

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Atrial fibrillation (AF) is the most common cardiac arrhythmia and is a growing health problem worldwide given the ageing of populations.1) AF increases the risk of stroke 5-fold, and is associated with increased risk of heart failure (HF), dementia, and all-cause mortality.2)3)4)5) The actual prevalence of AF is likely underestimated, as a large proportion of patients remain asymptomatic (‘silent AF’) and therefore undetected, so the first manifestations of AF may be a debilitating stroke or death.6) Once AF is detected, the risk of cardioembolic stroke can be effectively reduced by 64% with the commencement of oral anticoagulants (OACs), and all-cause mortality is reduced by 26%.7) However, this reduction in risk is largely contingent on the physician appropriately prescribing an OAC, and the patient persisting with this therapy.
ATRIAL FIBRILLATION AND ORAL ANTICOAGULATION PRESCRIPTION
A number of OACs, comprising of vitamin K antagonists (VKAs) such as warfarin and non-VKA OACs (NOACs) are used to reduce stroke risk among patients with AF.8) The use of warfarin or NOACs in high-risk patients has been shown to reduce stroke risk by up to 60–65%.9) Warfarin has traditionally been the medication of choice for managing high-risk patients with AF, until the advent and release of NOACs over the past decade, which have been shown to be as effective as warfarin, but are associated with a lower risk of major bleeding, particularly intracranial haemorrhage.10) Aspirin, which is sometimes used as a sole agent, or in combination with clopidogrel, has also been used by practitioners in the past and still continues to be used. However there is only weak evidence showing that antiplatelet agents (APAs) prevent stroke,9) and even when used in combination (e.g. aspirin and clopidogrel) have only been shown to have only half the efficacy of warfarin, with a similar incidence of major bleeding episodes.11) Indeed, misperceptions about both the efficacy and safety of aspirin in AF have probably been a major reason for perpetuation of OAC under-utilization.12) Currently, the Korean,13) European,14) USA,15) and American College of Chest Physician guidelines,16)and Australia and New Zealand9) guidelines for the management of stroke risk in AF discourage the use of APAs altogether for stroke risk reduction in AF.
NOACs are emerging as the preferred OACs for patients with AF at high-risk of stroke, and this has also been reflected in recent revisions of guidelines in Korea,13) Europe,14) the USA,15) and Australia and New Zealand9) which recommend NOACs as first-line medications. Efficacy, safety, ease of use without the need for regular blood monitoring have led to a gradual increase in NOAC use and a decline in warfarin or other VKA drug use for thromboprophylaxis for AF. However, some advantages of warfarin are that adherence to treatment can be easily monitored, it has a relatively long half-life, and a fast and effective mechanism of reversal is readily available.17) NOACs, on the other hand, are considerably more expensive than warfarin but have nevertheless been shown to be more cost-effective in the longer term.18) Unfortunately, there is a paucity of readily available measures of anticoagulation that can monitor patient adherence with NOACs, and reversal agents are less readily accessible in the event of a major bleed,17) though that situation is changing.
Stroke risk reduction guidelines for patients with atrial fibrillation
The appropriate identification and management of stroke risk in patients with AF is vital for reducing the incidence of avoidable stroke. New AF management guidelines have been developed and reviewed in recent years in Korea, the USA, Europe and Australia and New Zealand.9)13)14)15) Revisions of these guidelines in many countries have adopted the CHA2DS2-VASc/CHA2DS2-VA stroke risk assessment tool, superseding the CHADS2 score, for stratifying stroke risk due to a marginally improved stroke prediction risk, particularly in ascertaining those at low risk who do not require OAC.19) Patients score one point for: cardiac failure, hypertension, diabetes, vascular disease, age 65–74 years and female sex (the latter variable excluded from CHA2DS2-VA sexless score), and an additional point for age to give 2 points for age ≥75 years, and 2 points for previous stroke/transient ischemic attack (TIA). The recommendations are to commence an OAC for patients at high-risk (CHA2DS2-VASc≥2 in a male or ≥3 in a female=CHA2DS2-VA≥2), and consideration given to OAC for those with CHA2DS2-VA of one point, with oral anticoagulation therapy not recommended for those with a CHA2DS2-VA of zero.9)13) While these scores are easy to calculate at the bedside, the C statistic is only modest,16) and more complex scores including biomarkers offer a marginal increase which makes them less practical for widespread use.
Perceived bleeding risk is one factor, especially among Asian subjects, that contributes to sub-optimal prescribing of OACs among patients with a high risk of stroke.20) Not surprisingly, physicians are sensitized by a major bleed in one of their patients, but do not see the strokes they prevent. Bleeding risk can be estimated by a number of clinical scoring systems (e.g. HAS-BLED, ATRIA), however these algorithms have been shown to be only modest predictors of major bleeds.9) Due to similar factors predicting both stroke and bleeding risk, patients with higher CHA2DS2-VASc/CHA2DS2-VA scores are also at higher risk of bleeding. Current guidelines outline that the clinical benefit of stroke prevention nearly always outweighs bleeding risk, so bleeding risk scores should not be used to avoid anticoagulation in high-risk patients, but reversible bleeding risk factors which are incorporated in bleeding scores, should be identified and corrected, where possible.9)
The decision of whether to anticoagulate, and which anticoagulant to use, is made by the treating clinician after consultation with the patient. In this rapidly evolving area of changes to guidelines and therapies available, little is known about how prescribing practices have reflected these changes over the past decade.
Secular trends in overall oral anticoagulant use in atrial fibrillation over the past decade
Studies conducted in several countries over the past decade have consistently found an increase in the proportion of patients with AF appropriately prescribed OACs. The trend of increased use of OACs is evident from both large-scale time series analyses of patients with AF, as well as studies using prescription databases (Figure 1 and Table 1). 17)19)21)22)23)24)25)26)27)28)29)30)31)32)33)34)35)36)37)38)39)40)41)

Table 1
Secular trends in prescriptions for atrial fibrillation

| Author (years) | Country; study period | Source | Sample size | Primary outcome variable(s) | Secular trend over study period | ||||
|---|---|---|---|---|---|---|---|---|---|
| All OACs combined | NOAC | VKA | APA monotherapy | ||||||
| United Kingdom | |||||||||
| Apenteng et al. (2018)19) | UK; 2011–2016 | GARFIELD-AF registry | 3,482 | Prescription initiated at AF diagnosis (all CHA2DS2-VASc scores) | ↑ 54.7–73.9% | ↑ 2–47% | ↓ 53.3–30.6% | ↓ 36.4–10.5% | |
| Cowan et al. (2018)21) | UK; 2006–2016 | English national databases | Prescription proportion (CHA2DS2-VASc≥2) | ↑ 48.0–78.6% | ↑ 1–33% (2011–2016) | ↓ 42.9–16.1% | |||
| Protty and Hayes (2017)22) | UK (Wales); 2009–2015 | Welsh analytical prescribing unit | OAC prescriptions (items) per 1,000 prescribing units | ↑ 40.48–65.26% | Proportion of OAC defined daily doses: rivaroxaban: ↑ 17% | Proportion of OAC defined daily doses: ↓ 100–68% | |||
| Apixaban: ↑ to 9% | |||||||||
| Dabigatran: ↑ to 3% | |||||||||
| Robson et al. (2014)23) | UK (London); 2011–2013 | 4,604 | Prescription proportion (CHA2DS2-VASc≥1) | ↑ 52.6–59.8% | ↓ 37.1–30.3% | ||||
| Western Europe | |||||||||
| Maura et al. (2019)24) | France; 2011–2016 | French national health insurance database | 2,913,769 | OAC prescription initiated at diagnosis (all CHA2DS2-VASc scores) | ↑ 56.7–65.8% | 0–66.3% (2015–2016) | ↓ 57–41% | ↓ 37.1–30.3% | |
| Dalgaard et al. (2018)25) | Denmark; 2001–2012 | Danish nationwide registries | 12,231 | Proportion on OAC (all CHA2DS2-VASc scores) | ↑ 32.5–53.9% | ||||
| Gadsbøll et al. (2017)26) | Denmark; 2005–2015 | Danish national registries | OAC prescription initiated at AF diagnosis (all CHA2DS2-VASc scores) | 2005: 46.3% | ↑ 0–49% (2011–2015) | ↓ 50–18% | |||
| 2009: 38.1% | |||||||||
| 2015: 66.5% | |||||||||
| Gülker et al. (2018)27) | Germany; 2005–2014 | Wissenschaftliche Institut der AOK; and national hospitalisation database | Annual drug treatment rates per 100,000 persons hospitalised; using defined daily doses of OAC | ↑ 0–0.6% (of all people hospitalised) | ↑ 0.9–12.3% (of all people hospitalised) | ||||
| Urbaniak et al. (2017)28) | Norway; 2012–2015 | Norwegian prescription database | 57,995 | Proportion prescribed OAC (all CHA2DS2-VASc scores) | Apixaban: ↑ 2–43.5% | ↓ 33.2–17.2% | |||
| Rivaroxaban: ↑ 18.4–22.4% | |||||||||
| Sindet-Pedersen et al. (2018)29) | Denmark; 2011–2016 | Danish national prescription registry | 2,946 | NOAC prescription initiated at diagnosis (all CHA2DS2-VASc scores) | ↑ 10–52% | ||||
| Haastrup et al. (2018)30) | Denmark; 2008–2016 | Danish national prescription registry | 126,691 | No. of patients prescribed NOAC per 1,000 individuals in the Danish population | ↑ 0–2% (of the Danish population) | ||||
| USA and Canada | |||||||||
| Pilote et al. (2013)31) | Canada; 1998–2006 | Hospital administrative database | 338,479 | OAC prescription in newly diagnosed AF (all CHA2DS2 scores) | ↑ 51–64.5% | ↑ 20–22.3% | |||
| Weitz et al. (2015)32) | Canada; 2008–2014 | Canadian prescription database | Total OAC scripts (all indications) | ↑ From 4.8 to 7 million prescriptions per year | Rivaroxaban: ↑ to 18% | ↓ 99–67% (2010–2014) | |||
| Dabigatran: ↑ to 15% | |||||||||
| Apixaban: ↑ to 7% | |||||||||
| Marzec et al. (2017)33) | USA; 2008–2014 | NCDR PINNACLE registry | 655,000 | Proportion on OAC (CHA2DS2-VASc≥1) | ↑ 52.4–60.7% | ↑ 0–25.8% | ↓ 52.4–34.8% | ||
| Thompson et al. (2017)34) | USA; 2008–2014 | NCDR PINNACLE registry | 691,906 | Proportion on OAC (CHA2DS2-VASc≥2) | ↑ 57–60% | ↓ 56–28% | |||
| Lubitz et al. (2018)35) | USA; 2008–2014 | NCDR PINNACLE registry | 674,841 | OAC among patients (CHA2DS2-VASc≥2) | Likelihood of being treated with an OAC increased with time | ||||
| Steinberg et al. (2017)17) | USA; 2013–2016 | ORBIT-AF registry | 4,670 | NOAC prescription in newly diagnosed AF (all CHA2DS2-VASc scores) | ↑ 0–75% | ||||
| Zhu et al. (2018)36) | USA; 2010–2017 | Health insurance database | 112,187 | NOAC prescription in newly diagnosed AF (CHA2DS2VASc≥2) | ↑ 8.1–78.9% | ||||
| Asia | |||||||||
| Chao et al. (2018)37) | Taiwan; 2008–2015 | Taiwan national health insurance database | 181,214 | Proportion on OAC (CHA2DS2-VASc: ≥1 males and ≥2 females) | ↑ 13.6–35.6% | ↑ 0–26% | ↑ 13.6–9.6% | ||
| Lee et al. (2017)38) | Korea; 2008–2015 | National Health Insurance Service of Korea database | 276,246 | Proportion prescribed OAC (CHA2DS2-VASc≥2) | ↑ 34.7–50.6% | ↑ 0–25.4% (2012–2015) | ↓ 36–26% | ↓ 30.2–16.3% | |
| Guo et al. (2015)39) | China (Yunnan provence); 2001–2012 | 921 | OAC treatment initiated at AF diagnosis (CHA2DS2-VASc≥2) | ↑ 8–55% | ↑ 0–9.5% | ↑ 4–46.1% | |||
| Countries combined | |||||||||
| Verheugt et al. (2018)40) | 35 countries; 2010–2016 | GARFIELD-AF registry | 51,270 | OAC or APA treatment initiated at AF diagnosis | ↑ 42.1–57.7% | ↓ 30.2–16.3% | |||
| Haas et al. (2019)41) | 35 countries; 2013–2016 | GARFIELD-AF registry | 24,137 | NOAC prescription in newly diagnosed AF (CHA2DS2VASc≥2) | ↑ 33.8–62.6% | ||||
AF = atrial fibrillation; APA = antiplatelet agent; GARFIELD-AF = global anticoagulant registry in the field-atrial fibrillation; NCDR PINNACLE = national cardiovascular data registry's practice innovation and clinical excellence; NOAC = non-vitamin K antagonist; OAC = oral anticoagulant; ORBIT-AF = outcomes registry for better informed treatment of atrial fibrillation; VKA = vitamin K antagonist.
Approximately 10 years ago baseline rates of OAC use among intermediate-to-high risk patients ranged from 45–80% in the UK21)23) and USA,31)33)34) and were substantially lower in some Asian countries,37)38)39) ranging from 8–35%. In the UK,19)21) Europe24)26) and Asia,38)39) the proportion of patients with AF who were treated with an OAC increased by more than 50% over the decade from 2005–2015. This trend was seen for all stroke risk categories combined, as well as among intermediate-to-high risk patients. In the US the increase was marginally less than observed in other regions, but may have reflected the shorter time periods covered by these studies and/or the higher baseline rate of OAC use31)33)34). After 2015, rates of OAC prescription among intermediate-to-high risk patients increased to around 60–75% in the UK, Western Europe and USA21)23)33) and between 50–55% in Asian countries.37)38)39)
Although these findings shed a positive light on increased use of OACs to mitigate stroke risk in AF, they also show that increased OAC use was not uniform within and between countries, and that OAC use overall remained sub-optimal. Among the studies reviewed, only 50–70% of patients with CHA2DS2-VASc ≥2 were treated with OACs in the more recent years of the studies,21)34)35)38)39) leaving 30–50% of high-risk patients vulnerable to thromboembolic stroke.
Secular trends in the use of vitamin K antagonists for stroke risk reduction in atrial fibrillation
A number of studies have examined VKA prescription (predominantly warfarin) over the past decade, and have found marked shifts in practice, with sharp declines in the prescription of VKAs in most countries between 2010 and 2015. Prior to the introduction of NOACs, studies that examined trends in VKAs suggest that VKA use was increasing steadily.27)31)39) These studies show that prior to the introduction of NOACs VKAs were the preferred medication and were used in 50–70% of intermediate-to-high risk patients prescribed an OAC, however this reduced to 30–40% after the introduction of NOACs.33)34)38) These reductions in VKA use in the last half of the previous decade have been observed in the UK,19)22) Western Europe,24)26)28) USA,32)33)34) and Korea38) (Table 1).
Secular trends in the use of antiplatelet agents as monotherapy for stroke risk reduction in atrial fibrillation
A number of studies have documented a decline over the past decade in the use of APAs as monotherapy for the prevention of thromboembolism among intermediate and high-risk patients (Table 1). At the beginning of the past decade between 30–40% of patients with CHA2DS2-VASc ≥2 in the UK,19)21)23) Western Europe24), and Korea38) were treated with APA as a monotherapy (predominantly aspirin). Overall prevalence of APA monotherapy among high-risk groups declined to around 30% in these countries toward the end of the decade. The only study that was an exception to this trend was a study in China, which showed a sharp increase in aspirin monotherapy increasing from 4–46% among patients with CHA2DS2-VASc ≥2 between 2001 and 2012.39) Although there has been a notable decrease in the use of APAs as monotherapy to reduce stroke risk, there still remains a significant proportion of high-risk patients (approximately 30%) that are receiving inappropriate APA thromboprophylaxis for reducing stroke risk.
Secular trends in non-vitamin K antagonist oral anticoagulants over the past decade
Studies of prescription registry data and time-series analyses in multiple countries over the past decade have consistently shown that NOACs emerged as the favoured anticoagulant toward the end of the past decade (Figure 2 and Table 1).22)24)26)27)28)30)31)32)37) NOACs were released in the market between 2010 and 2013 in the USA, Western Europe, and Korea. Studies in these countries have shown that in the first 1–2 years after their release, the proportion of high-risk patients that were prescribed NOACs increased from <2% to 25–33%.21)33)36)38) A study in the USA that has followed up for five years after the introduction of NOACs showed that an even higher proportion (75%) of high-risk patients were prescribed a NOAC when diagnosed with AF. The relative use of this class of anticoagulants is of course also determined by the level of government subsidization of their cost, which can be minimal or absent in low- and middle-income countries, where the cost of NOACs may be beyond the reach of most elderly patients with AF.
Figure 2
Secular trends of warfarin versus NOACs.
NOAC = non-vitamin K antagonist oral anticoagulant.

A number of studies have examined clinician's prescribing behaviours after the introduction of NOACs. In the period immediately following NOAC release, patients prescribed this class generally had lower stroke and bleeding risks compared with those treated with warfarin.17)19)33) Other studies showed that patients with certain risk factors represented in the CHA2DS2-VASc score, such as advanced age, vascular disease, HF, male gender and diabetes were also less likely to be prescribed NOACs.17)33) There is a growing body of research that is suggesting that clinicians have improved their prescribing of NOACs to more closely follow guidelines in more recent years.19)23)26)33) However, perceived higher bleeding risk of NOACs is still reported by clinicians to be a barrier to their use,8)10) despite warfarin and NOACs having relatively similar bleeding risk profiles, with the marked exception of intracranial hemorrhage.9) There is also some evidence suggesting that specialists and sub-specialists, such as cardiologists and electrophysiologists, are more inclined to prescribe NOACs in preference to warfarin compared to primary care physicians.36)42)
A number of factors may contribute to these trends. Several contraindications to NOACs that are associated with CHA2DS2-VASc score, such as renal impairment and valvular heart disease may coexist among patients with higher CHA2DS2-VASc scores, although a recent meta-analysis of NOAC use in chronic kidney disease suggests this class is safer than VKA.43) There was no anticoagulation reversal for bleeding available for NOACs when they were released on the market, therefore clinicians may have been less inclined to prescribe them to patients with higher bleeding risk. This is despite evidence from the pivotal randomised trials which showed that NOACs were safer after a major bleed than VKAs in the absence of a reversal agent which was available for VKA. Furthermore, clinicians (and especially non-specialised clinicians) may lack familiarity and experience with prescribing NOACs and may choose to stay with agents with which they are more familiar, comfortable and knowledgeable. This has been one area of focus in quality improvement activities for clinicians,44) but also a focus of the promotion and marketing activities by pharmaceutical companies following the development of reversal agents such as idarucizumab and andexanet alpha and their release to the market.45)46) To date, there is no compelling evidence suggesting clinicians favour one NOAC over another, and prescribing of specific NOACs seems to be largely driven by country and regional factors in availability, promotion, or reimbursment.17)
Summary of the secular trends in the management of stroke risk among patients with atrial fibrillation
Multiple studies from several countries support that the clinical management of AF to reduce stroke risk with thromboprophylaxis has progressively improved over the past decade, in response to promotion of changes in AF management guidelines, various practice incentives, perceived ease of use of NOACs and strong marketing by pharmaceutical companies which produce NOACs during the same time frame. This has been strikingly mirrored by a declining incidence of AF-related stroke.21)37)44) Newly-diagnosed patients with intermediate/high stroke risk are increasingly more likely to receive guideline-recommended therapy. But the higher rates are not uniform, and remain low in a number of countries. There has also been a notable decrease in the use of APAs to reduce stroke risk, the one exception being China, which showed an increased use of aspirin over the past decade.39)47) The transition from the CHADS2 to CHA2DS2-VASc for stroke risk assessment has increased the proportion of patients deemed to be at higher risk during this period. The relative ease-of-use and fewer contraindications and interactions certainly played a major role in their uptake by physicians prescribing them as first-line therapy.
There remains a significant proportion of high-risk patients that are being treated with APAs alone, which are markedly less effective than OACs, relatively ineffective in preventing large cardio-embolic stroke, but still have appreciable major bleeding risks. There is also a sizeable proportion of low-risk patients inappropriately receiving anticoagulation therapy. On the positive side, the most important example of the impact of the favourable secular trend in appropriate prescription has been in the United Kingdom. Increase in appropriate OAC prescription to 78% from the 2009 level, and decrease in antiplatelet use, has been predicted to be associated with the prevention of 4,000 AF-related strokes in 2019 alone.12)21) It will take some time to quantify how these changes in practice have translated into AF-related stroke outcomes globally.
PATIENT PERSISTENCE AND ADHERENCE WITH ORAL ANTICOAGULANT THERAPY
Medication persistence is the act of continuing to take medications for the prescribed treatment duration.48) In AF, this usually equates to lifelong treatment. Non-persistence is defined as discontinuation of the medication, i.e. stopping the drug permanently. Non-persistence is usually assumed when scripts are no longer filled after a specified grace period, which varies in the literature from 30 to 90 days.
In contrast, medication adherence refers more to patients taking the drug as prescribed; relating to aspects such as timing, number of daily doses taken, and adhering to any required dietary modifications.48) Adherence is commonly calculated from prescription databases using the proportion of days covered (PDC) according to the prescribed medication dosage: good adherence is usually defined as a PDC >0.80. The PDC accounts for daily doses that may be missed and interruptions to therapy, however in some studies, those who have discontinued their medication (i.e. absolute non-adherence) are also counted in the total PDC. Therefore, direct comparison of both adherence and persistence rates between studies is limited due to different definitions and methodologies for calculating these outcomes.
Impact of poor persistence and adherence
Although there has been an improvement in overall guideline-based prescription of OAC over the past decade, prescription alone is not sufficient for effective stroke prevention in AF. It is also pertinent that patients continue to take OAC medications long-term (persistence), and take them as prescribed (adherence), however, a global problem exists with both patient persistence and adherence which requires further exploration and attention. It seems obvious that the benefits of OAC on stroke and mortality documented in randomized trials will not be realised if the medication is not taken. This issue of poor persistence and adherence, however, is not widely appreciated to be a significant cause of AF-related stroke. A study of data from the UK Clinical Practice Research Datalink demonstrated a high early stroke risk of discontinuing OAC, which remained fairly constant over the following 3 years, leading to an excess of 5 strokes in 3 years for every 100 people who stop OAC.49)
Good adherence, defined as PDC >0.80, is associated with reduced risk of all-cause mortality (hazard ratio [HR], 0.86; 95% confidence interval [CI], 0.81–0.91) and ischaemic stroke (HR, 0.69; CI, 0.56–0.85) as shown from data from the Valencia Health System database in Spain (n=37,774).50) Conversely, poor adherence (PDC<0.80) at 12-month follow-up is associated with a significantly higher risk of both ischaemic stroke (HR, 2.08; CI, 1.11–3.88) and deep vein thrombosis (HR, 5.39; CI, 1.78–16.3).51) Further, it appears that the degree of stroke and mortality risk is proportional to the degree of adherence. For each 0.10 decline in PDC for dabigatran there was an associated higher risk of mortality and stroke (HR, 1.07; CI, 1.03–1.12). While the point estimate was identical for rivaroxaban, the trend was non-significant (HR, 1.07; CI, 0.89–1.28).52) A similar association for dabigatran was noted in a study using the USA Veterans Affairs database (n=5,376: there was an increase in all-cause mortality and stroke (HR, 1.13; CI, 1.08–1.19) for each 0.10 decline in PDC.53) Interestingly, when NOAC adherence is poor (PDC<0.80) the resulting increased ischaemic stroke risk is similar for both NOACs taken once-daily (HR, 1.47; CI, 1.20–1.80) and those taken twice-daily (HR, 1.50; CI, 1.23–1.83).54)
The global issue of suboptimal persistence
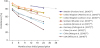
Persistence with OAC therapy appears to be a problem worldwide, with similar patterns of decline noted across different countries (Figure 3).26)55)56)57)58)59)60)61)62) Once prescribed, a large proportion of patients fill their initial OAC prescription, but persistence declines over time, with around only half of patients still taking OAC therapy by 2 years. Discontinuation often seems to occur quite early after initial prescription. USA health care claims data (n=16,253) showed the mean time to discontinuation occurred at ~3.7 months; and after 2-years follow-up persistence with warfarin was only 49%.63) Similar low persistence rates at 2-years were also noted in China (43%)64) and Germany (48%).60)
A gradual decline in persistence following initiation of OAC therapy has been noted in all studies (Table 2).52)53)55)56)57)58)59)60)61)64)65)66)67)68)69)70)71)72) In Australia, the first prescription repeat was filled by 91% of patients, reducing to 70% at 12-months, and 57% at 30-months.59) Similar declines were noted in Scotland where persistence rates for NOACs were 76% at 12-months, and 70% after 18-months,58) and the United Kingdom with 2-year persistence rates dropping to ~70%.56)57) The highest reported persistence rates overall came from the Stockholm administrative health data register, which reported persistence for any OAC was 88% at 12-months and 83% at 2-years,55) but these rates may be influenced by the definition of discontinuation, being any script filled in the 6-month follow up period.55) However, there may be a cultural influence as other Swedish studies have also identified high long-term persistence rates of 89% after 5-years.73) Self-reported discontinuation from the Chinese AF registry also identified similarly high persistence rates for NOAC medications.61)
Table 2
Time-course of persistence and adherence for oral anticoagulants from initiation of therapy

| Study (years) | Country; study period | Source | Sample size | Measure definition | VKA (%) | Apixaban (%) | Rivaroxaban (%) | Dabigatran (%) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Months | Months | Months | Months | ||||||||||||||||||
| 3 | 6 | 12 | 24 | 3 | 6 | 12 | 24 | 3 | 6 | 12 | 24 | 3 | 6 | 12 | 24 | ||||||
| Persistence | |||||||||||||||||||||
| Beyer-Westendorf et al. (2016)66) | Germany; 2012–2013 | IMS® Disease Analyzer | 7,265 | Supply gap>60 days | 58 | 26 | 66 | 53 | 60 | 47 | |||||||||||
| Collings et al. (2017)60) | Germany; 2012–2014 | IMS® Disease Analyzer | 15,244 | Supply gap>60 days | 94 | 71 | 58 | 49 | 79 | 72 | 63 | 59 | 82 | 67 | 57 | 49 | 71 | 60 | 50 | 42 | |
| Hohnloser et al. (2019)67) | Germany; 2013–2016 | Institute for Applied Health Research | 51,606 | Supply gap>30 days | 70 | 72 | 71 | 67 | |||||||||||||
| Forslund et al. (2016)55) | Stockholm; 2011–2014 | Stockholm administrative health data register | 17,741 | Any script filled in 6-months period; CHA2DS2-VASc=2–9 | 85 | 78 | 86 | 77 | 69 | 74 | 66 | ||||||||||
| Björck et al. (2016)68) | Sweden; 2010–2013 | AuriculA Swedish national quality register | 478 | Not defined | 91 | ||||||||||||||||
| Johnson et al. (2016)57) | UK; 2012–2014 | Clinical practice research database | 15,242 | Supply gap>56–60 days | 94 | 87 | 78 | 71 | 92 | 88 | 83 | 83 | 86 | 81 | 73 | 68 | 84 | 74 | 67 | 63 | |
| Martinez et al. (2016)56) | UK; 2011–2014 | Clinical practice research database | 27,514 | Supply gap>30 days | 87 | 77 | 64 | 50 | |||||||||||||
| Mueller et al. (2017)58) | Scotland; 2011–2014 | Prescribing Information System | 5,398 | Supply gap>28 days | 87 | 86 | 84 | 79 | 75 (18-months) | 68 | 60 | 55 (18-months) | |||||||||
| Simons et al. (2016)69) | Australia; 2013–2015 | PBS records | 1,471 | Supply gap>90 days | 86 | 38 | |||||||||||||||
| Simons et al, (2017)59) | Australia; 2013–2016 | PBS records | 8,656 | Supply gap>90 days or switching to warfarin | 92 (first repeat) | 73 | 61 (30-months) | 91 (first repeat) | 68 | 55 (30-months) | 89 (first repeat) | 66 | 52 (30-months) | ||||||||
| Shiga et al. (2015)70) | Japan; 2011–2014 | Tokyo Women's Medical University Hospital | 601 | Discontinuation reported in medical record | 93 | 88 | 82 | 90 | 83 | 80 | 88 | 83 | 70 | 80 | 76 | 65 | |||||
| Wang et al. (2016)64) | China; 2011–2014 | Chinese AF registry | 1,461 | Self-reported discontinuation | 78 | 56 | 43 | ||||||||||||||
| Liu et al. (2019)61) | China: 2011–2017 | Chinese AF registry | 5,699 | Self-reported discontinuation | 93 | 89 | |||||||||||||||
| Zalesak et al. (2013)71) | USA; 2010–2012 | USA Department of Defence | 5,145 | Supply gap>60 days | 53 | 39 | 72 | 63 | |||||||||||||
| Adherence | |||||||||||||||||||||
| Borne et al. (2017)52) | USA; 2010–2015 | Veterans Affairs Healthcare System | 2,882 | PDC>0.80 | 77 | 75 | 71 | ||||||||||||||
| Brown et al. (2017)72) | USA; 2012–2014 | Truven Health Analytics MarketScan database | 15,341 | PDC>0.80 | 71 | 60 | 71 | 59 | 61 | 48 | |||||||||||
| Han et al. (2019)65) | Korea; 2014 | HIRA service-aged patient sample | 1,234 | MPR≥0.80 | 92 | 84 | 88 | ||||||||||||||
| Shore et al. (2014)53) | USA; 2010–2012 | Veterans Affairs Corporate Data Warehouse | 5,376 | PDC≥0.80 | 71 | 71 | |||||||||||||||
Suboptimal adherence
It is more difficult to gauge if medications are actually taken once the prescription is filled.74) Different methods can provide vastly differing results when calculating adherence and persistence rates. In a study using the USA HealthCore Integrated Research Database (n=675) adherence at 12-months was 48% using prescription refill data, and only 37% when measured using self-report (the eight-item Morisky Medication Adherence Scale [MMAS-8]).75) This could suggest that although people were filling their prescription they may not have actually taken all the doses.76) Other studies using MMAS-8 survey data have also shown poor long-term adherence of only 55%.77)
Most studies have utilised PDC to measure adherence. The majority of these studies are cross-sectional, rather than looking at the time-course of adherence following treatment initiation. The studies looking at adherence over time do show a reduction in adherence to NOACs following treatment initiation (Table 2). Using PDC ≥0.80, data from the USA Veterans Affairs Healthcare System (n=2,882) identified 72% adherence at 12-months.52) Korea had similar rates for adherence to of NOACs of 87% measured with medication possession ratio ≥0.8 using Health Insurance data (n=1,234).73)
Comparison between oral anticoagulant medications
In the early 2000s persistence to warfarin was reported to be ~70% at 1-year and ~60% at 2-years.78)79)80) With the release of NOAC medications in the early 2010s, the generally-held perception was that NOACs would result in better medication adherence and persistence, in part due to the reduced need for monitoring, and dietary restrictions. Many studies have reported higher persistence rates for NOACs, however some large studies published in the last 4 years that have shown little difference between NOAC and VKA persistence (Table 2). A meta-analysis of OAC medications from 2014 also identified no statistical difference in persistence rates between VKA and NOAC.81)
A large study from Germany (n= 51,606) showed similar persistence at 12-months with warfarin (70.1%) and NOACs (70.5%).67) Similarly, within a Stockholm study (n=17,741), at 12-months warfarin persistence (85%) was similar to apixaban (86%), and both were notably higher than dabigatran (77%) and rivaroxaban (74%).55) In contrast, data from the United Kingdom for 2011–2014 found higher persistence rates for NOACs compared with warfarin at all time-points: 3-months (95% vs. 87%), 6-months (86% vs. 77%), 12-months (79% vs. 64%), and 2-years (70% vs. 50%).56) Also, an Australian study from 2013–2015, found persistence at 12-months was 70% for NOACs and 38% for warfarin: indicating patients on warfarin were 2.5 times more likely to discontinue over 12-months than those on NOACs.69)
Overall, it appears that apixaban consistently achieves higher persistence rates than the other OAC medications, with warfarin and rivaroxaban generally achieving similar rates, and dabigatran overall achieving the lowest rates (Table 2). Higher persistence for apixaban is noted across all time points, except for one German study which showed warfarin persistence (94%) was higher than the NOACs at 3-months (mean 81%); however at 12-months apixaban had highest persistence (63%).60) Because apixaban was launched a few years after dabigatran and rivaroxaban, comparative data have only been available relatively recently, and it should be noted that in many of these analyses there were smaller numbers treated with apixaban.
This result of higher persistence with apixaban is somewhat surprising given that apixaban is required to be taken twice-daily, compared to the once daily dosing of rivaroxaban. A meta-regression of persistence to cardiac medications confirmed that people on twice-daily dosages are 23% (CI, 13–33) less likely to have good persistence than those with once-daily regimes.82) A large USA study (n=36,868) comparing NOACs noted higher adherence of 73% for once-daily dosing with edoxaban or rivaroxaban (combined), compared to 68% for twice-daily dosing with apixaban or dabigatran (combined).54) However, as apixaban users constituted only a quarter of the twice-daily population, and rates were not reported separately for each medication and it is possible that those on apixaban may have also achieved superior persistence in that study.
Persistence and adherence to other medications
Sub-optimal medication adherence is not unique to OACs. A review of USA claims data in 2010 noted only 72% of all new prescriptions were filled, in respect of all medications.74) In this analysis, adherence with filling prescriptions was notably worse for chronic conditions such as hypertension (filling rate: 72%), hyperlipidaemia (72%), and diabetes (69%).74) This is consistent with low rates of adherence to cardiac medications. Following myocardial infarction, when it could be assumed that motivation to take medications should be high, adherence with taking medications was only 57%.83) In this myocardial infarction sample (n=405) from the USA, the factors associated with lower adherence were younger age, lower education, lower financial stability, and concerns about medication side effects.83) Although race has not been identified as a factor related to adherence, it was noted that African Americans were less likely to follow instructions on how to take their medications.84)
Patient beliefs about cardiac medications and treatment were identified as a major theme in an Australian review, where adherence with cardiac medications was recorded as 57–86%.85) In comparison, self-reported adherence with cardiac medications was better in Japan at 83%.86) Interestingly, in that study ‘forgetting’ to take medications was the most common reason for poor adherence, and this was most likely to occur for medications requiring ≥2 dosages per day, younger age, and those employed (especially those with a busy work schedule).86)
Factors associated with oral anticoagulant adherence and persistence
Overall, OAC adherence rates appear to be comparable to adherence rates for chronic and cardiac conditions. Therefore, multiple patient-level factors may be contributing to poor adherence and persistence in addition to specific OAC-related factors (e.g. fear of bleeding, difficulty with monitoring and INR testing, and dietary restrictions related to warfarin). General factors affecting both OAC adherence and persistence should be assessed in each patient, with consideration of both ‘lifestyle’ and ‘intrinsic’ factors (Box 1).
Box 1: Factors that may be associated with poor adherence and persistence
-
Medical factors:
-
Patient factors:
Younger age
Lower health literacy
Low AF knowledge; unaware of associated stroke risk
Poor OAC knowledge
Medication concerns (bleeding and lifestyle related)
Information overload
Anger, depression or anxiety from the AF diagnosis
Low treatment satisfaction
Busy work schedule
No health insurance cover; low ability to pay for medications
Age
Most research indicates a clear association between older age (≥65 years) and better adherence63)72)77)87) and persistence to OAC therapy.52)67)71) A stepwise trend was noted for better persistence with increasing age: 65–74 years HR, 0.95 (CI, 0.88–1.03), 75–84 years HR, 0.77 (CI, 0.71–0.83), and 85+ years HR, 0.64 (CI, 0.58–0.71).67) In a large USA study (n=15,341) using the MarketScan database, adherence was also noted to strengthen over time since initial prescription.72) Compared to those younger age groups, for people aged 65–74 years the odds ratio (OR) for better adherence was 2.94 (CI, 2.66–3.24) at 3-months, 3.60 (CI, 3.27–3.97) at 6-months, and 5.43 (CI, 4.89–6.04) at 12-months.72) Only one study contrasted these results. Data from the German IMS® Disease Analyzer (n=7,265) indicated that increasing age was associated with poorer persistence, with an OR, 0.99 (CI, 0.98–0.99) per extra year of age.66)
Sex
There is no clear association seen between sex and OAC persistence. One German study (n=7,265) suggested male sex was associated with better persistence rates: OR, 1.11 (CI, 1.01–1.23).66) In contrast, a larger German study (n=51,606) reported male sex was associated with higher rates of discontinuation: HR, 1.12 (CI, 1.06–1.18).67) This lower persistence in men was supported by an Australian survey which identified women were more likely to comply with their medication regime than men OR, 1.69 (CI, 1.08–2.63).77)
Co-morbidities
In general, people with additional medical co-morbidities are more likely to have higher adherence and persistence to OAC therapy, especially those with comorbidities related to an increased stroke risk.52)63)64)71) Results obtained in Germany and the USA showed similar associations with higher persistence for the presence of hypertension OR, 1.19–1.23 and diabetes OR, 1.21–1.24.66)72) Additional associations likely to improve persistence included dyslipidaemia OR, 1.21 (CI, 1.12–1.31) and cancer OR, 1.28 (1.12–1.48).66)72) Further, people were less likely to discontinue OAC if they also had congestive HF (HR, 0.90; CI, 0.85–0.96) or peripheral artery disease (HR, 0.89; CI, 0.81–0.97).67) As expected, those with a prior history of stroke/ TIA were much less likely to discontinue OAC (OR, 0.36; CI, 0.2–0.68),52) and those without prior stroke/TIA have higher likelihood of discontinuing (HR, 1.60; CI, 1.24–2.05).52)64)
Conversely, those with a higher bleeding risk were more likely to discontinue (HR, 1.25; CI, 1.08–1.46), as well as those with a history of intracranial bleeds (HR, 3.61; CI, 1.80–7.25).71) Other factors associated with a higher likelihood to discontinue are paroxysmal AF (HR, 1.56; CI, 1.28–1.92), where both doctors and patients may not perceive a significant risk if they are mostly in sinus rhythm64) and absence of AF symptoms.88)
Health insurance and financial circumstances
The presence of health insurance is an importance consideration in OAC persistence.64)66) In China, people without insurance cover are more likely to discontinue (HR, 1.65; CI, 1.03–2.64).64) Similarly, the presence of health insurance led to better persistence rates with an OR, 1.22 (CI, 1.03–1.44) according to German IMS® Disease Analyzer data.66) Lower socio-economic status and capacity to afford medications, significantly impacts ability to fill prescriptions,89) and adherence is known to be lower for medications that cost more.77) Other research from the USA, has identified income and social support as known variables affecting medication taking as a whole.84)
Health literacy, atrial fibrillation knowledge, and oral anticoagulant knowledge
Intrinsic patient factors such as core beliefs, health literacy, cognition, and medication awareness, can significantly alter the patient's decisions about taking medications.90)91) If correctly identified, these factors can be addressed and overcome with appropriate interventions.90)91) Health literacy, and knowledge of AF are significant predictors of medication adherence in AF.77)88)92)93) As a specific example, 21.7% of patients, in a Chinese study, declined to take the prescribed OAC because they were not informed of the stroke risk associated with AF.94)
Greater OAC knowledge was highly associated with better adherence (OR, 1.60; CI, 1.12–2.30)88); especially in relation to better understanding of risk-benefit, bleeding risk and how this impacts their quality of life.89) A belief in the importance of OAC medications increases adherence, and strong negative beliefs or fears around OAC medications (especially the perceived adverse effects of warfarin) lead to poor adherence.93) Despite these concerns, a systematic review has shown appropriate education can overcome barriers regarding fear of bleeding, resulting in the majority being willing to accept an increased bleeding risk to reduce the risk of a stroke.95) However, education needs to be correctly targeted to individual patients, as information overload can led to poorer adherence.77)
Personal well-being, lifestyle and employment
Treatment satisfaction is associated with better adherence (OR, 1.05; CI, 1.00–1.09).77)88) Emotions of anger, depression, or anxiety resulting from the AF diagnosis reduce adherence and persistence.87)96) Furthermore, it is also reported that impaired memory, family situations, support available, and busy work schedules all affect adherence.89)
Factors impacting adherence are often related to lifestyle choices.90)91) Particularly in the young and middle-aged, non-adherence may result from the demands of work, social activities and commitments.93)97) People who are employed are more likely to have lower OAC adherence compared to those who are unemployed.77) Thus, time commitments are an important consideration, and medication regimes with fewer daily doses are shown to have higher adherence.97) These factors can easily be overlooked during a consultation, however, it is important to consider the patient's well-being and personal circumstances in order to determine the pertinent factors impacting medication adherence and persistence.
How to improve oral anticoagulant adherence and persistence in practice
Health professionals have a pivotal role in assessing and maximising medication adherence and persistence among their patients. The critical role of monitoring OAC persistence has recently been highlighted by the European Heart Rhythm Association (EHRA) (Box 2).91) EHRA's practical guide for OACs in AF advocates for 3-monthly follow-up to review persistence.91) The guide recommends multiple strategies to achieve optimal adherence and persistence, including: adequate patient education; involvement of family members; pre-specified follow-up schedules; involving a local pharmacist if possible; use of technical aids (medication boxes, phone apps, reminder systems); and electronic monitoring if poor adherence is suspected.91) The new Australian AF management guidelines have also recommended similar strategies and note that specific attention should be paid to patient persistence.9) The Australian guidelines also recommend the development of individualised strategies to increase adherence and persistence, and recognise the need for patient-centred care and decision-making in this process.9)
An important intervention effect was observed in the IMPACT-AF cluster-randomised controlled trial which assessed the effect of targeted education of providers, patients and families.98) In that study, significantly higher proportions of patients were appropriately prescribed OAC in the intervention group at 6-months and 1-year.98) However, the AEGEAN study looked at the effect of additional education on adherence to apixaban over 48 weeks, however failed to find an improvement.99) Patients were randomised to standard care only, or standard care plus an education package which included a selection of reminder apps and access to a virtual clinic.99) Both groups were followed up every 12-weeks to determine medication adherence, and at 48 weeks there was no difference between additional education and standard care (90.4% vs. 90.1%).99) This high adherence in both groups may be the result of regular follow-up, which was also observed in a smaller study in Belgium.100) Potentially, attention to individual patient factors may have further improved adherence rates, however it would be difficult to improve on 90% adherence.
Patient-centred approach
It is suggested that a good physician-patient relationship and communication is required to facilitate good patient adherence and persistence with OACs.101) Patients want to be involved in the decision-making process, and wish to feel reassured about the diagnosis, understand the condition sufficiently, and understand the possible side effects of OAC medications.96)
At each follow-up visit, health professionals should assess patient knowledge of AF, OAC risk-benefit and bleeding risk, and check on the patient's current priorities and concerns, and how treatment may impact their quality of life.89)101) It is important to determine any barriers impacting taking medications, including the patient's cognition and memory, and understand the facilitators and assistance that is available to each patient.89) Facilitators that should be considered include their family situation and any support systems available to them.89) Establishing an appropriate medication routine or system is important, and this can improve both adherence and persistence.102)
Family and carer involvement
Involvement of family and caregivers in the development of medication strategies significantly improves adherence.103) Valuable insights can be identified through discussions with family, especially in relation to successful methods for medication management and suitability of alternative strategies and assistance (e.g. Webster packs, pillboxes, and reminders).103) Family can also provide important information pertaining to difficulties or challenges faced by the patient, and relevant beliefs or medication concerns.
Atrial fibrillation knowledge and decision aids
If underlying knowledge deficits exist, or if there are significant beliefs that medications have negative side-effects, medication strategies may not be effective. Additionally, as cognitive impairment is common in patients with AF,104) education and intervention strategies may need to be altered to accommodate the patient's knowledge and/or cognitive deficits. To ensure the information is understood and knowledge is retained, it is important to consider the timing, delivery and choice of education materials. Decision aids for patient education have been shown to improve knowledge and acceptance of treatment and medications, resulting in increased adherence rates.105) These aids could be incorporated into AF education, however it is essential to consider the patient perspective during this process.89)
Electronic reminders and apps
Assistance required by younger people will generally differ from that required by older populations. In a younger population, where forgetting to take medications can be a primary cause of poor adherence, especially due to busy work or social schedules, reminders and systems are likely to assist. However, if the adherence issue is more deeply related to anxiety, medication concerns, a fear of bleeding or impact on activities of daily living, then reminders and alerts are unlikely to work, and a different approach is warranted.
A meta-analysis of text messaging studies for medication adherence in people with chronic disease showed that text messages significantly improved medication adherence (OR, 2.11; CI, 1.52–2.93).106) However these text studies generally included younger people with a mean age of 39 years (range, 31–64 years).106)
Medication apps have been shown to significantly increase adherence to cardiac medications compared to usual care in a middle-to-older age sample (mean age, 58 years).107) Medication apps are often divided into 1) basic apps using reminder strategies only, such as alarms and push notifications; and 2) more advanced apps using behavioural and educational strategies.108) Advanced apps often use behavioural strategies such as external monitoring, personal tracking, and gamification.108) These advanced apps often include additional features such as tracking of health metrics, appointment reminders, refill reminders, ability to record medical history, and pharmacy information.108) However, a recent randomised control study identified no difference in medication adherence rates between the basic and advanced apps.107)
Electronic monitoring
Electronic monitoring tools provide real-time monitoring of exact medication taking behaviour and provide this information to the health professional. They are particularly useful for pinpointing patterns of poor adherence.109) Although more expensive than other options, these interventions have been shown to be successful for people with very poor adherence. A systematic review of electronic monitoring tools demonstrated a positive improvement in medication adherence with use of these tools, over follow-up periods ranging from 7- to 26-weeks.110)
These systems use electronic sensors which transmit to a receiver and record information on the exact time medications are taken.111) Available tools include ‘smart pill boxes’ which record lid opening; ‘wearable sensors’ which work in conjunction with smart pill boxes and detect actions such as hand-to-mouth movements and pill swallowing; ‘ingestible biosensors’ detecting pill ingestion; ‘computer vision’ which can detect medications presence through images captured by the camera; and ‘radio frequency identification’ systems which communicate with a device (e.g. smartphone) in close proximity, and provide an alert, such as a flashing light, when medications need to be taken.111) The ideal tool needs to be determined with consideration given to the patient's personal circumstances and needs.
In conclusion, the management of stroke risk among patients with AF has been a rapidly-evolving area over the past decade. The review findings show that clinicians' management is increasingly reflecting guideline recommendations, with a greater proportion of high-risk patients (CHA2DS2-VASc≥2 men; ≥3 women) receiving OACs over the past decade. However, there is still significant room for improvement in management, as 25–35% of high-risk patients are still not prescribed OAC. Since the introduction of NOACs between 2010–2014 in most countries, and guideline preference for NOAC as first line therapy for high-risk patients, clinicians are prescribing NOACs in preference to warfarin.
Despite better prescription, patient persistence and adherence with OACs long term is poor, with 2-year persistence as low as 50% in many countries. In addition to OAC-related factors such as a fear of bleeding, difficulty with monitoring, and dietary restrictions related to warfarin; multiple other patient-level factors exist which contribute to poor adherence and persistence. A detailed review of each patient, and better understanding of the factors impacting adherence, will assist to direct appropriate interventions to improve both adherence and persistence and reduce stroke-risk. Overall, the results highlight the interplay of both clinician's awareness of guideline recommendations and understanding of the individual patient level factors in reducing the population prevalence of stroke attributable to AF.
 XML Download
XML Download