

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Breast cancer is one of the major causes of death among women worldwide, and its incidence continues to increase (12). Because of the early detection of breast cancer through medical imaging and advances in treatment methods, survival rates of patients with breast cancer have increased recently. Factors that determine the prognosis of breast cancer include age, tumor size, lymph node metastasis (TNM staging), histological characteristics (e.g., histological subtype, nuclear grade, lymphovascular invasion), and hormone receptors such as estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor receptor 2 (HER-2) (3). Larger tumor sizes, higher histological grades, more extensive lymph node metastasis, HER-2-positive tumors, and ER- and PR-negative tumors indicate poorer prognoses. Invasive ductal carcinoma (IDC) is graded from 1 to 3 depending on the extent of tubular formation, nuclear pleomorphism, and mitosis; generally, higher grades indicate poorer prognoses (4). These prognostic factors for breast cancer are important for the follow-up treatment and management of patients (5).
Dynamic contrast-enhanced MRI techniques, using a contrast medium, can reduce the number of histological tests performed and assist in the detection of multifocal breast cancer and the determination of the breast cancer stage. Although dynamic contrast-enhanced MRI is the technique with the highest sensitivity for diagnosing breast lesions, the specificity of MRI is disputed (6). Recently, the specificity of dynamic contrast-enhanced MRI for malignant breast lesions has been improved through the use of diffusion-weighted imaging (DWI) (7). Most malignant tumors exhibit high cellularity, thereby preventing water diffusion and displaying high signal intensity on DWI; moreover, these tumors have low apparent diffusion coefficients (ADCs), which measure the magnitude of the diffusion of water molecules that are present within the body. These malignant tumors contain more cells than lesions with high ADCs, indicating that they inhibit water diffusion. Several studies have attempted to utilize this phenomenon to diagnose breast cancer, and have reported an association between ADCs and prognostic factors for breast cancer (8910111213). In addition, attempts are currently underway to predict lesion malignancy through the use of the peak standardized uptake value (pSUV) of PET using 18-fluorodeoxyglucose (FDG) (14). This technique is based on the phenomenon that high levels of malignant tumor metabolic activity are observed on PET, as a result of increased carbohydrate metabolism within the tumor itself, as well as on various biochemical characteristics of the tumor and other external factors (15). Previous studies have reported cut-off values for distinguishing between malignant and benign tumors, using ADCs on DWI and pSUVs of PET-CT (81011121617). Within this context, we aimed to characterize ADCs on DWI and pSUVs of PET-CT, to investigate their correlations with prognostic factors for breast cancer as well as with MRI findings.
MATERIALS AND METHODS
This retrospective study was performed with Institutional Review Board approval and the requirement for obtaining informed patient consent was waived (IRB No. 2018-11-002). A total of 126 patients diagnosed with breast cancer, based on histological examinations at our institution between January 2012 and December 2015 (mean age, 53.5 years; range, 30–87 years), were retrospectively analyzed.
The exclusion criteria were as follows: patients who did not undergo surgery (20 patients), patients who underwent pre-operative neoadjuvant chemotherapy or pre-operative endocrine treatment (10 patients), patients histologically confirmed to have benign lesions (9 patients), and patients who provided low-quality medical images with MRI artifacts (5 patients).
Of all 126 patients, 44 patients in total were excluded from the study. Ninety-four breast lesions from 82 women, including six bilateral and three multifocal lesions, were included. Immunohistochemical staining was performed on all lesions. Those lesions that had been subjected to MRI or PET-CT were further analyzed. Among these, 87 lesions were available for mean ADC measurements. pSUVs were recorded for 87 lesions. Both mean ADCs and pSUVs were recorded for 80 lesions.
For MRI, a Philips Intera Achieva 3.0T MRI system (Philips Medical Systems, Best, the Netherlands) was used. A bilateral four-channel phase array breast coil was used while the patient was in a prone position. Axial DW images of both breasts were obtained. In single-shot echoplanar imaging with sense encoding, b-values of 0 mm2/s and 1000 mm2/s were used. The parameters were repetition time/echo time (TR/TE) = 1825/57, field of view (FOV) = 350 × 350 mm2, matrix size = 116 × 115, 2.0 number of excitations (NEX), section thickness = 5 mm, and intersection gap = 0. For the calculation of ADCs, two radiologists, who were blinded to the results, placed as many multiple circular regions of interests (ROIs) with a diameter between 5 and 10 mm. When compared with dynamic contrast-enhanced MRI, the enhancing solid portion of the tumor was used for the ADC measurement without including necrosis or liquids. Mean ADCs were automatically calculated when drawing the ROIs.
T2-weighted MRI images of the axial view of both breasts were obtained, using the spectral adiabatic inversion recovery and spectral attenuated inversion recovery (SPAIR) technique. The parameters were TR/TR = 2660/70, FOV = 339 × 339 mm2, matrix size = 584 × 342, 1.0 NEX, section thickness = 4 mm, and intersection gap = 0. For T1-weighted MRI images, the axial T1-weighted 3 dimensional dynamic gradient-echo fat-suppressed sequence technique was used to obtain one pre-contrast image, along with seven early and delayed contrast-enhanced images, each at a 1-minute interval. The parameters were TR/TE = 3.8/1.9, FOV = 340 × 340 mm2, matrix size = 424 × 424, 1.0 NEX, section thickness = 1.5 mm, intersection gap = 0.
For PET-CT, a Gemini TF PET-CT scanner (Philips Medical Systems) was used. PET-CT was performed 50–60 minutes after intravenous administration of FDG. The parameters for CT were slice thickness = 4 mm, 120 kVp, and 100 mAs. A single expert in nuclear medicine examined the PET-CT images, and lesions showing high levels of FDG consumption, compared with surrounding breast tissues, were considered a positive indication for the presence of a tumor. A radiologist confirmed the locations of these lesions and calculated their pSUVs.
For the analysis of the prognostic factors for breast cancer, patients were classified as ≤ 50 or > 50 years of age. Tumor size was measured as the maximum diameter of the tumor in pathologic results, and was divided into ≤ 2 and > 2 cm. Tumors were categorized according to the expression levels of ER, PR, HER-2, and four major subtypes (Luminal A, Luminal B, HER-2-enriched and triple-negative breast cancer). The expression level of HER-2 was semiquantitatively recorded as 0, 1+, 2+, or 3+. Tumors that scored 3+ were classified as HER-2-positive. Tumors with an HER-2 expression of 2+ were reevaluated according to recent guidelines (18). Tumors that scored 2+ were studied using fluorescent in situ hybridization to determine the HER-2 gene amplification. Tumors that scored 0 and 1+ were classified as HER-2-negative. Breast cancer was histologically analyzed by referring to reports of pathological results. IDC was graded, from grade 1 to grade 3. For lymph node testing, a sentinel lymph node resection was performed, and axillary lymph node resection was immediately performed upon determination that the sentinel lymph node was positive (+). MRI findings regarding breast cancer were classified according to the 5th Edition of the American College of Radiology of the Breast Imaging-Reporting and Data System. Breast lesions were divided into mass and non-mass enhancement (NME). The shape (round/oval vs. irregular), margin (circumscribed vs. not circumscribed), mass internal enhancement (homogeneous vs. heterogeneous vs. rim enhancement; there were no cases with dark internal septations), and kinetic curve assessment (initial phase: slow vs. medium vs. fast/delayed phase: persistent vs. plateau vs. washout) of the mass lesions were analyzed. Two radiologists analyzed the MRI findings and ADCs on DWI, respectively, and came to a consensus. Mean ADCs and pSUVs of each lesion were recorded to analyze their correlations with age, tumor size, histologic grade, hormone receptor expression, and MRI findings.
For statistical analysis, the SPSS, version 20.0 (IBM Corp., Armonk, NY, USA) was used. Mann-Whitney and Kruskal-Wallis tests were respectively used to analyze how the ADC value and mean pSUV of each lesion correlated with prognostic factors (age, tumor size, cancer grade, lymph node metastasis, ER, PR, and HER-2 receptor) as well as with the MRI findings, and to find differences in the mean pSUVs and ADCs according to the histologic grade of the cancer. To investigate how histological diagnosis and grade correlated with the pSUVs and ADCs, a Pearson correlation analysis was performed. To analyze how the histologic grade of the breast cancer correlated with the ADCs and pSUVs, a linear regression analysis was performed. Moreover, prognostic factors were subjected to multiple regression analysis to determine those that were independently associated with the mean ADCs and pSUVs. The level of statistical significance was set at p < 0.05.
RESULTS
Of the 94 lesions, 78 (83.0%) were identified as IDC, 13 (13.8%) as ductal carcinoma in situ (DCIS), 2 (2.1%) as invasive lobular carcinoma, and 1 (1.1%) as mucinous carcinoma. There were 10 cases of grade 1 lesions (12.8%), 23 cases of grade 2 lesions (29.5%), and 45 cases of grade 3 lesions (57.7%). As for the age distribution, 40 patients (42.6%) were ≤ 50 years old, whereas 54 patients (57.4%) were > 50 years old. Mean tumor size was 1.99 cm (range, 0.3–5.7 cm). Thirty-three tumors (35.1%) tested positive for lymph node metastasis, whereas 61 (64.9%) tested negative. Among the patients who underwent MRI, 13 had NMEs and 74 had mass lesions. The classification by internal enhancement revealed 39 homogeneous enhancements, 13 heterogeneous enhancements, and 22 rim enhancements. The kinetic curve assessment showed that four lesions were slow and none were medium during the initial phase. Since most lesions exhibited a fast kinetic curve (83 lesions), a statistical analysis for the initial phase could not be performed. Moreover, during the delayed-phase kinetic curve assessment, 3, 28, and 56 lesions were classified as persistent, plateau, and washout, respectively.
A significant difference in mean pSUVs was found between tumors measuring ≤ 2 cm and tumors measuring > 2 cm (2.74 and 6.99, respectively) (p = 0.001). No significant difference was found in mean ADCs according to tumor size (p = 0.270). Significant differences in mean ADCs and pSUVs were found according to the extent of lymph node metastasis (p = 0.013 and p = 0.001, respectively) (Figs. 1, 2). As for the MRI findings, mean ADCs were 0.92 × 10−3 mm2/s and 1.04 × 10−3 mm2/s for the mass and NME lesions, respectively (p = 0.043). There was a significant difference in mean pSUVs between round/oval shape mass lesions and irregular shape mass lesions (2.76 and 5.02, respectively) (p = 0.004). In the analysis of internal enhancement of the mass lesions, statistically significant differences were found in mean pSUVs between homogeneous enhancements and rim enhancements (p = 0.001).
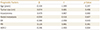
The mean pSUV across all patients subjected to PET-CT was 4.50; it was 1.64 for DCIS and 5.05 for IDC. The mean pSUVs for IDC, according to histologic grade, were 1.60 for grade 1, 3.75 for grade 2, and 6.21 for grade 3. Mean pSUVs increased as the histologic grade increased, in a statistically significant fashion (p = 0.001). The mean ADC across all patients subjected to MRI was 0.94 × 10−3 mm2/s, whereas it was 1.11 × 10−3 mm2/s for DCIS and 0.89 × 10−3 mm2/s for IDC. The mean ADCs for IDC, according to histologic grade, were 0.93 × 10−3 mm2/s for grade 1, 0.92 × 10−3 mm2/s for grade 2, and 0.90 × 10−3 mm2/s for grade 3. Mean ADCs significantly decreased as the histologic grade increased (p = 0.017) (Fig. 3). In the analysis of hormone receptors, a significant difference was found in mean pSUVs between ER-negative and ER-positive lesions (5.74 and 3.88, respectively) (p = 0.040). However, there was no significant difference in mean pSUVs and ADCs according to the expression level of other hormone receptors (PR and HER-2). The mean pSUVs of Luminal A and triple-negative breast cancer were significantly different (3.44 and 6.74, respectively) (p = 0.028) (Tables 1, 2).
DISCUSSION
MRI is widely known as an imaging technique that plays an important role in the detection, diagnosis, and staging of breast cancer (192021). DWI, which is currently a popular focus of research, quantifies the magnitude of water diffusion in breast cancer lesions and expresses it as ADCs. PET-CT utilizes the high metabolic activity of tumors to distinguish between malignant and benign lesions and can thus be used for diagnosing and staging cancer, as well as for assessing relapse and treatment responses (2223).
In the current study, we analyzed how pSUVs of PET-CT and ADCs on DWI correlate with age, tumor size, lymph node metastasis, hormone receptors, histologic grade, and MRI findings.
Tumor size is an important prognostic factor for breast cancer and is associated with overall survival (2425). In a multivariate analysis in our study, tumor size was significantly associated with mean pSUVs, but not with mean ADCs. Although the size standard used in this study slightly differed from those used in previous studies (in our study, lesions were classified as ≤ 2 cm or > 2 cm), the results are similar to the majority of previous reports (12161726). Conversely, Razek et al. (9) reported an association between mean ADC and tumor size; however, in their study, patients with tumors measuring < 1 cm were excluded, since those tumors were assumed to be difficult to detect on DWI.
Breast cancer grade is also closely associated with patient survival. In this study, significant differences were found in mean ADCs between lesions with various levels of invasiveness, (i.e., between IDC and DCIS). In a study by Nakajo et al. (16), similar to our study, a significant difference in mean ADCs was found between IDC and DCIS; in contrast, there was no significant difference in mean pSUVs.
Numerous prior studies have reported that tumor cellularity is a factor that affects tumor grade and an in inverse correlation exists between mean ADCs and tumor cellularity (25272829). Since most tumors exhibit increased glucose metabolism as their size or histologic grade increases, FDG consumption consequently increases (153031).
In our multivariate analysis on hormone receptors, ER and HER-2 receptor states were significantly associated with mean ADCs, whereas other receptors were not associated with mean ADCs and pSUVs. Choi et al. (11) found that mean ADCs and pSUVs were significantly higher for ER-negative tumors. Similarly, Ludovini et al. (32) reported that in ER-positive tumors, ER blocks the angiogenic pathway and reduces perfusion, thereby affecting ADCs. The results of the present study, although we found no significant differences in pSUVs, are largely identical to those of Choi et al. (11) and Ludovini et al. (32).
In the current study, mean pSUVs for ER-negative and ER-positive lesions significantly differed from each other (5.74 and 3.88, respectively), and the same was observed for the pSUVs of Luminal A and triple-negative breast cancer (3.44 and 6.74, respectively). This is consistent with the results of a previous study. Baba et al. (17) also reported that mean pSUVs were significantly associated with triple-negative breast cancer. As the results of previous studies show, however, considerable variation regarding the relationship between hormone receptors and pSUVs or mean ADCs, large-scale research studies may be needed to further clarify this relationship.
In our current study, significant differences in pSUVs and ADCs were found according to the extent of lymph node metastasis; this is consistent with several previous findings (910). Chung et al. (33) evaluated mean ADCs of the lymph node itself and found that the mean ADC is useful for predicting metastatic axillar lymph nodes. However, in our multivariate study, neither mean ADCs nor pSUVs showed a statistically significant relationship with lymph node state, because the lymph node state is not an independent prognostic factor itself but, rather, is related to other prognostic factors.
This study has several limitations. First, the sample population was small (94 lesions). Of these, 78 (83.0%) were classified as IDC and 13 (13.8%) as DCIS; therefore, there were significantly fewer cases of DCIS than of IDC. Second, since this study was a retrospective study conducted at a single institution, there is a possibility of selection bias. Third, since most lesions were histologically diagnosed as IDC and DCIS, the characteristics of other types of breast cancer [two cases of invasive lobular carcinoma (2.1%), and one case of mucinous carcinoma (1.1%)] are not reflected in the results. Fourth, it was difficult to objectively measure mean ADCs on DWI. For instance, in the case of NMEs, there may be a lack of consistency between measurements performed by different examiners. Lastly, because PET-CT was performed after all patients underwent histological examinations, an effect of the histological examinations on lesion behavior cannot be disregarded.
In conclusion, in this study, we found higher pSUVs for breast lesions of larger size and higher histologic grades, and lower ADCs on DWI for ER-positive breast lesions and lesions of higher histologic grades. These findings show that mean pSUVs of PET-CT and mean ADCs on DWI can help predict the prognosis of breast cancer. A comprehensive interpretation of DWI and PET-CT results may contribute to an improved accuracy of breast cancer diagnosis, histologic grading, and prognosis prediction, but it still has limitations. A larger-scale study is therefore needed.






 XML Download
XML Download