaluation Criteria in Solid Tumor (RECIST) 1.0. This study was approved by institutional review board of Wonju Severance Christian Hospital (IRB number: 2019-02-0013), and conducted according to declaration of Helsinki.
Immuno-histochemical analysis
For the 36 patients with available tumor tissue, 4-um-thick tissue sections were de-paraffinized, rehydrated, and washed two times in buffer. To reduce nonspecific background staining due to endogenous peroxidase, the slides were incubated in Hydrogen Peroxide Block for 10 minutes and washed four times in buffer. The primary antibodies Gli1 (1:50, Santa Cruz; Santa Cruz, CA, USA), Ptch-1 (1:50, Santa Cruz), Smo (1:50, Santa Cruz), and Shh (1:50, Santa Cruz) were applied and incubated according to the manufacturers' recommended protocols; then, the slides were washed four times in buffer. The slides were then stained with Primary Antibody Enhancer (Thermo Fisher Scientific Anatomical Pathology, Runcorn, UK), incubated for 20 minutes at room temperature, and then washed four times in buffer. Afterward, HRP Polymer (Thermo Fisher Scientific Anatomical Pathology) was applied to the slides, and slides were incubated for 30 minutes at room temperature and washed four times in buffer. Slides were then incubated with hematoxylin for chromogen, washed four times in deionized water, and counterstained.
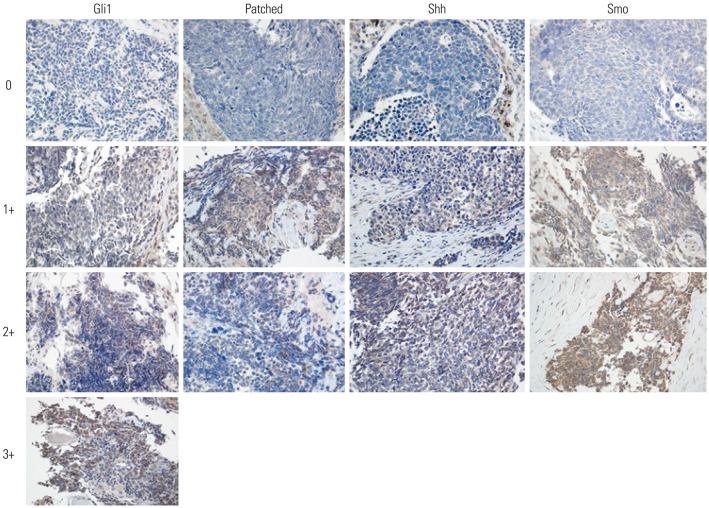
Immunohistochemistry (IHC) intensity staining was scored as 0 (negative), 1 (weak), 2 (moderate), or 3 (strong) (Fig. 1). The percentage of positive cells (percentage scores) was graded as 0 (0%), 1 (1–25%), 2 (25–50%), 3 (50–75%), or 4 (75–100%). The overall IHC score was calculated by multiplying the intensity score by the percentage score. Any IHC score >6 was defined as over-expression.
Statistical analysis
Fisher's exact test was used to evaluate the association between protein expression and clinical parameters. Overall survival (OS) was calculated as the date of initiation of first-line chemotherapy to death from any cause. Progression free survival (PFS) was defined as the time from initiation of first-line chemotherapy to progression or death, whichever occurred first.
Kaplan-Meier curves were used to plot PFS or OS cures, and the differences in survival time were analyzed using log-rank tests. Multivariate analysis was performed using Cox proportional hazards model to determine the significance of relationships between variables and survival. p values less than 0.05 were considered significant. All analyses were performed with SPSS version 18.0 (SPSS Inc., Chicago, IL, USA).
Go to :
RESULTS
Patient characteristics and expression stats of proteins related to Shh pathway
Baseline characteristics of study patients are described in Table 1. The median age was 65 years (range, 49–75 years), with 32 male (88.9%) and four female (11.1%) patients. The majority of patients (91.7%) had an ECOG PS of 0 or 1. All 36 patients were diagnosed with ES-SCLC and treated with platinum-based doublet chemotherapy (belotecan plus cisplatin). We have previously published data regarding the efficacy and safety of this treatment regimen.19
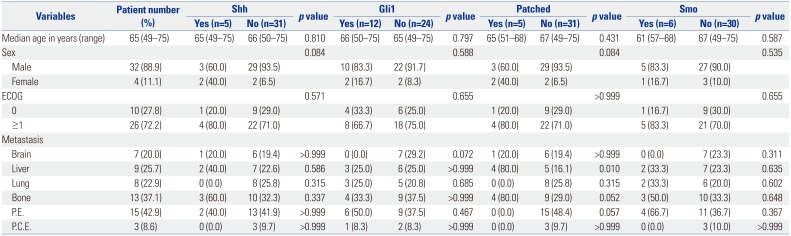
Table 1
Baseline Characteristics of Patients according to Expression Status Related to Shh Pathway
Shh, sonic hedgehog; Gli1, glioma-associated oncogene homolog zinc finger protein 1; Smo, Ptch-mediated repression of smoothened; ECOG, Eastern Cooperative Oncology Group; P.E., pleural effusion; P.C.E., pericardial effusion.
Values are presented as median (range) or n (%) unless otherwise indicated.
![]()
Of the 36 specimens examined, overexpression of Gli1, patched, Shh, and Smo was found in 12 (33.3%), five (13.9%), five (13.9%), and six (16.7%) cases, respectively (Fig. 2). We evaluated the correlation between overexpression of each protein and found that the overexpression of Gli1 and Shh (p=0.034), and Shh and Patched (p=0.001) were correlated to each other (Table 2). There was no correlation between the expression status of other proteins.
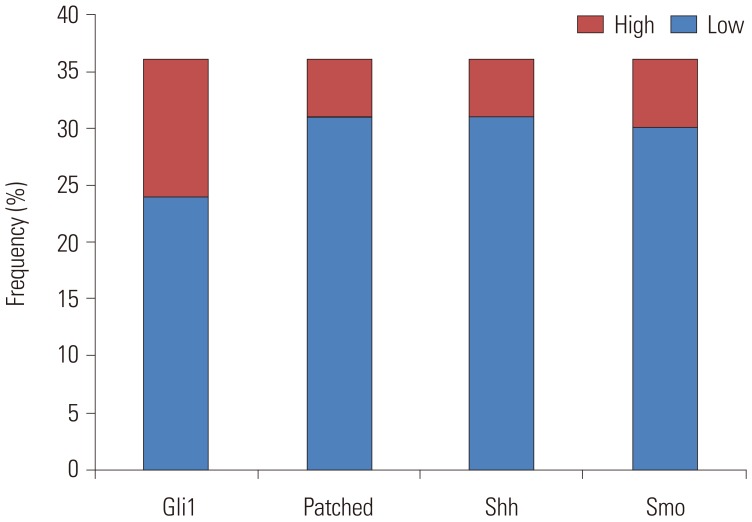 | Fig. 2Frequency of overexpression for each protein. Gli1, glioma-associated oncogene homolog zinc finger protein 1; Shh, sonic hedgehog; Smo, Ptch-mediated repression of smoothened.
|

We investigated the correlation between protein expression and clinical parameters. Patched overexpression was correlated with liver metastasis, and had a tendency for bone metastasis and pleural effusion. Although overexpression of Shh appeared to be more common in female patients and Gli1 expression seemed to have negative correlation with brain metastasis, both had no statistical significance (Table 1). Other than that, no correlation was found between protein expression and other clinical parameters.
Survival outcome according to expression status of proteins related to Shh pathway
In overall patients, response rate to chemotherapy was 84% (all partial response), and percentage of patients exhibiting a stable disease was 11.9%. There was no association between overexpression of each protein and response rate.
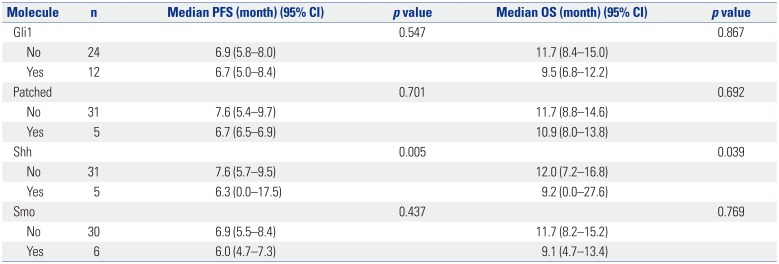
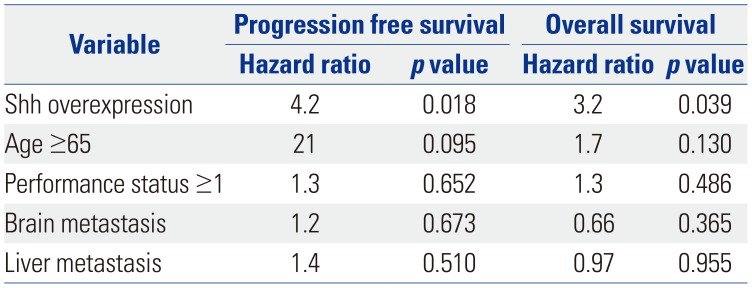
The median PFS and OS were 6.9 months and 11.2 months, respectively. We investigated the association between overexpression of each protein and patients' outcome. We performed univariate analyses of PFS and OS according to expression status of proteins related to Shh pathway and other clinical parameters (Table 3, Fig. 3). We found that higher expression of Shh was associated with worse PFS (6.3 vs. 7.6 months, p<0.01) and OS (9.2 vs. 12.0 months, p=0.039) (Fig. 3), whereas other protein expression was not related to patient prognosis. Shh overexpression remained as a poor prognostic factor (Table 4) with a hazard ratio of 3.2 after adjustment of age, ECOG PS, brain metastasis, and liver metastasis.
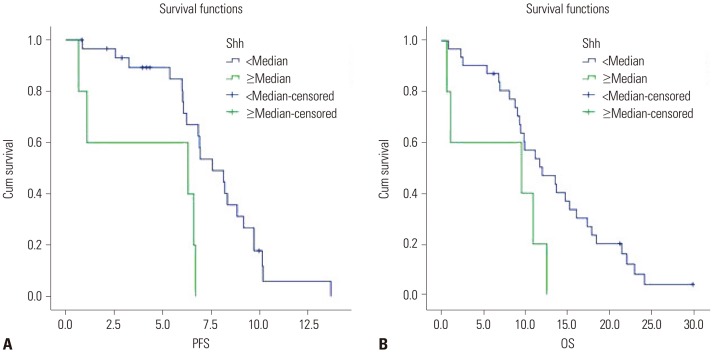 | Fig. 3Kaplan-Meier analysis of progression free survival (PFS) (A) and overall survival (OS) (B) according to sonic hedgehog (Shh) expression.
|
Table 3
Univariate Analysis for Progression Free Survival (PFS) and Overall Survival (OS)
![]()
Table 4
Multivariate Analysis for Progression Free Survival and Overall Survival
![]()
Go to :
DISCUSSION
In this study, we investigated the expression of components of Shh pathway and their prognostic ability in patients diagnosed with ES-SCLC. Our study indicated that some subsets of SCLC tumors expressed proteins related to Shh pathway. Among them, Shh overexpression was associated with worse prognosis in ES-SCLC patients.
It remains uncertain how Shh pathway is involved in lung cancer carcinogenesis. It has been shown that Shh signaling pathway is critical for growth and differentiation of the trachea and lungs, and its aberrant expression may be involved in abnormal development of the lungs. Shh signaling is thought to possibly be inactive in the human adult lung epithelium, except in epithelial progenitor (stem) cells.
Although we could not explain the underlying mechanisms of the prognostic effect of Shh pathway in SCLC, previous studies conducted on NSCLC may give some insight into this matter. Hwang, et al.18 suggested that induction of proliferation and activation of lymphangiogenesis could result in a survival disadvantage in patients with tumors showing high Shh expression. Chemo- and radioresistance conferred by this pathway could be another explanation for the association between Shh signaling and poor prognosis.14 Further studies are warranted to clarify how Shh pathway can affect the survival outcome of SCLC patients.
Shh pathway inhibition was considered and tested as a relevant therapeutic target for treatment of SCLC. Preclinical studies have demonstrated that Shh pathway inhibition is a novel strategy for eradicating cancer stem cells.20 To date, there has been one published study investigating the efficacy of visdemogib, a selective hedgehog pathway inhibitor, in patients with ES-SCLC.21 Disappointingly, no significant improvement was shown in the survival outcome with the addition of vismodegib to standard chemotherapy, and the authors concluded that further evaluation of hedgehog inhibitors with chemotherapy could not be recommended for patients with SCLC. However, for the following reasons, we propose that it is premature to conclude that Shh pathway is not a relevant target for SCLC patients. First, as pointed out by the authors, the study design included visdemogib during the concurrent and maintenance phases of treatment. Therefore, administration of a hedgehog inhibitor on a different schedule might yield more favorable outcomes. Second, and more importantly, the trial was not a biomarker-driven study. As we have learned from the studies investigating the use of gefinitib in epithelial growth factor receptor-mutated non-small cell lung cancer,2223 identification of the correct target population is the most crucial step for successful clinical trials. Hence, another clinical trial that exclusively enrolls patients with the aberration in Shh pathway is warranted. Finally, other studies using different Shh pathway inhibitors (NCT01579929, NCT00927875, and NCT01722292) are ongoing, and it is prudent to await the results of those studies before evaluating the importance of Shh pathway in ES-SCLC.
Our study had several limitations. First, since this was a retrospective study with a small number of patients, we should be cautious about interpreting these results due to the possibility of population selection bias. Therefore, subsequent studies using a larger prospective validation cohort are required to validate the prognostic ability of the Shh IHC score. Also, issues regarding the Shh detection method should be discussed here. There has been no previously validated method to detect Shh pathway aberration. Although IHC was chosen in this study in accordance with previous reports,1418 further studies using other detection methods, such as direct sequencing, next-generation sequencing, or RNA array, are warranted.
In conclusion, this is the first report on the relationship between components of Shh signaling pathway and prognosis in patient with ES-SCLC. We found that a large proportion of tumors expressed proteins related to Shh pathway, and overexpression of Shh was correlated with worse PFS. Further studies are needed to clarify the role of Shh signaling pathway in SCLC and the underlying mechanisms that are responsible for driving the malignant behavior of SCLC.
Go to :
 XML Download
XML Download