

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Since King et al.1) reported the first percutaneous closure of secundum atrial septal defects (ASDs), the treatment modality has been improved rapidly for 4 decades,2)3) and has become the preferred treatment strategy in most cases now.4)5)6) Many studies have demonstrated that percutaneous closure of moderate sized ASDs is safe and effective.7) Moreover, recent studies reported the good long-term outcomes and lower late complications.8)9) However, the feasibility of a percutaneous approach for very large defects is less clear.
METHODS
Patients and study protocol
A retrospective analysis of patients within a 12-year period, from May 2003 to February 2015, was performed. A total of 1,061 patients underwent percutaneous closure of ASD at Severance Cardiovascular Hospital within this period. Among them, 269 adult patients with large ASD (defined as ASD ≥25 mm) underwent device closure with Amplatzer septal occluder (ASO; St. Jude Medical Inc., Plymouth, MN, USA) were included in this study. This study was approved by the Institutional Review Board of Severance Hospital (No. 4-2015-0418) and the informed consensus was waived due to retrospective nature. The patients were divided into 2 groups according to maximal diameter of ASD, which was measured either by pre-procedural transthoracic echocardiography (TTE) or by intra-procedural transesophageal echocardiography (TEE) or intracardiac echocardiography (ICE). Group 1 (n=216) was patients with large ASD (25 mm≤ASD<35mm) and group 2 (n=53) was patients with very large ASD (35 mm≤ASD). The medical records of these patients were retrospectively analyzed and the demographic and hemodynamic data, immediate post- procedural, early and long-term outcomes were compared in each group. Although there was no decided exclusion criteria, but we usually refer to surgery patients with severe tricuspid regurgitation (TR) and/or extreme large ASD (>42 mm) except one patient.
Peri-procedural transthoracic echocardiography
TTE was routinely performed using Philips® iE33 echocardiography equipment (Philips, Amsterdam, The Netherlands). The anatomic ASD features and relationship between the adjacent structures were fully evaluated. The largest ASD diameter on any view was recorded as ASD size. Right ventricular size and function were assessed to the American Society of Echocardiography.10) Right ventricular systolic pressure was estimated using the Bernoulli equation in patients with TR. In all cases, follow-up TTE was performed in next day after the procedure.
TEE guidance
In our institution, ASD closure was performed with TEE guidance under general anesthesia with endotracheal intubation until June 2006, and thereafter selective cases were performed under TEE guidance for patients with multiple defects or who want general anesthesia. The proportion of TEE guidance was not different between groups after June 2006; 15.0% (8 of 53) in very large ASD vs. 15.3 (27 of 176) in large ASD groups for TEE, Philips® echocardiography equipment (Philips) was used. All echocardiographic examinations were performed according to the recommendations of the American Society of Echocardiography.11)
ICE guidance
After June 2006, ASD closure was routinely performed under ICE guidance using previous described techniques.12) The ACUSON AcuNavTM 8-Fr ultrasound catheter (ACUSON, Issaquah, WA, USA) with an 8- or 8.5-Fr short sheath catheter introducer was used via left femoral vein. The ICE catheter was placed at the right atrium through the femoral vein. After confirming the tricuspid valve at the home view position, the anatomical characteristics were confirmed, steering the probe rightward and posterior to bicaval view and long axis view. ICE views were acquired by guidance according to previously published basic ICE views.13)
ASD closure
Percutaneous closure of the ASD was usually performed via femoral vein under local anesthesia with ICE guidance, and selectively performed under general anesthesia with TEE guidance, and fluoroscopic guidance in all cases. All patients were pre-medicated with acetylsalicylic acid (100 mg). Cardiac catheterization was performed to evaluate the hemodynamic status. Shunt volume was measured by stepwise oximetry measurements of superior and inferior vena cava, and pulmonary artery blood sample using the Fick principle, and expressed as the ratio of pulmonary blood flow to systemic flow (Qp/Qs). For patients with pulmonary arterial hypertension (PAH), criteria for ASD closure were pulmonary vascular resistance <8 WU·m2, and persistent left-to-right shunt. Selective patients with risk factors of coronary artery disease, or had history of stroke or transient ischemic attack underwent coronary angiography. In case of patient with PAH (defined as mean pulmonary artery pressure (mPAP) ≥25 mmHg), PAP was measured again by right cardiac catheterization 20–30 minutes after device detachment. Before entering the left atrium, 5,000 IU of intravenous heparin was injected. Native and balloon occlusive diameter (BOD) using “stop-flow technique” of the ASD were measured by echocardiography, and by fluoroscopy. A size 2 mm greater than the BOD device was generally chosen, except in cases with important discrepancies between the size of the defect on different views, where several sizes of device were attempted and most suitable device was implanted. A long sheath (9 to 12 Fr) was positioned via the ASD into left atrium, usually near the left superior pulmonary vein. With extreme caution for preventing air embolism, the device was introduced through the sheath and deployed under ICE or TEE guidance. After confirming of device position by gentle pull-and-push, “Minesota wiggle” maneuver, the device was released. The position of the device and relationship with adjacent structures were evaluated by ICE or TTE, and by fluoroscopy. Post-interventional treatment consisted of acetylsalicylic acid (100 mg) once daily for 6 months. For peri-interventional prophylaxis, the patients were given 3 doses of cefazolin.
Procedural success was defined as successful ASO delivery without peri-procedural major complications, and well-positioning of the device without migration as assessed by chest X-ray and TTE on the next day. Procedure- or device-related death, cardiac tamponade, erosion, thromboembolism, stroke, complete atrioventricular (AV) block, ventricular arrhythmias were considered major complications. We included vascular damage requiring surgery into major complication. Other any adverse events were regarded as minor complications. Late complications were defined as any adverse events occurred after 6 months from device closure.
Follow-up
A physical examination, 12-lead ECG and chest X-ray were performed 2 hours and the next morning after the procedure. TTE was performed the next day after the procedure in all cases. A physical examination, 12-lead ECG, chest X-ray and TTE were done 1 week, 1, (3), 6, 12 months, and thereafter every one year. Oral antiplatelet drug was prescribed for 6 months, and routine prophylaxis for infectious endocarditis for 6 months in cases without complication. Early complications were evaluated at every visit and late complications were evaluated at any event or at last follow-up.
Statistical analysis
Statistical analysis was performed using SPSS version 21.0 (SPSS, Chicago, IL, USA). Continuous variables are expressed as mean±standard deviation. Variables were compared using Student's t-test or Fisher's exact test, and a p value of <0.05 was considered statistically significant.
RESULTS
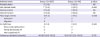
During the period, 1,061 patients were underwent percutaneous closure of ASD. Among them 735 (69.3%) were adult patients (defined as ≥18 years of age), of which 269 (36.6%) patients were adult patients with large ASD. The female-to-male ratio was 2.6, and the mean age was 39.0±14.2 years (range, 16.0–73.0) (Table 1). There were no statistical differences of sex, age, weight, and body surface area between 2 groups. The mean follow-up duration was 43.6±33.1 months (range, 3.0–135.5) without statistical difference between 2 groups.
Table 1
Baseline characteristics of ASD device closure patients (n=269)
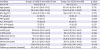
Values are presented as mean±standard deviation (range) or number (%).
ASD = atrial septal defect; BOD = balloon occlusive diameter; BSA = body surface area; mPAP = mean pulmonary arterial pressure; MR = mitral regurgitation; Pul. HTN = pulmonary hypertension; Qp/Qs = the ratio of pulmonary blood flow to systemic flow; TR = tricuspid regurgitation.
*Defined as mPAP≥25 mmHg during catheterization, pre means before device closure and post means after device closure.
Procedural results
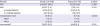
Procedural parameters and outcomes are presented in Tables 2 and 3, respectively. Understandably, defect size, BOD and device size were significant larger in group 2, and the Qp/Qs was also significantly higher in group 2 (2.86±0.82 vs. 3.20±1.00, p=0.009). The maximal diameter of either echocardiographic measurement or BOD in our series was 43 mm, and the ASO sizes of group 2 were as follow; 34 mm (n=1), 36 mm (n=25), 38 mm (n=24) and 40 mm (n=3). The need of modified implantation techniques (MITs) was higher group 2 (23.6% vs. 37.7%, p=0.034). Among MIT, left upper pulmonary vein technique was most commonly applied followed by right upper pulmonary vein technique14) and balloon assisted technique.15)16)17) However, procedural time and fluoroscopy time were not different between 2 groups. Among our 269 patients, 33 (12.3%) had multiple defects which were closed by one device, except one patient underwent percutaneous closure with 2 devices (25 mm and 17 mm). Eleven cases of combined procedure were successfully performed in group 1 without complications.
Table 2
Comparisons of procedural parameters between 2 groups

Values are presented as mean±standard deviation or number (%).
FT = fluoroscopy time; MIT = modified implantation technique; PPV = percutaenous pulmonary valvuloplasty; PT = procedure time;
*PT was defined as time interval from puncture to completion of hemostasis; ‡4 cases of radiofrequency ablations for atrial fibrillation (n=2) and wolff-parkinson-white syndrome (n=2), 3 cases of direct current cardioversions, 1 case of coronary angioplasty.
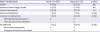
Table 3
Results of device closure
PSR = procedural success rate; RSR = residual shunt rate.
*One case of device migration and 1 case of complete atrioventricular block; †Two cases of device retrieval (1 of device migration and 1 of complete atrioventricular block), and 4 cases of device closure with fenestration due to severe pulmonary hypertension were excluded. All of the flow of the fenestrated atrial septal defect closure remained patent; §Late events were defined as adverse events after 6 months from device closure.
Immediate and short-term procedural successful rate were 99.5% and 99.1%, respectively. One case of device migration to right ventricle was occurred during device closure in group 1. The 34 mm device was removed, and the ASD was repaired surgically. One case of complete AV block was occurred at 2 days after the device closure. The device was retrieved via catheterization.
The residual shunt rate after 3 months follow-up was 0% in single defect in both groups, except 4 cases of closure with fenestrated devices due to pulmonary hypertension. The residual shunt rates of multiple defects after 6 months follow-up were 10% in group 1and 16.7% in group 2.
Hemodynamic results
Associated hemodynamic phenomenon showed conflicted relationship with size groups (Table 1). TR more than grade II was not different in 2 groups and mitral regurgitation (MR) more than grade I was also not different in 2 groups. PAH, defined as mPAP ≥25mmHg during catheterization, was more prevalent in group 2 (25.9% vs. 47.2%, p=0.003), and the mean mPAP was also significantly higher in group 2 (21.8±8.6 vs. 24.6±7.8, p=0.043). However, these statistical differences were disappeared after the device closure. Regarding to hemodynamic changes, TR was improved in 54 (87.1%) patients with TR≥grade II (Figure 1). There was no statistical difference of trend of hemodynamic change between 2 groups, maybe due to small number of significant TR in group 2. In 15 (5.6%) patients, the left atrial disk mildly touched to mitral valve without encroachment. Nevertheless, there was no newly developed MR or mitral valve erosion related with the device.

Early major and minor complications
In our 269 patients, there was no death, stroke and cardiac tamponade. The overall major complication rate was 1.5%, and there was no statistical difference between 2 groups (Table 4). We experienced 2 cases of device migration, one case of femoral arterio-venous fistula, and one case of complete AV block. One case of device migration during procedure was above mentioned, who underwent surgical remove of device and repair of ASD. Another 50-year-old patient, with multiple large ASD (40 mm, 20 mm and 6 mm) with relative short aortic rim (d=6 mm), underwent device closure. Although careful Minesota wiggle was performed, device was migrated to left ventricle after deployment. The device was retrieved via femoral artery access, and another 40 mm ASO was deployed successfully without any complication. One year after the 1st procedure, 2nd 20 mm ASD device closure was performed and resulted in complete closure of all defects. This case was regarded as successful procedure, but as major complication.
Table 4
Major complications of atrial septal defect device closure
One patient underwent repair of right femoral vessels due to arterio-venous fistula. Retroperitoneal hematoma was not occurred.
Regarding to life threatening arrhythmias, there was no ventricular arrhythmia in our case. Above mentioned, one patient complained chest discomfort and dizziness 2 days after device closure with 32-mm ASO. He was diagnosed as complete AV blocks and underwent retrieval of the ASO via catheterization. He was treated with dexamethasone for 7 days and recovered normal sinus rhythm. He underwent surgical repair of ASD and had been doing well without complete AV block.
Most common minor complications were arrhythmias, followed neurological problems. There was no statistical difference between 2 groups (Table 5). Arrhythmias were occurred in similar frequency in both groups (4.2% vs. 5.6%, p=0.238). One case of junctional tachycardia was terminated spontaneously. One case of paroxysmal supraventricular tachycardia and one case of atrial flutter underwent successful radiofrequency ablation (RFA). Nine cases of atrial fibrillation (AF) were treated as below: 4 cases were spontaneously resolved, 3 cases occurred before the deployment of the device underwent direct current (DC) cardioversion followed by successful detachment, and 2 cases were treated with medication as warfarin. Minor neurologic complications were occurred 5 (2.3%) in group 1, and 1 (1.9%) in group 2, respectively. Minor infarction or transient ischemic attack was not occurred. Two cases of migraine were occurred in group 1, and one case of lidocaine toxicity complained of dizziness was occurred in group 2. Three cases of brachial plexopathy due to shoulder traction were occurred in our early experiences related with general anesthesia for TEE guidance. Hematomas were occurred in 4 patients without statistical difference between 2 groups. Allergic reactions were occurred 4 patients in group 1. Three patients experienced contrast-related skin erythema and itching sensation. Suspicious allergic reaction was occurred in previously known nickel-allergy patient. Vague chest discomfort and mild dyspnea was occurred one day after the device closure. Electrocardiography, cardiac enzyme, and chest X-ray were all normal findings. She was treated with antihistamine and low dose steroid, and was observed during 4 days for concerning of delayed hypersensitivity. There was no other event and she had been doing well with the device for 5 years.
Table 5
Minor complications
Late events
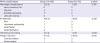
Thirteen patients less than 6 months after percutaneous closure were excluded in this analysis. During long-term follow-up (46±32.1 vs. 52.5±33.1 months, p=0.215), there was no procedure- or disease-related death, device erosion, device fracture, or cardiac tamponade (Table 6). During follow-up, there was one non-cardiac death, 58-year-old female died of cholangiocarcinoma 3 years after the device closure. There was one (0.4%) major adverse event in our study. Middle cerebral infarction was occurred 8 years after device closure in one patient, who had a persistent AF before device closure and had taken a warfarin. Because the extent of infarction was not severe and immediate treatment was taken, he has been well doing without major disability.
Table 6
Late adverse events at least 6 months after atrial septal defect device closure (n=256)
There was no statistical difference of minor late events in both groups. Newly developed migraine headache (3.9%) was most common problem, followed by AFs (1.9%). Patients with AFs were treated as below; one was spontaneously resolved, one treated with medical treatment, 2 patients treated with DC cardioversion resulted in normal sinus rhythm in one case, while other patient treated subsequent RFA resulted in normal sinus rhythm.
DISCUSSION
In our study, percutaneous closure of very large ASD proved safe and effective as well as large ASD did. There is no universal definition of large ASD, thus the interpretation of success rate of percutaneous closure of large ASDs needs caution. Varma et al.14) reported 91% success rate in 34 large ASD patients using a definition of large>25 mm (mean 30±3 mm) diameter on balloon stretched diameter (BSD). Rodríguez et al.18) reported 74% success rate in 31 large ASD patients using a definition of large>30 mm (mean 33±3.4 mm, range, 30–40 mm) diameter on BSD. Romanelli et al.19) reported 97% success rate in 36 large to very large ASD patients, defined as maximal pre-procedural TEE ASD diameter in the range 20–39 mm, while only 17% in 6 extreme large ASD patients (≥40 mm). Recently, Baruteau et al.20) reported the largest study of the feasibility and safety of percutaneous closure in both adult and pediatric large ASD patients. Using a definition of large≥34 mm on BSD in 175 adults, they reported 89.7% successful rate. In our study, the procedural success rate was 99.1% in large ASD group and 100% in very large ASD group. It is one of the highest successful rates, with acceptable major complication rate of percutaneous closure using ASO for large ASD patients. In our study, there was no cardiac death and the early and late major complication rate was 1.5%. This is consistent with previous studies not focused large ASDs.2)7)9) Abaci et al.21) reported 1.0% of peri-procedural major complication of percutaneous closure of ASD in 13,526 patients by their meta-analysis, including 0.7% of device embolization.
In our study, 2 cases (0.7%) of device migrations were treated via catheterization (n=1) or surgery (n=1) without further complications. Although extreme caution to avoid device migration is essential, we agree with Baruteau et al.20) that the morbidity related with ASO migration is rare and easily managed without complication. A recent multicenter cohort study reported that ten devices (1.5%) embolization were treated successfully via catheterization (n=7) or surgery (n=3) without further complications.22) Large ASDs with posterior or inferior rim deficiency were known the risk factors for device migration.23)24) In our study, the procedural success rate using the 40 mm ASO was excellent; 3 of 3 patients, although one patient with multiple ASDs complicated device embolization described before who finally underwent successful device closure. However, we did not found any association between rim deficiency and device migrations, which might be due to small case of migration. We suggested that percutaneous closure of the extreme large ASDs could be attempted in experienced center as others reported.19)25)
We experienced one case of complete AV block above mentioned. The exact mechanism of complete AV block after percutaneous closure of ASD is not clear. Mechanical pressure on AV node may result in inflammatory response and could lead to AV block.26) Although, there had been report of spontaneous resolution or successful treatment with steroids,27) it is usually recommended that surgical or percutaneous removal of the devise, when the block was not resolved in one week.8)
For vascular complications, there were no relationship between intra-procedural echocardiographic modalities and vascular complications, although one more venous access was required for ICE guidance. This was consistent with our previous report of the safety of ICE guidance including small children.12)
After a median follow-up of 48 months, there was no cardiac death, and no long-term major complication was occurred, except one case (0.4%) of stroke in above-mentioned patient with permanent AF. Long-term follow-up data reported 0.4% of cerebrovascular events, 0.1% of device embolization, 0.1% of device erosion and 0.1% of device related death.21) Our study showed the incidence of AF after percutaneous closure of ASD as 5.5% (3.7% in early and 1.8 in late), which was higher than previous report not focused on arrhythmias,2)21) although most of AFs were resolved spontaneously or medically well treated as other reported.20) However, a recent study focused on AF and stroke showed a higher incidence rate of 11.8% after ASD closure and higher risk of stroke even after ASD closure which was related with AF,28) although the incidence rate of AF was 23.7 in unclosed ASD patients. ASD closure could reduce the incidence of atrial tachycardia.29) Nevertheless, comprehensive evaluation and long-term follow-up of atrial tachycardia is necessary, thus we routinely performed 24-hour Holter monitoring in adult large and elderly ASD patients. In this article, we did not analysis of pre-existed atrial tachycardia.
For migraine headache, we reported 4.4% of incidence (0.7% in early and 3.7% in late) after percutaneous closure, which is compatible to a study focused on migraine headache after transcathter closure of ASD and patent foramen ovale.30) While other previous studies, which conducted all complication in together, reported lower incidence of migraine headache. Other reports supported new onset of migraine headache after percutaneous closure of ASD,31)32) whereas percutaneous closure of ASD resulted in significant reduction of migraine headache.
There was gap of incidence of atrial tachycardia, migraine headache between studies focused on the complications and studies did not. Thus, further investigation for these complications is warranted.
Our study showed the co-incidence of moderate TR was approximately 23% and it of mild-to-moderated MR was 15% without statistical difference between 2 size groups. The TR was improved in most (87.1%) cases, which may reflect the reduction of right atrial and ventricle size.33)34) Our study showed that percutaneous closure of large ASD with moderate TR was effective for both anatomic and hemodynamic results. However, we preferred surgical treatment in large ASD with severe TR (grade IV), thus further investigation for these patients is still needed.
PAH assessed by cardiac catheterization was more prevalent in very large ASD group, however, this phenomenon was disappeared after the device closure. This showed that the hyperkinetic pulmonary blood flow is not sole mechanism of development of PAH, and multifactorial factors were related with PAH.35) Nevertheless, early transcatheter closure of large ASD is important because mild-to-moderate PAH could be reversed without permanent PAH. In our study, the incidence of residual PAH was approximately 20% after percutaneous closure, which was higher than previous reports,35)36)37) may be related that we evaluated the PAH with cardiac catheterization rather than echocardiography using the estimated right ventricular systolic pressure, and our patient had large ASD than other study did. We planned further investigation of detailed hemodynamic status of ASD percutaneous closure with our various clinical groups.
This was a non-randomized retrospective study with its inherent limitations. The number of device migration was small, thus we could not analyzed the risk factors in our study. Detailed analysis of hemodynamic assessment was not performed, and the comprehensive evaluation of quality of life or survey for migraine headache was not obtained. Cardiopulmonary function tests were performed in recent cases, thus we did not include the analysis in this study.
Nevertheless, our study is one of the largest studies for percutaneous closure of adult large ASD patients with detailed information of various complications, which were usually not mentioned in other articles. Long-term follow-up is mostly achieved in our patients, thus our data could show comprehensive information about long- term events and hemodynamic changes.
In conclusion, our study demonstrated the effectiveness and safety of transcathter closure in very large ASD patients as well as large ASD patients. The procedural success rate was 99.1% in large ASD group and 100% in very large ASD group with acceptable early (1.5%) and late (0.4%) major complication rate. Long-term follow-up of transcathter closure of large ASD is important, especially for late complication and hemodynamic results. And lastly further investigation of extreme large ASD using 40 mm ASO is still needed.
 XML Download
XML Download