

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Primary percutaneous coronary intervention (PPCI) is now the standard treatment strategy in patients with ST-segment elevation myocardial infarction (STEMI). Although PPCI has been reducing the risk of acute myocardial infarction (AMI)-related heart failure (HF),1) symptomatic HF can develop in patients with STEMI even after early reperfusion therapy and medical treatment and contributes to poor prognosis.2) Measurement of global longitudinal strain (GLS) and global circumferential strain (GCS) by 2-dimensional speckle tracking echocardiography (2D STE) is a novel method that has been suggested to have superiority over left ventricular ejection fraction (LVEF) in evaluation of ventricular systolic function. This study was conducted to investigate the usefulness of parameters of myocardial deformation, GLS, GCS, and mean longitudinal strain of left anterior descending artery territory (LSant), the average longitudinal strain of left ventricular (LV) segments supplied by left anterior descending (LAD) artery, measured by 2D STE in prediction of HF in patients with anterior wall STEMI (ant-STEMI) successfully treated with PPCI in comparison with LVEF and biomarkers including N-terminal pro-brain natriuretic peptide (NT-proBNP) and troponin.
METHODS
Subjects
We reviewed medical records of 543 patients who were diagnosed with ant-STEMI and underwent PPCI successfully at proximal or middle LAD artery at Chonbuk National University Hospital from January 2008 to December 2016. Two-dimensional echocardiographic study was performed within 48 hours after percutaneous coronary intervention (PCI) in all patients using machines from a specific vendor because GLS values can significantly vary depending on the study time point after AMI3) or on the software from different vendors.4) Patients with prior history of symptomatic HF, prior history of myocardial infarction (MI) or angina, in-hospital death during index hospitalization, final thrombolysis in myocardial infarction (TIMI) flow grade <3 of the culprit lesion at the end of the procedure, or significant (≥moderate) organic valvular dysfunction were excluded. After primary elimination of 298 patients based on these criteria, 74 patients were additionally excluded because their echocardiographic images were not analyzable due to low frame rate or poor quality. A total of 171 patients with eligible echocardiographic data were eventually enrolled to the study (Figure 1). The study protocol was approved by the local ethics committee of the Institutional Review Board of Chonbuk National University Hospital (IRB No. 2018-10-016) and written informed consent was waived because the study was retrospective and anonymous clinical data were used for analysis.
Figure 1
A flow chart showing the number of patients excluded, the reasons for exclusion and 3 groups in this study.
HF = heart failure; LAD = left anterior descending artery; PCI = percutaneous coronary intervention; RWMA = regional wall motion abnormalities; STEMI = ST-segment elevation myocardial infarction.

Definition and classification of heart failure associated with anterior wall ST-segment elevation myocardial infarction
Patients with ant-STEMI-related HF was divided into 2 categories according to the timing of development: in-hospital and post-discharge HF. Group 1 (in-hospital HF) included patients with signs of HF, rales or pulmonary edema (Killip classification II and III) at the time of admission or during hospitalization after PCI. Patients in Group 1 were subdivided into HF at the time of admission (Group 1A) and new HF after PPCI (Group 1B). Among those who did not develop in-hospital HF, patients who experience HF after discharge were assigned to Group 2 (post-discharge HF). Group 2 involved patients who were discharged without signs of HF at the time of discharge and visited emergency room (ER) or were re-hospitalized due to dyspnea with signs of HF and elevated level of NT-proBNP (≥150 pg/mL for patients aged ≤74 years, ≥450 pg/mL for patients aged ≥75 years) at any time after discharge. Group 3 included patients who did not experience HF during index hospitalization or after discharge. The verification of HF development or hospitalization was performed by an independent reviewer blinded to echocardiographic information.
Clinical and procedural data
Patient demographic data, atherosclerotic risk factors, procedural characteristics, and laboratory data were collected based on the medical records. Patients who were lost during follow-up were called to confirm the occurrence of clinical events. Chest pain-to-ER visit time was defined as the time from onset of chest pain to the contact to our ER. Successful PCI was defined as residual diameter stenosis <30% and TIMI flow grade 3 of the culprit lesion at the end of the procedure. No reflow phenomenon was defined as a transient or persistent TIMI flow grade 0 or 1 after relief of coronary occlusion without angiographic evidence of mechanical obstruction.
Echocardiographic assessment
Two-dimensional echocardiography was performed using a Vivid 7 (GE Vingmed Ultrasound, Horten, Norway) or Vivid q (GE Medical Systems, Haifa, Israel) echocardiography machine with an M4S probe in all study patients. LV dimensions, volumes, and ejection fraction were measured according to the recommended guidelines from American Society of Echocardiography and European Association of Echocardiography.5) Wall motion score index (WMSI) of the LV was analyzed using a 17-segment model. Indexing of modified Simpson formula-derived LV volumes was performed to body surface area for left ventricular end-diastolic volume index (LVEDVI) and left ventricular end-systolic volume index (LVESVI). Mitral regurgitation (MR) was evaluated by distal jet area using color Doppler study and effective regurgitant orifice area using the proximal isovelocity surface area method and MR ≥grade 2 was considered significant. Right ventricular systolic pressure (RVSP) was calculated based on the peak velocity of tricuspid regurgitation and respiratory collapsibility of the inferior vena cava.
Two-dimensional speckle tracking echocardiography processing and analysis of strain
Measurement of GLS was performed as an offline analysis of digitally stored cineloop images at a remote workstation (EchoPAC BT 201.54.0; GE Vingmed Ultrasound, Horten, Norway) using a semiautomated software (Automated Function Imaging; AFI) by 2 experienced operators (S. H. Lee and W. H. Kim) who were blinded to patients' clinical information and the mean of the 2 measured values was used. For measurement of GLS, three apical images were selected and a region of interest (ROI) was automatically tracked for each of the 3 images by the software. Position of the ROI was manually adjusted if automatic tracking was not satisfactory. The software generated longitudinal strain curves for each of 17 segments, a color-coded bull's eye plot image, and a calculated value of GLS from the average of peak longitudinal strain values of 17 segments (Figure 2). For measurement of GCS, a mid-LV level image at parasternal short axis view using the papillary muscles as an anatomical landmark was obtained. A value of GCS was automatically calculated by the software from the average of peak circumferential strain values of 6 segments. In case of unsatisfactory tracking even after adjustment of the trace line, the segments were excluded from the analysis. If GLS was not available because of insufficient tracking of speckles in more than three segments, the patient was excepted from the study. The LSant was defined as the mean peak systolic longitudinal strain of the 11 segments supplied by LAD and calculated by the operator using the bull's eye plot image (Figure 3).
Figure 2
Measurement of GLS and LSant using two-dimensional speckle tracking echocardiography. (A-C) A region of interest is semiautomatically tracked in each of 3 apical images and software generates longitudinal strain curves for each 17 segments. (D) Note a bull's eye plot image and GLS.
GLS = global longitudinal strain; LAD = left anterior descending artery; LSant = mean longitudinal strain of left anterior descending artery territory.

Figure 3
Bull's eye image plots in 2 contrastive cases of with ant-STEMI, the same LVEF of 48%, and single vessel disease on coronary angiography. Note the differences between (A) a 73-year-old man with GLS of −9.7% (LSant, −2.5%) who experienced in-hospital HF and (B) a 46-year-old man with GLS of −16.1% (LSant, −10.5%) without signs of HF.
ant-STEMI = anterior wall ST-segment elevation myocardial infarction; GLS = global longitudinal strain; HF = congestive heart failure; LSant = mean longitudinal strain of left anterior descending artery territory; LVEF = left ventricular ejection fraction.

Statistical analysis
Continuous variables were presented as mean ± standard deviation and categorical variables as percentages (%). The Chi-square test was used for between-group comparison of categorical variables. A Kruskal-Wallis test and Mann-Whitney test with Bonferroni correction for post hoc analysis were used for continuous variables. Laboratory variables such as high-sensitivity C-reactive protein (hs-CRP) and NT-proBNP were incorporated into the model as a continuous variable. Absolute values were used for statistical analyses of strain values including GLS, GCS, and LSant. Univariate and stepwise backward multivariate logistic regression analyses were separately used to determine the factors associated with the development of in-hospital and post-discharge HF. All variables significant on univariate analyses with a p value <0.05 in group-to-group comparison were submitted for multivariate analysis. The PASW Statistics 18.0 for Microsoft Windows® (SPSS Inc. Chicago, IL, USA) was used for statistical analyses. In all cases, p values <0.05 were considered statistically significant. The predictive power and the best cut-off values of GLS and LSant for in-hospital and post-discharge HF were respectively determined in comparison to LVEF and level of NT-proBNP on receiver operating characteristic (ROC) curve analysis using the MedCalc for Windows, version 18.11.3 (MedCalc Software, Ostend, Belgium).
RESULTS
Study population
Mean age of overall patients was 62±13 years and 72.5% were male. Median follow-up period was 31.6 (mean, 98.9±76.6) months. In-hospital HF developed in 39 patients (22.8%). Among 132 patients who did not have HF during index hospitalization, 13 patients (9.8% [13/132], 7.6% of overall patients [13/171]) experienced HF during follow-up after discharge. In the total of 171 patients, the segmental feasibility of GLS measurement was 95.0%. Inter-observer and intra-observer variability for overall strain measurement was 0.88 and 0.92, respectively.
Baseline clinical and laboratory findings
Baseline demographic characteristics were comparable except age and history of smoking. Mean age of patients in Group 2 was significantly higher than those in other two groups (65±13 vs. 69±12 vs. 60±13 years, p=0.029). Smokers were more prevalent in Group 3 than in Groups 1 and 2 (38.5% vs. 38.5% vs. 59.7%, p=0.038). The levels of NT-proBNP and hs-CRP were significantly higher in Group 2 and in Group 1 than the other 2 groups, respectively (Table 1). Peak troponin I levels were comparable in the 3 groups.
Table 1
Comparison of characteristics of ant-STEMI patients according to development of heart failure
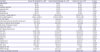
ant-STEMI = anterior wall ST-segment elevation myocardial infarction; ER = emergency room; GCS = global circumferential strain; GLS = global longitudinal strain; HF = heart failure; hs-CRP = high-sensitivity C-reactive protein; LSant = longitudinal strain at of left anterior descending artery territory; LVEDVI = left ventricular end-diastolic volume index; LVEF = left ventricular ejection fraction; LVESVI = left ventricular end-systolic volume index; MR = mitral regurgitation; NT-proBNP = N-terminal pro-brain natriuretic peptide; RVSP = right ventricular systolic pressure; TIMI = thrombolysis in myocardial infarction; WMSI = wall motion score index.
*p<0.05.
Echocardiography for strain analysis was 1.5±1.1 days after PPCI. The strain values showed significantly different values in the three groups. GLS (−10.63±2.93% vs. −12.11±2.24% vs. −13.51±3.30%, p<0.001) and GCS (−8.61±3.55% vs. −11.59±2.89% vs. −12.11±3.68%, p=0.004) were more prevalently impaired in Group 1. LSant was depressed in both HF groups, Group 1 and Group 2, compared to non-HF group (−6.22±4.69% vs. −5.49±5.17% vs. −9.48±5.44%, p=0.001).
In addition to strain parameters, patients in Group 1 and Group 2 showed poorer LVEF, higher WMSI, LVESVI, and E/E′ ratio, more significant MR, more elevated RVSP, and more extensive coronary artery disease than those of Group 3 (Table 1). Chest pain-to-ER visit time, door-to-balloon time, and frequencies of initial TIMI flow grade 0 and no reflow phenomenon during the procedure were comparable.
Among 39 patients in Group 1, 56.4% (n=22) presented with symptoms or signs of HF at the time of admission (Group 1A) and the remained 43.6% (n=17) developed HF after admission (Group 1B). Patients in these two subgroups were indistinguishable in demographic, laboratory, procedural, and echocardiographic characteristics (see the Supplementary Table 1). The development of post-discharge HF was widely distributed from 1 month to 8 years after ant-STEMI. Mean level of NT-proBNP at the diagnosis of post-discharge HF was 5,007.6±4,835.6 pg/mL.
Post hoc analysis for group-to-group comparison
Table 2 demonstrates the result of post hoc analysis for group-to-group comparison. Levels of NT-proBNP and hs-CRP, traditional echocardiographic parameters including LVEF, WMSI, LVESVI, E/E′ ratio, RVSP, and significant MR, history of smoking and number of diseased vessels showed significant differences between in-hospital-HF and no-HF groups. Patients with post-discharge HF were different in age, levels of NT-proBNP and hs-CRP, E/E′ ratio, and RVSP compared to those of no-HF group.
Table 2
Post hoc analysis* of parameters for group-to-group comparison in patients with ant-STEMI
ant-STEMI = anterior wall ST-segment elevation myocardial infarction; GCS = global circumferential strain; GLS = global longitudinal strain; HF = heart failure; hs-CRP = high-sensitivity C-reactive protein; LSant = longitudinal strain of left anterior descending artery territory; LVEDVI = left ventricular end-diastolic volume index; LVEF = left ventricular ejection fraction; LVESVI = left ventricular end-systolic volume index; MR = mitral regurgitation; NT-proBNP = N-terminal pro-brain natriuretic peptide; RVSP = right ventricular systolic pressure; WMSI = wall motion score index.
*Mann-Whitney test was used for post hoc analysis; †p<0.05.
As regards strain values, GLS and GCS were significantly depressed in Group 1 compared to Group 3. LSant was the only strain parameter that showed discrepancy between Group 2 and Group 3. GLS and GCS values were impaired in both HF groups, Group 1 and Group 2, compared to Group 3 but they showed far more depression in Group 1 than in Group 2 (Table 2).
Predictors of in-hospital and post-discharge heart failure
In multivariate analysis to identify predictors of in-hospital HF using GLS, LSant, GCS, LVEF, WMSI, LVESVI, significant MR, RVSP, number of diseased vessels, and history of smoking, all of which were proved to be of significance in univariate analysis, GLS was the only and the strongest predictor remained statistically significant (odds ratio [OR], 1.853; 95% confidence interval [CI], 1.207–2.846; p=0.005), and RVSP showed borderline significance (Table 3).
Table 3
Univariate and multivariate logistic regression analyses for prediction of in-hospital and post-discharge HF in patients with ant-STEMI

ant-STEMI = anterior wall ST-segment elevation myocardial infarction; CI = confidence interval; GCS = global circumferential strain; GLS = global longitudinal strain; HF = heart failure; hs-CRP = high-sensitivity C-reactive protein; LSant = longitudinal strain of left anterior descending artery territory; LVEF = left ventricular ejection fraction; LVESVI = left ventricular end-systolic volume index; MR = mitral regurgitation; NT-proBNP = N-terminal pro-brain natriuretic peptide; OR = odds ratio; RVSP = right ventricular systolic pressure; WMSI = wall motion score index.
*p<0.05.
For prediction of post-discharge HF, multivariate analysis including age, LSant and E/E′ ratio showed that and LSant was the only independent factor associated with post-discharge HF (OR, 1.143; 95% CI, 1.006–1.298; p=0.040).
Discriminatory power of strain in prediction of heart failure
ROC curve analysis to predict in-hospital HF using the area under the curve (AUC) displayed the AUCs for GLS of 0.753 (95% CI, 0. 682–0.816; p<0.001), for LVEF of 0.735 (95% CI, 0.662–0.800; p<0.001) and for NT-proBNP of 0.600 (95% CI, 0.516–0.679; p=0.072) (Figure 4A). The predictive power of GLS for in-hospital HF was significantly superior than that of NT-proBNP (p=0.012) and comparable with LVEF (p=0.532). The best cut-off value of GLS was −10.9% which achieved a sensitivity of 69.2% and a specificity of 76.5% to predict in-hospital HF. For prediction of post-discharge HF, LSant (AUC, 0.715; 95% CI, 0.630–0.790; p=0.010) and NT-proBNP (AUC, 0.720; 95% CI, 0.628–0.801; p=0.005) were comparably fair (p=0.585), but LVEF was not discriminatory (AUC, 0.643; 95% CI, 0.555–0.725; p=0.055) (Figure 4B). The LSant cut-off value of −2.36% achieved a sensitivity of 53.9% and a specificity of 89.1% in prediction of post-discharge HF.
Figure 4
ROC curves testing and comparing values of GLS and LSant versus LVEF and NT-proBNP in predicting in-hospital and post-discharge HF in patients with ant-STEMI. (A) The AUC of GLS was 0.753 (95% CI, 0.682–0.816; p<0.001) which was comparable (p=0.532) with LVEF (AUC, 0.735; 95% CI, 0.662–0.800; p<0.001) and significantly higher (p=0.012) than that of NT-proBNP (AUC, 0.600; 95% CI, 0.516-0.679; p=0.072) to predict in-hospital HF. (B) In prediction of post-discharge HF, LSant (AUC, 0.715; 95% CI, 0.630–0.790; p=0.010) and NT-proBNP (AUC, 0.720; 95% CI, 0.628-0.801; p=0.005) were comparable (p=0.585), but LVEF showed poor discriminatory power (AUC, 0.643; 95% CI, 0.555–0.725; p=0.055).
ant-STEMI = anterior wall ST-segment elevation myocardial infarction; AUC = area under the curve; CI = confidence interval; GLS = global longitudinal strain; HF = heart failure; LSant = mean longitudinal strain of left anterior descending artery territory; LVEF = left ventricular ejection fraction; NT-proBNP = N-terminal pro-brain natriuretic peptide; ROC = receiver operating characteristic.

DISCUSSION
The major findings of this current study are as follows: 1) the frequency of in-hospital and post-discharge HF in patients with ant-STEMI successfully reperfused with PPCI was 22.8% and 7.6%, respectively; 2) GLS and LSant measured by 2D STE were significantly correlated with development of in-hospital and post-discharge HF, respectively; 3) strain parameters surpassed the discriminative power of LVEF in prediction of HF; and 4) the well-known indicators of HF including LVEF and NT-proBNP were of less significance than strain values.
The incidence of AMI-associated acute HF has been variably reported between 18% to 29%, which is in accordance of our study, mainly according to the characteristics of patients, types of AMI, treatment strategies, and location of infarct.6)7) In a previous study by Santoro et al.,6) among 2,089 patients with AMI-associated acute HF of 18%, most patients (17%) presented HF at the time of hospital admission and the remaining 1.3% developed HF after admission, whereas 56.4% presented HF at admission and 43.6% developed during hospitalization in our study. The difference in the timing of HF development from our study can be explained by the difference in patient population because only 47.3% of patients had anterior wall Q-wave MI, 83.9% underwent PCI, and 10.9% had a history of prior MI in the study by Santoro et al.6)
Reported incidence of HF following AMI during the long-term follow-up period ranges from 8.6% to 10.3%.7) A recent study8) including patients with STEMI treated with PPCI described the incidence of HF hospitalization as low as 4% for 21±13 months. Another study9) only involving in patients with ant-STEMI presented the incidence of HF of 10% during 18.3±9.0-month follow-up, which shared similarities in study population, follow-up duration, and the incidence of long-term HF with our study.
We have assigned patients with HF related to ant-STEMI into in-hospital and post-discharge HF according to the time point of HF development. Diabetes, age, anterior location, prior history of MI, baseline TIMI 0 flow, peak troponin or creatine kinase, heart rate, extensive coronary disease, delayed admission, and LVEF have been suggested as predictors for acute HF following AMI.2)6)10) Our study enrolled patients with ant-STEMI, a high-risk subgroup of AMI-related HF, and showed that GLS, LVEF, LSant, GCS, WMSI, LVESVI, significant ischemic MR, and number of diseased coronary vessels were associated with in-hospital HF in this population denoting more severe coronary artery disease and more extensive infarct. We also showed that GLS was the only independent predictor of in-hospital HF. There have been few studies examining the risk factors for acute HF and limited study population to ant-STEMI, but strain has rarely been tested as a predictor of ant-STEMI-related acute HF.11)
Few studies have described the risk factors for late-onset HF after AMI. Lewis et al.12) reported that age, diabetes, prior history of MI, and impaired renal function were related to development of HF in post-MI patients. In our study, age, LSant and E/E′ ratio were associated with post-discharge HF and LSant was the only independent predictor. However, NT pro-BNP was not related to in-hospital nor post-discharge HF although it has been known to be one of the prognostic indicators of AMI.13)
GLS has been emerging as a useful tool in detection of subclinical LV dysfunction in patients with normal LVEF as well as in prediction of cardiovascular outcome in patients with normal or reduced LVEF.14)15)16)17) Longitudinal fibers of the subendocardial layer are susceptible to ischemic injuries and GLS is determined by longitudinal deformation of the LV, reflects the early changes in subendocardial longitudinal function, and is more dependent on the movement of apical segments than base. Therefore, it can reflect acutely deteriorated LV systolic function caused by infarcted myocardium of the LAD territory more sensitively than LVEF.
In patients with AMI, GLS has been suggested to be able to manifest infarct size18)19)20) and level of NT-proBNP21) in acute phase and to predict myocardial functional recovery,22)23)24) adverse LV remodeling,25)26)27) and adverse clinical outcome during post-MI long-term follow-up period.8)28) However, there have been few studies examining the relationship between GLS and development of acute HF in patients with ant-STEMI. Although Ersbøll et al.11) described that GLS was the strongest independent predictor of in-hospital HF in patients with AMI, which was consistent with the result of our study, STEMI accounted for only 67.5%, PPCI was performed in 60.8%, and LAD was the culprit vessel in 38.1% in their study. This current study is unique because it ascertained the prognostic implication of GLS for prediction of in-hospital HF in a high-risk AMI population, patients with ant-STEMI.
In survivors with a history of AMI, age and LVEF have been reported to be predictors of late-onset HF29) and involvement of LAD as culprit vessel is one of the negative predictors of recovery of LV function.3) In this study, 11-segment LSant was an independent predictor of post-discharge HF in patients with ant-STEMI suggesting that LSant can reflect the potential for late recovery more accurately in patients with ant-STEMI than other echocardiographic parameters including LVEF and GLS. Although GLS can be progressively restored after AMI with recovery from myocardial stunning, infarcted myocardium undergoes adverse remodeling in 30% to 35% of patients after ant-STEMI due to chronic and excessive neurohormonal activation,26) which can explain late-onset HF after AMI. The result of the current study suggests that residual myocardial scarring and dysfunction of the infarcted segments which can lead to post-discharge HF during long-term follow-up can be better reflected by impaired LSant than by other factors including LVEF or GLS in patients who experienced ant-STEMI.
LSant was one of the two independent predictors of post-discharge HF and the cut-off value of −2.36% was discriminative. Several studies have shown the relationship between strain of infarct zone and functional recovery of the LV or clinical outcome in patients with AMI.20)22)23) Antoni et al.8) described that not only GLS but also strain of the infarct zone was independently associated with all-cause mortality after AMI during follow-up for 21±13-months. A small study involving patients with ant-STEMI treated with PPCI suggested LSant as the only independent predictor of LV functional recovery with the best cut-off value of −6.13%.24) Another small study showed that 7-segment anterior strain assessed by speckle tracking echocardiography and Doppler tissue imaging was a significant predictor of adverse long-term outcome including HF and HF death after PPCI for ant-STEMI.9) Jang et al.30) showed that GLS was more sensitive in patients with ant-STEMI than in those with non-ant-STEMI for prediction of 2-year clinical outcome including all-cause mortality and HF hospitalization in STEMI patients treated with PPCI but did not study LSant as a long-term prognosticator. Characteristics of study population of the two studies involving LAD were quite similar except that follow-up duration of our study was substantially longer (median, 31.6; mean, 98.9±76.6 months).
There are some limitations to our study. This is a retrospective and single-center study. Scheduled measurement of echocardiography and level of NT-proBNP and troponin, and clinical follow-up were not performed. However, we rejected all patients whose images were not suitable for analysis to minimize the inclusion of inadequate images. Patients who had severe HF and died immediately after admission or during index hospitalization were excluded from this study because 2D STE could not be performed in some of them due to their critical medical condition. Patients with inadequate echocardiographic image quality for analysis of strain and those who did not undergo echocardiography machines from a specific vendor were also excluded. It may have introduced a selection bias and underestimated the incidence of acute in-hospital HF, but not all mortality of excluded patients might result from STEMI-related HF. Statistical significance can be underpowered due to a relatively small number of patients with in-hospital and post-discharge HF. A prospective study with larger population can assess further whether routine assessment of GLS and LSant improves risk prediction in this patient population.
In conclusion, the present study described the prognostic implication of myocardial strain in prediction of HF in patients with ant-STEMI successfully treated with PPCI. GLS was a significant predictor for in-hospital HF and LSant was an independent prognosticator for post-discharge HF. These strain parameters showed superiority over LVEF, NT-proBNP, and troponin in prediction of HF. Although current treatment guidelines for AMI recommend the LVEF as a representative value of LV systolic function, measurement of myocardial strain, including GLS and LSant, using a semiautomated software, can provide additional prognostic information.
 XML Download
XML Download