

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Intravascular stenosis occurs in many kinds of congenital heart disease congenitally or after an attempted surgical repair. Vascular stenosis such as pulmonary artery stenosis, particularly branch pulmonary artery stenosis, coarctation of the aorta, or right ventricular outflow tract obstruction could be the cause of significant morbidity or mortality. Although percutaneous balloon angioplasty has been mainly used to dilate narrowed vessels in pediatric patients, recoiling occurs frequently. Balloon expandable stents have been used among patients with congenital heart disease to prevent recoiling and sustain the relief of obstructive lesions. However, there are only a limited number of sizes and types of balloon expandable stents in our country, and it is not easy to use the available balloon expandable stents in vascular stenosis in moderate to large-sized vessel.
Recently, a few studies reported the use of self-expandable stents in vascular stenosis in various kinds of congenital heart disease.1)2)3)4) However, limited data on the efficacy and safety of these stents in moderate to large-sized vascular stenosis are available, especially in our country. In this study, we described the early and intermediate-term outcome and complications following self-expandable stent implantation in moderate to large-sized vessel in congenital heart disease.
METHODS
Patients
The Institutional Review Board of Korea University Ansan Hospital approved this study (Approval Number: 2019AS0041). A total of 12 self-expandable stents were placed among 9 patients (7 males, 2 females) between February 2012 and January 2019. Informed consent was obtained from all patients prior to performing the procedure. The median age of the patients at catheterization was 12 years (range, 4–39 years), and the median weight was 38 kg (range, 19–69 kg). The patient's demographic data and underlying diagnosis are shown in the Table 1. Two patients previously underwent Fontan operations for complex congenital heart disease. There were multiple stenoses in the anastomosis line between the pulmonary artery and previously placed modified Blalock–Taussig shunt in 1 patient. Moreover, diffuse narrowing of the left pulmonary artery (LPA) was observed in the other Fontan patient. In 3 patients with tetralogy of Fallot (TOF) and double outlet right ventricle (DORV), self-expandable stents were placed to dilate the stenosed LPA. In 1 patient with unilateral absence of the right pulmonary artery (RPA), the stenosis was at the anastomosis site between the native pulmonary artery and conduit. Furthermore, 1 patient previously underwent Rastelli operation for complex pulmonary atresia (PA) with ventricular septal defect (VSD), and severe stenosis in the right ventricle to pulmonary artery (RV-PA) conduit was noted. One patient who underwent coarctoplasty in infancy had postoperative recurrent coarctation. Finally, 1 patient had severe RPA narrowing after surgical repair.
Table 1
Characteristics of patients with self-expandable stents

DORV = double outlet right ventricle; PA = pulmonary atresia; RPA = right pulmonary artery; TGA = transposition of great arteries; TOF = tetralogy of Fallot; UAPA = unilateral absence of pulmonary artery; VSD = ventricular septal defect.
![]()
Methods
The interventional catheterization was conducted under general or local anesthesia. All patients received prophylactic antibiotic therapy prior to catheterization. After percutaneous puncture of the femoral artery and vein, all hemodynamic variables were evaluated. Following hemodynamic assessment, angiogram in the pulmonary artery or aorta was performed to delineate the stenotic vascular segment. Then, a catheter was placed in the stenotic lesion. A stiff guide wire was advanced through the well-positioned catheter, and the tip of the stiff wire was placed in the distal branch of the vessel. Balloon dilations were performed among patients to ascertain that the stenoses were dilatable prior to self-expandable stent implantation. A Hercules self-expandable vascular stent (S&G Biotech, Seoul, Korea) was implanted in all patients. It is made of 2 nitinol wires in a tubular configuration. Its mean radial force is 0.94 Newton, and it has soft ends and good flexibility. The stent diameter was about 10% or 20% greater than the diameter of the proximal and distal vessel. The stent length was between 30 mm and 40 mm (36.7±4.9 mm). Following balloon dilations, the self-expandable stent was loaded over a stiff wire passing through the stenotic lesion. The exact position of the stent was confirmed by angiogram via a separate angiographic catheter. The stent was then fully uncovered and deployed by withdrawal of the shaft of the Hercules self-expandable stent catheter, and the deployed stent was expanded to the wall of the vessel. After stent implantation, angiography was repeated and the systolic pressure gradient in the stenotic segment was assessed. Systemic heparinization was administered to all patients during procedures, and oral aspirin was taken for 6 months after stent implantation. Oral warfarin was continued for patients who previously underwent Fontan operations.
RESULTS
A total of 12 self-expandable vascular stents have been implanted among 9 patients. The mean stent diameter and length were 16.0±3.7 mm (range, 10–22 mm) and 36.7±4.9 mm (range, 30–40 mm), respectively. The narrowest diameter of the stented vessel increased from 5.7±3.2 mm (range, 2.9–11.0 mm) to 12.6±3.4 mm (range, 6.4–17.2 mm; p<0.05). The mean pressure gradient across the stenotic lesion decreased from 23.0±28.2 mmHg (range, 2–95 mmHg) to 3.2±3.6 mmHg (range, 0–10 mmHg; p<0.05, Table 2).
Table 2
Comparison between pre- and post-stent implantation
Values are presented as mean±standard deviation.
F/up = follow-up; LPA = left pulmonary artery; RPA = right pulmonary artery; RV-PA = right ventricle to pulmonary artery.
![]()
The patients were followed-up for a median of 43 months (range, 1–83 months). In 1 patient with stenosis at the RV-PA conduit, significant narrowing occurred in the stent which had been placed in RV-PA conduit stenosis. One procedure was complicated by distal migration of the self-expandable stent in the LPA, resulting in an inaccurate placement, which had been managed immediately by overlapping a self-expandable stent.
Pulmonary artery stenosis
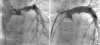
Nine self-expandable stents were used among 7 patients with pulmonary artery stenosis. In 2 patients who previously underwent Fontan operations, 1 patient had transposition of the great artery with PA and huge VSD while the other patient had congenitally corrected transposition of the great artery with large VSD. Multiple narrowing in the LPA after Fontan operation was observed in the patient with transposition of great artery with PA and huge VSD; hence, a self-expandable stent with a 12-mm diameter and 40-mm length was introduced via the right femoral vein and implanted in the LPA. However, the stent was not capable of covering multiple narrowing of the LPA. Thus, another self-expandable stent with a 14-mm diameter and 40-mm length was successfully overlapped with the first stent (Figure 1). In the other patient with congenitally corrected transposition of the great artery with large VSD, there was diffuse narrowing in the LPA after Fontan operation; hence, a self-expandable stent 14 mm in diameter and 40 mm in length was placed in the LPA successfully. In 1 patient with unilateral absence of the RPA who previously underwent RPA reconstruction using homograft, stenosis at the anastomosis site between the native pulmonary artery and conduit occurred during the follow-up period. Thus, a self-expandable stent with a 10-mm diameter and 40-mm length was implanted in the RPA. About 2 self-expandable stents were implanted in 1 patient due to distal migration of the first implanted stent in the distal pulmonary artery. In this patient, stenosis at the proximal LPA after DORV repair was noted, and a self-expandable stent with a 16-mm diameter and 30-mm length was initially placed in the LPA. However, distal migration of the stent occurred after deployment. Thus, another self-expandable stent 18 mm in diameter and 30 mm in length was overlapped with the first stent. There was 1 patient with severe mid-RPA stenosis who previously underwent pulmonary artery repair. In lung perfusion scan, the right-to-left lung perfusion ratio was found to be 15/85 (Figure 2), and the pressure gradient across the stenosis was measured at 26 mmHg. The patient's pulmonary artery measured approximately 20 mm. Consequently, a self-expandable stent with 22 mm and 40 mm in diameter and length, respectively, was implanted in the RPA. The stenotic segment of the RPA gradually widened through the stent's constant radial force as time passed. There was near-complete relief of the stenosis and blood flow restoration to the right lung 6 months after stent implantation (Figure 2).
 | Figure 1(A) Catheterization after Fontan operation demonstrated multiple narrowings of the LPA. (B) Angiography after 2 self-expandable stent implantation showing relief of the stenosis of LPA.LPA = left pulmonary artery.
|
 | Figure 2(A) Angiography showing severe stenosis of the right pulmonary artery (arrow). (B) Lung perfusion scan showing right-to-left lung perfusion ratio of 15/85. (C) Immediate follow-up angiography after stent implantation. (D) After 6 months of stent placement, there was near-complete relief of the stenosis by constant radial force.ANT = anterior.
|
RV-PA conduit stenosis
A 5-year-old girl with PA and large VSD underwent Rastelli operation and developed severe cyanosis that was prominent on the face and limb. Percutaneous oxygen saturation was 45% at rest, and she complained of severe dyspnea. At 2 years, she underwent Rastelli operation using a 12-mm valved conduit. The echocardiogram revealed severe narrowing of the valved conduit. Hence, emergent catheterization was done, and balloon dilation of the stenotic lesion in the valved conduit was initially performed. However, recoiling of the stenosed conduit occurred immediately following balloon dilation. With this, a self-expandable stent with a 14-mm diameter and 40-mm length was implanted in the RV-PA conduit. The narrowing of the valved conduit was almost abolished and blood flow restoration to both lungs was achieved. Percutaneous oxygen saturation increased to above 80% after stent implantation, and she was discharged. However, several days after the stent implantation, the patient appeared febrile and the fever persisted for a few days, after which the fever subsided for several consecutive days. Thereafter, the fever redeveloped and persisted. Follow-up echocardiogram after stent implantation revealed restenosis and some mass in the stented RV-PA conduit, and the percutaneous oxygen saturation decreased again to about 50% at rest. Catheterization was performed to identify the causes of this narrowing and cyanosis, and significant restenosis was found in the stented conduit. Its thickness amounted to 50% of the stented luminal diameter. Then, balloon dilation was initially attempted in the stented conduit, however restenosis after balloon dilation and aggravation of cyanosis were anticipated. So, we decided to place another stent with antibiotics rather than redo cardiac surgery. Following balloon dilation, another self-expandable stent 14 mm in diameter and 40 mm in length was overlapped with the first stent. There was a near-complete relief of the restenosis and pulmonary blood flow restoration after second stent implantation (Figure 3). Although the right ventricular to pulmonary artery flow was recovered again after second stent implantation, fever was not controlled despite adequate supportive care including antibiotics. Serial blood cultures were obtained to identify the cause of the fever, and we isolated Streptococcus oralis. Therefore, operation was decided on this patient with the possibility of infective endocarditis, and the vegetations were seen in the operating room, which adhered to the prosthetic valve in the RV-PA conduit. After the infected valved conduit and vegetations had been surgically removed, the patient eventually recovered.

Coarctation of the aorta
A self-expandable stent was placed in 1 patient with coarctation of the aorta. Previous coarctation repair was performed for this patient at 5 months of age. The echocardiogram and cardiac catheterization were conducted when he was 13 years, and the results revealed significant narrowing in the descending aorta. Consequently, a self-expandable stent with 22 mm in diameter and 40 mm in length was implanted. The narrowest diameter of the descending aorta increased from 11 mm to 16 mm. The pressure gradient across the stenotic lesion decreased from 20 mmHg to 7 mmHg immediately. Follow-up cardiac computed tomography after 1 year of stent implantation was performed, and no stenotic lesion or aneurysm in the descending aorta was observed (Figure 4).

DISCUSSION
Many interventional types of catheterization have been introduced and accepted as alternative to surgery in intravascular stenosis in several congenital heart diseases.5)6)7)8) Balloon dilation is a useful option for the management of intravascular stenosis; however, restenosis can frequently occur immediately or later following balloon dilation because of external compression, non-dilatable fibrotic lesion, or enhanced vessel elasticity. Mullins et al.9) reported the first implantation of balloon expandable stent in congenital heart disease in an experimental animal model in 1988. The advantages of stent implantation compared to balloon dilation are prevention of elastic recoil of the stenosed vessel and overcoming of external compressive forces. In 1991, O'Laughlin et al.10) reported balloon expandable stent implantation among 30 patients wherein 45 stents were placed. Thereafter, endovascular stenting has evolved as another viable option to treat intravascular stenosis instead of balloon dilation or vascular surgery. There are 2 general types of stents: a balloon expandable intravascular stent and self-expandable intravascular stent. A balloon expandable stent has become an integral part of the treatment of intravascular stenosis among children and adults with congenital heart disease, and it has successfully been used to manage and treat a variety of vascular stenoses such as pulmonary artery stenosis, coarctation of the aorta, arterial duct, postoperative systemic to pulmonary shunt, and RV-PA conduit.11)12)13) However, despite the benefits of balloon expandable stent implantation in congenital heart disease, some problems may arise when used in children. As the child grows, the final stent diameter of the target vessel achieved during implantation may not be adequate.14)15)16) Further, other potential problems such as in-stent restenosis, stent migration and malpositioning, balloon rupture, or vessel dissection were noted.17)18) Despite these complications, the use of a balloon expandable stent has been widespread and applied effectively in intravascular stenosis in various congenital heart diseases.
However, in our country, there is only a limited number of sizes and types of balloon expandable intravascular stents. It is not easy for us to apply a balloon expandable stent in intravascular stenotic lesions in congenital heart disease. Therefore, percutaneous balloon dilation has mainly been used in our country to dilate a stenosed vessel such as the pulmonary artery, coarctation of the aorta, and RV-PA conduit. However, recoiling or restenosis frequently occurred after balloon dilation as mentioned previously, and balloon expandable stents have been of limited use in a stenotic lesion of small to medium-sized vessel because of a limited number of sizes. Moreover, it has been more difficult to use an available balloon expandable stent in vascular stenosis especially in large-sized vessel. Hence, we used a self-expandable stent in intravascular stenosis in moderate to large-sized vessel after surgical repair, which is available in our country. Self-expandable stents were used in our institution for the following reasons; diffuse stenotic lesion, multiple stenoses, kinking vessel, externally compressed vessel, restenosis following balloon angioplasty, or stenoses presenting in the postoperative period. The advantages of self-expandable stents over the balloon expandable stents are their smaller delivery systems, their flexibility, conformability to the vessel wall, and easy deployment. Thus, self-expandable stent can be traversed over the wire despite tortuous vascular stenoses without slippage of the stent. The Hercules self-expandable vascular stent has been used in moderate to large-sized stenotic vessels such as the pulmonary artery, RV-PA conduit, and coarctation of the aorta in our institution. It is constructed from 2 threads of wire in a tubular configuration in an interlocking diamond-shaped meshwork (Figure 5). It is made in a shape of memory nitinol with a semi-open cell structure and reconstrainable design. This bare metal stent is available for a diameter of 8 to 22 mm and length of 30 to 120 mm. Its main advantages are good flexibility, conformability to the vascular structure, and it has soft ends which reduce vessel wall damage. Its flexibility allows for modelling of the stent to the vascular wall after stent implantation. Furthermore, such stent has a low constant radial force, resulting in gradual widening of the stenotic vascular segment and less vascular wall injury. In our study, the narrowest diameter of the stented vessel increased immediately from 5.7±3.2 mm to 9.4±3.0 mm (p<0.05) after stent implantation, and then the narrowest diameter of the stented vessel gradually increased to 12.6±3.4 mm (p<0.05) at the last follow-up (Table 2). However, there are limited data evaluating the outcomes of using self-expandable vascular stent in a stenotic lesion of moderate to large-sized vessel in congenital heart disease, especially in our country. We implanted mainly the self-expandable stent to the stenotic lesion in the pulmonary artery after surgical repair in congenital heart disease, and the stents were also placed in the RV-PA conduit after Rastelli operation and postoperative coarctation. Our study described acceptable short- and mid-term results of using the self-expandable stent for the treatment of vascular stenosis in moderate to large-sized vessel in congenital heart disease.
 | Figure 5Hercules self-expandable vascular stent, bare metal stent which is made in a shape of memory nitinol. It has soft ends and good flexibility.
|
Branch pulmonary artery stenosis may occur as congenital lesions or postoperative residual problems. Pulmonary artery stenoses frequently occur after TOF repair, Rastelli operation, or bidirectional or total cavopulmonary connections. Unilateral or bilateral pulmonary artery stenosis causes significant hemodynamic effects to the patient's condition and prognosis. In our study, pulmonary artery stenosis was observed in 2 patients after Fontan operation: 2 self-expandable stents were implanted in 1 patient with multiple narrowing of the LPA and 1 stent was placed in the other patient with hypoplastic LPA. Moreover, pulmonary artery stenosis was noted in patients with TOF and DORV after an attempted surgical repair; thus, a self-expandable stent was placed in each patient.
The use of the RV-PA conduit is helpful in the successful surgical corrections of patients with PA with VSD. However, if the surgical conduit degenerates over time, a narrowed RV-PA conduit could increase right ventricular pressure. This has a significant effect on the right ventricular function and re-do surgery will be required. Repeated surgeries pose a higher risk than the initial conduit surgery. Subsequently, catheter interventions such as conduit stenting will be needed to avoid the surgical risk and to delay its surgical replacement. RV-PA stenting provides sustained luminal widening without restenosis compared to balloon dilation.19)20) In our study, we placed a self-expandable stent in significantly narrowed RV-PA conduit in a patient with PA with VSD after Rastelli operation. The cause of restenosis of the stented conduit was large-sized vegetations which adhered to the prosthetic valve by infective endocarditis rather than neointimal ingrowth in self-expandable stent.
Percutaneous balloon dilation angioplasty has been known to be safe and effective in patients with postoperative recurrent or native coarctation. However, it may have suboptimal results caused by vessel recoiling, aortic dissection, or aneurysm formation.21)22)23) Endovascular stenting can generally provide uniform vascular support and can relieve the stenotic segment of the aorta without vessel disruption. Stent implantation in the aorta has also been successful in long segment lesion compared to balloon dilation angioplasty. In our case, there was a postoperative recurrent focal coarctation, and self-expandable vascular stent was implanted successfully.
Although there are many advantages of stent implantation in intravascular stenosis compared to balloon dilation angioplasty or surgery, procedure-related complications have also been reported after stent placement: stent migration, neointimal proliferation, vessel dissection, balloon rupture, or aneurysm formation. There are also potential problems when performed in a young child because of the failure to keep pace with the patient's somatic growth. The final diameter of the stented vessel achieved during implantation may not be adequate as the young patient grows; hence, surgical stent removal and repair may later be required in some patients. Neointimal ingrowth after stenting is a serious complication; however, the accurate mechanism of restenosis remains unclear. Cheung et al.3) reported significant intimal proliferation after self-expandable stent implantation. In contrast, other studies reported positive results that show good patency and little complication after the procedure.24)25) In our case, restenosis occurred following self-expandable stent implantation in the RV-PA conduit; however, the cause of the restenosis was vegetations which adhered to the prosthetic valve by infective endocarditis rather than neointimal proliferation of the stent.
The limitations of this study involve its retrospective nature, the limited number of self-expandable stent implantation evaluated, and the relatively short-term follow-up period. Thus, further investigation about self-expandable stent implantation in congenital heart disease with a large sample size will be needed.
In conclusion, this study shows that the self-expandable stent could be a useful option in the management of vascular stenosis in moderate to large-sized vessels in congenital heart disease, especially in special circumstances such as unavailable balloon expandable vascular stent. Although a self-expandable stent does not provide significant radial strength, it has a low constant radial force, which may result in a gradual widening of the stenotic segment and less trauma to the vessel. Thus, it could be used in stenotic vessels in congenital heart disease.
 XML Download
XML Download