

 PDF
PDF Citation
Citation Print
Print



BACKGROUND
Korea has the second longest working hours from 2008 to 2017 after Mexico among Organization for Economic Cooperation and Development countries [1]. This might be due to a low employment rate, instability of working, high work pressure, or traditionally strict and fastidious workplace culture of the society.
The various health outcomes caused by long working hours have been continuing issues in Korea. Previous studies have reported long working hours was related to weight gain, fatigue, injuries, and musculoskeletal diseases [2345]. Many other studies have also revealed the negative effects of long working hours on cardiovascular diseases [5678]. An investigation on British civil servants had reported that 3 to 4 hour of overtime work per day was related to an increased risk of incident coronary heart diseases comparing workers with no overtime [7]. A case-control study by Jeong et al. [8] also have shown the risk of cardiovascular diseases for the over 60-hour working group. Furthermore, psychological conditions such as stress, anxiety, depression, and insomnia are found to be associated with long working hours [9101112]. According to Yoon et al. [13], long working hours was linked to suicidal thoughts in groups with over 60 hours work compared to groups with less 52 hours work.
Most of the researchers and physicians have been largely neglecting the negative effects of alopecia. Nevertheless, it has been becoming a quite important health problem these days. Alopecia is not a critical or life-threatening disease, but it does have a significant impact on the psychological area. A previous study with self-report questionnaires has revealed that the diffuse hair loss group has significantly higher scores on stresses and depressive feelings but lower scores on self-confidence [14]. In addition, both men and women with alopecia were identified to possess less body-image satisfaction and a pattern of less adaptive functioning [1516]. Some studies have also shown that unstable psychological state and pathological symptom occurrence rates increased, while reliability on their own ability decreased in the hair loss group [17]. Furthermore, it was reported that interpersonal stress and daily-life stress have high correlations with hair loss [18].
The number of alopecia patients in Korea has increased from 166,000 in 2007 to 194,000 in 2011, an increase of about 28,000 (17.0%). The annual average growth rate was 4.0%. Total medical expense was increased by South Korean Won (KRW) 4.7 billion over these five years (from KRW 10 billion in 2007 to KRW 14.7 billion in 2011), with an annual average growth rate of 10.3% [19]. This statistical result was obtained only for population covered by National Health Insurance benefits. This means there will be much more alopecia patients if we add people who do not take any treatment at a clinic or people paying in cash without medical benefits.
Causes of hair loss are known to include genetic factors, stress, infection, unbalance of androgen hormones, blood circulation disorders, nutritional imbalance, and drug use [20]. According to sex, men with hair loss showed significant differences in family history of alopecia and number of staining. Women with hair loss also showed significant differences in family history of alopecia, experience of childbirth, number of staining, number of perms, and use of hair dryer [21].
However, no previous studies have examined the relationship between working hours and alopecia development. Only a few studies have reported that job-related stress could have correlations with employees' hair loss [2223]. Further investigation would help us to elucidate the need for moving forward to appropriate and reasonable working hours in our society. Thus, the main purpose of this study is to explore the relationship between long working hours and the development of alopecia among Korean male workers.
METHODS
Study design and subjects
The Kangbuk Samsung Health Study is a study of Korean men and women 18 years of age or older who underwent a comprehensive annual or biennial health examination at the clinic of Kangbuk Samsung Hospital Total Healthcare Center in Seoul and Suwon, Korea. To investigate the relationship between long working hours and the development of alopecia among Korean male workers, we used this health examination data retrospectively and followed up male employees who had not taken alopecia medicine yet in 2013 to see if they were going to take alopecia medicine after 4 years.
The study population was 43,383, consisting of the subset of Kangbuk Samsung Health Study participants who were males with age of 20 to 59 years. All of them were workers who answered “yes” to the following question, “Have you worked more than one hour for the last week for income purposes?” and visited the healthcare center both in 2013 and 2017.
Of these subjects, 13,853 workers who had missing data for questions about age, marital status, education, household income, smoking, alcohol, vigorous exercise, working hours, work schedule, and taking alopecia medicine were excluded first. To establish baseline, 710 workers who were already taking alopecia medicine in 2013 were additionally excluded so that all baseline subjects in this study consisted of employees without alopecia in 2013.
Working time is a key variable in this study. However, a lot of employees changed their answers for working hours between 2013 and 2017. Therefore, 14,703 employees who changed their answers for working hours, as much as their working hour classification should be reconsidered, were excluded to make sure that all subjects in this study had quite consistent working hours during the follow-up period.
Finally, 13,391 subjects were included in the analysis.
Working hours
Weekly working hours were based on the answer to the question, “During the last 1 year, how much was your average working hours per week including night work and overtime?”
Based on a five-day working system in Korea, principal working hours is up to 40 hours per week. From 2011, companies with five or more full-time workers are not allowed to let their employees work over 52 hours per week by legislation. In this regard, working hours were classified into three categories for analysis: reference working hours (RWH; up to 40 hours/week), long working hours (LWH, 40–52 hours/week), and much longer working hours (MLWH; > 52 hours/week).
Alopecia development
Since there were no specific questions or physical examinations about the diagnosis of alopecia, the question of “Do you take any oral medication for alopecia?” was used to confirm alopecia development. If subjects answered “no” to this question in 2013 and answered “yes” to the same question in 2017, those subjects were defined as employees with alopecia development after 4 years.
Socioeconomic and lifestyle factors
Socioeconomic factors included age group (20–29, 30–39, 40–49, 50–59), marital status (unmarried, married, and separated/divorced/bereaved/cohabitation), educational level (under high school diploma as low, bachelor degree as middle, master and doctor degree as high), and monthly household income (< 400, 400–600, > 600 × 104 KRW).
Lifestyle factors included smoking (non-smoker, smoker), alcohol consumption (non-drinker, drinker), regularly vigorous exercise (no, yes), weekly working hours (RWH, LWH, MLWH), and work schedule (daytime, non-daytime).
Statistical analysis
IBM SPSS Statistics ver. 24.0 (SPSS Inc., Chicago, IL, USA) was used for all data analyses. Descriptive statistics for baseline characteristics were calculated separately for each working hour group. Proportions of alopecia development after 4 years were calculated within strata of working hour groups and other covariates. Logistics regression analyses were conducted to calculate odds ratios (ORs), 95% confidence intervals (CIs), and p for trend of alopecia development after 4 years of LWH and MLWH groups relative to the RWH group. ORs were adjusted for age group, marital status, education, monthly household income, smoking, and work schedule. To avoid interactions clearly, adjusted ORs were also calculated in several individual models within covariates' strata.
RESULTS
Table 1 shows baseline characteristics of study participants categorized by working hour groups. The 28.2%, 59.3% and 12.5% of subjects were in RWH, LWH, and MLWH group each. Over 80% of participants were in their 30s and 40s with married status. About 90% of subjects were alcohol drinkers and daytime workers. Percentages of participants who graduated from a university or a graduate school were more in LWH (86.4%) and MLWH (86.7%) groups compared to the RWH group (72.6%).
Table 1
Baseline characteristics of study populations categorized by working hour groups
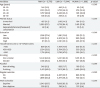
Data are presented as number (%).
RWH: reference working hours (< 40 hours/week); LWH: long working hours (40–52 hours/week); MLWH: much longer working hours (> 52 hours/week); KRW: South Korean Won.
ap-value by χ2 test.
![]()
As working time got longer, proportions of employees who earned over 600 × 104 KRW for a monthly household income increased (45.4%, 47.0%, and 56.1% for RWH, LWH, and MLWH, p < 0.001) while proportions of workers who were doing vigorous exercise regularly decreased (50.2%, 46.3%, and 42.1% for RWH, LWH, and MLWH, p < 0.001).
Table 2 shows proportions of alopecia development after 4 years based on selected characteristics of the study population. The proportion of alopecia development increased linearly with increasing working hour category (2.0%, 3.4%, and 3.8% for RWH, LWH, and MLWH, p < 0.001). When working hours were getting longer, populations of those who were in their 30s (p = 0.002), married (p < 0.001), low-educated (p = 0.009), highly educated (p = 0.039), low-income (p = 0.001), smoking (p = 0.001), drinking (p < 0.001), regularly exercising (p < 0.001), and daytime-working (p < 0.001) also showed increased proportion of alopecia development. Results also showed that 20s, unmarried, highly educated, high-income, drinking, and daytime-working employees were more likely to take alopecia medicine than older, married, low-educated, low-income, non-drinking, and non-daytime workers.
Table 2
Proportions of alopecia development after 4 years based on selected characteristics of study populations
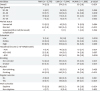
Data are presented as number (%).
RWH: reference working hours (< 40 hours/week); LWH: long working hours (40–52 hours/week); MLWH: much longer working hours (> 52 hours/week); KRW: South Korean Won.
ap-value by χ2 test.
![]()
Table 3 shows adjusted ORs, 95% CIs, and p for trend of alopecia development after 4 years of LWH and MLWH groups relative to the RWH group. ORs for development of alopecia after adjusting age, marital status, education, household income, smoking, and work schedule was 1.57 (95% CI: 1.21–2.05) for LWH group and 1.74 (95% CI: 1.23–2.47) for MLWH group relative to RWH group.
Table 3
Adjusted ORs, 95% CIs, and p for trend for alopecia development after 4 years of LWH and MLWH groups relative to the RWH group

Data are presented as ORs (95% CI). Adjusted with age group, marital status, education, household income, smoking, and work schedule.
OR: odds ratio; CI: confidence interval; RWH: reference working hours (< 40 hours/week); LWH: long working hours (40–52 hours/week); MLWH: much longer working hours (> 52 hours/week); KRW: South Korean Won.
![]()
Stratification revealed that the linear association of long work time with increase of alopecia development was strong for those who were in their 30s (p for trend = 0.007), unmarried (p for trend = 0.020), married (p for trend = 0.009), low-educated (p for trend = 0.045), highly educated (p for trend = 0.025), low-income (p for trend = 0.002), non-smoking (p for trend = 0.035), smoking (p for trend = 0.004), drinking (p for trend = 0.001), regularly exercising (p for trend = 0.003), and daytime-working (p for trend=0.001).
DISCUSSION
The results of this study demonstrate that long working hours is significantly associated with the increased development of alopecia in Korean male workers. Furthermore, the strength of association has increased linearly as work time got longer. Although we were unable to compare this result with previous studies since this was the first such research to investigate the relationship between working hours and alopecia development in workers, there are some noticeable results we may discuss.
Despite of whether the government of Korea has established regular working hours of 40 hours per week with a five-day working, we have just found only 28.2% of subjects were in the RWH group (< 40 hours/week), and that means over 70% of Korean male workers have to work overtime. Furthermore, 12.5% of subjects, classified in the MLWH group (> 52 hours/week), are currently working beyond the legal maximum overtime of 12 hours per week.
On the stratified results analyzed by age group, we have found significant differences in alopecia development according to working hours only in the 30s. According to Lee et al. [14], more than half of alopecia patients have experienced their first hair loss in the 30s. Based on this fact, the 30s could be the best age group that can reflect the actual hair loss development of employees, so it seems better for us to focus more on the result of the 30s. Although we could not find any statistically significant differences of the 20s, but it is also worth noting that workers who have worked more than 52 hours in the 20s had the alopecia development rate of 8.3% and this was a much higher rate than the 4.1% seen in the 20s with less than 40 hours of work. In this context, limitation of working hours in order to prevent alopecia development may be more necessary from younger workers, such as those in the 20s and 30s, at which hair loss symptoms start to appear.
The outcomes of married employees could have underestimated risks for the alopecia development. The adjusted ORs showed that unmarried employees had a much higher risk of alopecia development associated with working hours compared to married ones. This is probably related to one of our study limitations, which will be described in detail later. We have simply defined alopecia development as whether to take any alopecia medicine. Therefore, it is recommended to pay attention to previous research showing that unmarried people are more interested in their good appearance and are actively managing it comparing to married ones [2425]. If so, unmarried employees are likely to take alopecia medicine eagerly than married ones, which helps to reflect the alopecia development more closely. From this point of view, it would be better to take the results of unmarried employees rather than the results of married ones in our stratified analyzed data.
Other stratified substratum by socioeconomic status (income and education), behavioral risks (smoking, alcohol, and regular exercise), and work schedule have also demonstrated the consistent results for the risk of alopecia development by long working hours. Even though some results were not statistically significant, it is worth to note that none of the results in each stratum have contradict the hypothesis on positive correlations between working hours and alopecia development.
Finally, we would like you to pay attention to the positive association from the trend analysis (p for trend) which has been used to compare the alopecia development risks between working hour groups. There have been many other studies investigating the relationship between working hours and a variety of harmful health effects for it [2345678910111213], but we could rarely find any research that carried out the trend analysis. Our studies have verified the trends for the risk of alopecia development according to working hours and revealed the positive association in overall population and those in 30s, unmarried, married, low-educated, highly educated, low-income, non-smoking, smoking, drinking, regularly exercising and daytime working. From this result, our society might be able to get a critically momentous lesson. This could help the society be aware that, even if it is not possible to limit working hours strictly to 40 hours per week and overtime work is inevitable in a certain situation, it is still better to put some more efforts to reduce overtime hours consistently as much as possible.
Many previous researches on hospital doctors, police officers, mangers, professionals, and clerical workers have highlighted that long working hours is a core factor of job-related stress [262728293031]. long working hours can act both directly as a stressor that increases fatigue and indirectly by increasing the time that a worker is exposed to other sources of workplace stress. Some studies also have suggested that job stress could be one of reasons that cause hair loss for workers [2223].
A lot of studies have revealed the mechanism of alopecia development by stress. In mice experiments, stress was significantly related to the inhibition of hair growth, induction of catagen cycle, and damage of hair follicles by substance P and corticotropin-releasing hormone (CRH) [32333435]. Other researches have also suggested that stress can affect injuries and inflammations of hair follicles, cell deaths, and inhibit hair growth by action of catecholamine, prolactin, adrenocorticotropic hormone, CRH, β-endorphins, glucocorticoids, and a variety of neurotrophins including nerve growth factor [36373839404142434445464748].
Based on these previous researches, we can cautiously assume that the relationship between long working hours and the development of alopecia is likely to be mediated by job-related stress.
Our study has some limitations. First, to confirm the development of alopecia, we exploited the following question, “Do you take any oral medication for alopecia?” However, this question definitely cannot represent the entire patients with hair loss and it just reflects only a part of them. Many previous studies investigating alopecia have defined patients using a self-diagnosis questionnaire [141718]. However, the question like “Do you have any hair loss?” could imply the possibility of either over-diagnosis or under-diagnosis for alopecia. To avoid that, Lee et al. [14] has added the question of how many strands of hair were missing per day, and defined the alopecia group only for the subjects who had answered to fall in excess of 100 strands per day. In other studies, especially mainly conducted by dermatologists, patients with alopecia have been defined only after visiting a dermatology department in a hospital and getting a confirmed diagnosis through a doctor's examination [151620495051]. In contrast to previous studies, we have simply defined alopecia development as starting to take alopecia medicine. Yet, there could be some reasons that employees with hair loss do not take alopecia medicine. For example, they could simply use topical medications, nutritional supplements, or medicated shampoo products instead. Also, they could have no concerns at all about their hair styles so they just let it happen without any intervention. A previous study has revealed that only 62.6% of patients with hair loss have experienced any kind of medical treatment [14]. As a result of this, our study has a disadvantage to precisely classify employees with alopecia from ones without it, and is likely to be limited to those with severe alopecia. Nevertheless, it is important to remember that our study was not designed to investigate the prevalence of alopecia, but rather aimed to reveal the ratio of alopecia development between working hour groups. The measurement of negative predictive values for validity to define alopecia development with taking alopecia medicine is another area requiring a prospective study.
Second, selection bias might exist because many of employees who underwent health examination at the clinic of Kangbuk Samsung Hospital Total Healthcare Center are likely to belong to one of the biggest companies with high-quality welfare in Korea. It could mean that our findings cannot be extrapolated to entire Korean populations.
Finally, due to limited items on the questionnaire, it was not possible to include all variables such as family history of alopecia, the number of stainings, or the number of perms per year that may have strong effects on hair loss.
Nevertheless, our study also has a couple of powerful strengths. In contrast with cross-sectional studies that could not allow us to determine the temporality of the association, we did follow up the subjects over 4 years so that we could distinguish between cause and effect. In addition, our study included a relatively large sample size which helped us better determine average values.
CONCLUSIONS
In conclusion, our findings suggest that unintentional development of alopecia is another potential health consequence of long working hours in Korean male workers. Preventive interventions to promote appropriate and reasonable working hours are required in our society. Further studies are needed to investigate incident alopecia with an accurate diagnostic tool and other covariates such as genetic characteristics, family history, and type of alopecia.
 XML Download
XML Download