

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Mixed adenoneuroendocrine carcinoma (MANEC) was classified by the World Health Organization (WHO) in 2010 referring to a neoplasm with dual adenocarcinomatous and neuroendocrine differentiation. It is very rare malignancy of gastrointestinal tract and several cases were reported in the pancreas, colon, gallbladder, biliary tract, stomach, ampulla, cecum and esophagogastric junction, in order of frequency (1). But, there are only few reports in the small bowel, especially in Crohn's disease patient. Here, we report a case of MANEC of the small bowel in Crohn's disease patient.
CASE REPORT
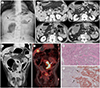
A 54-year-old male visited to our emergency room for abdominal pain and distension for 3 weeks. He had the diagnosis of Crohn's disease for 30 years, and the surgical history of the segmental resection of ileum for bowel obstruction and primary repair for enteric fistula. Bowel sound was absent on physical examination, and simple radiograph showed ileus (Fig. 1A). On initial laboratory examination, white blood cell count was 14080/µL with neutrophilia of 85% and the C-reactive protein was elevated to 5.3 mg/dL.
A dynamic phase contrast-enhanced abdominopelvic computed tomography (CT) was performed. CT examination revealed an asymmetric segmental wall thickening of jejunum (Fig. 1B, C). The thickened bowel showed heterogeneous enhancement with loss of normal layered pattern, and mesenteric fat stranding. Mild proximal small bowel dilatation also showed. And there were multiple enlarged mesenteric lymph nodes with central low density (Fig. 1B) and several ill-defined low density hepatic nodules in both lobes (Fig. 1B, C). And the thickened small bowel also showed hot uptake on 18F-fluorodeoxyglucose positron emission tomography/CT (PET/CT) with maximal standardized uptake value 13.3 (Fig. 1D). We suspected adenocarcinoma of small bowel with metastatic lymphadenopathy and hepatic metastasis. Serum carcinoembryonic antigen was elevated (203.5 ng/mL) and other tumor markers, such as alpha fetoprotein and carbohydrate antigen 19–9 were within normal range.
We performed a ultrasonography-guided core needle biopsy on hepatic nodule and the initial pathology was an adenocarcinoma, probably metastasis from the small bowel carcinoma. The patient was treated with conservative therapy and discharged for further chemotherapy of the cancer.
2 weeks later, the patient came to our emergency department again for pneumoperitoneum. An emergency operation was done. And there were several perforation sites at small bowel, so we did a segmental resection of small bowel. On microscopy, the tumor revealed a classic adenocarcinoma component with glandular growth pattern as well as a neuroendocrine component on hematoxylin and eosin stain (Fig. 1E). And the neuroendocrine proportion showed positive reaction on chromogranin and synaptophysin immunohistochemical stain, while the glands of the adenocarcinoma component stain negative (Fig. 1F). The final pathology was a MANEC of small bowel. The patient underwent a conservative treatment after the surgery but was died after 2 months.
DISCUSSION
According to the WHO classification system published in 2010, neuroendocrine tumors in the digestive system were classified as neuroendocrine tumor grade 1, neuroendocrine tumor grade 2, neuroendocrine carcinoma, and MANEC. And MANEC is defined as having combined exocrine and neuroendocrine components, where each of these components composed at least 30% of the tumor (2). Also mixed exocrine and neuroendocrine tumor can be classified by morphological patterns of the two components; combined tumors (admixed of exocrine and neuroendocrine components within a single lesion, also known as intermingled tumors), collision tumors (two components occur in separate areas of the same lesion, without admixture), or amphicrine tumors (two components are present in the same neoplastic cell) (3). And according to this classification, our case was a combined tumor.
Crohn's disease patients have a high risk of developing large and small bowel adenocarcinoma compare to the general population. The relative incidence of small bowel adenocarcinoma in Crohn's disease is 3.4–66.7 fold higher than the general population. Similarly, they have an increased risk of developing neuroendocrine tumor of the gastrointestinal tract. Crohn's disease is associated with a 14.9 fold incidence of neuroendocrine tumor compare to incidental neuroendocrine tumor found in appendectomy specimen from healthy people. However, as most neuroendocrine tumors are found incidentally during surgery their true incidence in Crohn's disease is unknown (45).
It is unclear whether there is a connection between the pathogenesis of Crohn's disease and carcinoid tumor. Some carcinoid tumors are found in colonic segments that are free from inflammation. This finding suggests that the development of neuroendocrine tumor in Crohn's disease may result from local inflammation and/or may be secondary to distant secretion of mediators (45).
Simultaneous presence of neuroendocrine tumor and Crohn's disease is extremely rare, with 52 reported cases in the literature (5). And among them, only 5 cases of coexistent Crohn's disease and mixed adenoneuroendocrine tumor have been reported, as we know. Of the 5 cases, 1 case occurred in the cecum, and other 4 cases occurred in the terminal ileum. The most common clinical presentation of the small bowel mixed adenoneuroendocrine tumor is intestinal obstruction, similar to our case (567). However, these reports only focus on clinical and pathologic features.
Crohn's disease-related neuroendocrine tumor is very rare, so there are only little attention about imaging findings. It can present as a mural thickening associated with luminal narrowing and proximal dilatation, or a soft tissue mass on CT. In Boltin's case, the CT scan also shows a segment wall thickening and luminal narrowing of terminal ileum with proximal bowel dilatation (58). However, Crohn's disease-related small bowel adenocarcinoma also shows similar image findings. Small bowel adenocarcinoma may present as 4 different patterns on CT, such as enhancing mass, long stenosis with heterogeneous submucosal layer and moderate enhancement, short and marked stenosis with resulting proximal small bowel dilatation, or sacculated small bowel loop with irregular and asymmetric circumferential thickening. Clearly visible mass can be detected only in 50% of the adenocarcinoma of Crohn's disease patient. Some cases show luminal narrowing and proximal bowel dilatation without visible mass on CT scan, similar to benign fibrotic or acute inflammatory stricture. So, it is very difficult to differential diagnose between benign stricture of Crohn's disease, Crohn's disease-related adenocarcinoma and neuroendocrine tumor in preoperatively (89).
The optimal management of MANEC is largely unknown, due to its rarity. But, the more aggressive component of MANEC should be considered in treatment. MANEC containing a well differentiated neuroendocrine component and an adenocarcinoma component should be treated as adenocarcinoma. MANEC containing a poorly differentiated neuroendocinre component should be treated as neuroendocrine carcinoma (10). Also, the prognosis of MANEC depends on the grade of malignancy of each component.
In this report, we report a MANEC of the small bowel in Crohn's disease patient. Because of its rare incidence and non-specific image finding, it is difficult to diagnose MANEC before surgery. However, MANEC has different treatment and prognosis with other diseases. Therefore, we should understand the disease entity of MANEC so that appropriate treatment can be done. And, this report will help to consider the possibility of MANEC when there is small bowel wall thickening with bowel obstruction or perforation on CT in Crohn's disease patients.
 XML Download
XML Download