

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The prevalence of childhood obesity has markedly increased worldwide over the past 30 years. The prevalence of obesity in children in the inner northern region of Turkey is 10.4%, which is comparable (3.7–15.4%) with that in many other countries [1234]. This increased prevalence of obesity has led to a rise in the incidence of metabolic syndrome (MS).
Obesity is due to an imbalance between food intake and energy expenditure, and increased fat storage results in high positive energy balance. Obesity is a multifactorial syndrome influenced by genetic and environmental factors, and it affects millions of people worldwide. Recent studies have focused on genetic and environmental factors (dietary and lifestyle habits, sociological factors, and metabolic and neuroendocrine alterations) [56] that affect the energy balance in children and adolescents [78].
Identification of the major susceptibility locus might be essential for elucidating the pathophysiology of a disease, especially in obesity. Recent studies have contributed to further expand the knowledge regarding obesity-related genetic factors, and novel advance molecular biology techniques have accelerated the search for genes related to energy expenditure, such as those encoding adrenergic receptors and mitochondrial uncoupling proteins [910].
The β3-adrenergic receptor (ADRB3) plays a pivotal role in catecholamine-stimulated thermogenesis and lipolysis. A missense mutation in the ADRB3 gene, Trp64Arg, results in the substitution of a tryptophan with an arginine in the first intracellular loop of ADRB3 [1112]. Walston et al. [13] reported that the ADRB3 Trp64Arg variant is associated with early onset type 2 diabetes mellitus and low resting metabolic rate in Pima Indians. ADRB3 Trp64Arg polymorphism was demonstrated to be associated with obesity [1114151617] and increased tendency to gain weight [181920]. However, studies on this association have reported contradictory results. Other researchers have reported that ADRB3 polymorphism exhibits no effect on obesity, type 2 diabetes [21222324], or energy expenditure in obese post-menopausal women [25].
In recent studies with obese children, ADRB3 trp64arg polymorphism was demonstrated to be significantly associated with MS components, such as increased visceral fat, dyslipidemia, and high blood pressure (BP) [171826]. Although p-3AR genotype was found to be related to insulin resistance (IR), research on the association between sex and W64A polymorphism in obese patients is scarce.
In this study, we aimed to investigate trp64arg polymorphism of the ADRB3 gene in obese children and examine the relationship between this genotype and obesity-related metabolic disorders. The association between ADRB3 genotype and sex was also investigated.
MATERIALS AND METHODS
Participants and study area
A total of obese 264 children and adolescents aged 6–18 years that were followed at the Hospital of the School of Medicine at Gaziosmanpasa University, Tokat-Turkey, were enrolled in the study. Approximately 179 non-obese school-aged children recruited from pediatric clinics constituted the control group. The study protocol was in accordance with the Helsinki Declaration of the World Medical Association and ethical standards. Ethical approval was received for this study from the ethics committee of Gaziosmanpasa University School of Medicine (14-KAEK-204). Informed consent was obtained, and the questionnaires used to gather information about the children were answered by the parents and themselves. This study was conducted prospectively between March 2015 and January 2016.
Definition of obesity, hypertension, insulin resistance, and dyslipidemia
Participants were diagnosed as obese according to body mass index (BMI) SDS, which takes into account the growth curve for each sex and cutoff points proposed by the World Health Organization (WHO) [27]. Weight was measured using a digital scale (Seca Co., Chino, CA, USA) with patients wearing light clothing. Height was measured using a portable stadiometer (Seca). BMI was calculated as weight in kilograms divided by height in meters squared (kg/m2). A patient was considered obese if his or her BMI was >95th percentile [28]. The BMI percentile curve for Turkish children was used to determine obesity [29]. BP was measured using a standard digital sphygmomanometer (0 mron705IT; Omron Electronics, Ltd., Hoffman Estates, IL, USA) and an appropriate collar based on the Fourth Report on the Diagnosis, Evaluation, and Treatment of High BP in Children and Adolescents, considering sex, age, and height percentile, as follows: normal BP (systolic and diastolic BP <90th percentile), prehypertensive (90–95th percentile), and hypertensive (BP >95th percentile) [282930].
Laboratory tests
Blood samples were collected in the morning following a 10–12 h overnight fasting to measure serum levels of fasting glucose (FG), total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol, and triglycerides (TGs) using enzymatic methods and an autoanalyzer (COBAS 6000; Roche Diagnostics, Indianapolis, IN, USA). Dyslipidemia was defined according to the TC, HDL-C, and TG levels. The TC cutoff value used was the accepted laboratory normal range. The other cutoff values were HDL <35 mg/dL, TG >150 mg/dL, and FG >110 mg/dL. Abnormal glucose homeostasis was determined according to the FG level, homeostasis model assessment of insulin resistance (HOMA-IR), and oral glucose tolerance test values. HOMA-IR was calculated according to the Levy formula: FG×fasting insulin/22.5; [31] IR was considered to be present if the value was >3.16 [32]. The patient was considered to have abnormal glucose homeostasis if FG was >110 mg/dL or the 120 minutes glucose level ranged from 140–200 mg/dL [32]. MS was defined according to the modified WHO criteria adapted for children [33], and patients were diagnosed with MS if they met three of the following four criteria: (i) obesity; (ii) abnormal glucose homeostasis; (iii) hypertension; and (iv) dyslipidemia [33].
Genetic analysis
DNA was extracted from peripheral blood samples using ExgeneTM Blood SV Genomic DNA Kit according to the manufacturer's instructions (GeneALL®; Biotechnology Co., Ltd., Seoul, Korea). The ADRB3 trp64arg gene polymorphisms were analyzed by polymerase chain reaction (PCR)-based restriction fragment length polymorphism. PCR was performed in a total volume of 25 µL containing 25–50 ng of genomic DNA, 0.8 nmol/µL of each primer, 1.5 mM MgCl2, 2.5 µL of 10× PCR buffer, 0.3 mM dNTP, and 1 U Taq DNA polymerase (Fermentas, Shenzhen, China). The PCR primers, PCR protocol, product sizes, and restriction enzymes are shown in Table 1. The amplified products were run on 3% agarose gel, stained with ethidium bromide, and visualized under ultraviolet light.
Table 1
PCR primers, PCR protocol, product sizes, and restriction enzymes for ADRB3 trp64arg polymorphisms

Statistical analysis
Data are expressed as the mean±standard deviation or frequency and percentage. Independent sample t-test was used to compare the continuous normal data between groups. Chi-square test was conducted to compare the categorical data among groups. The χ2 test was used to evaluate the Hardy–Weinberg equilibrium for the distribution of the genotypes of the patients and the controls. The p<0.05 was considered statistically significant. Analyses were performed using SPSS version 19.0 (SPSS Inc, Chicago, IL, USA).
RESULTS
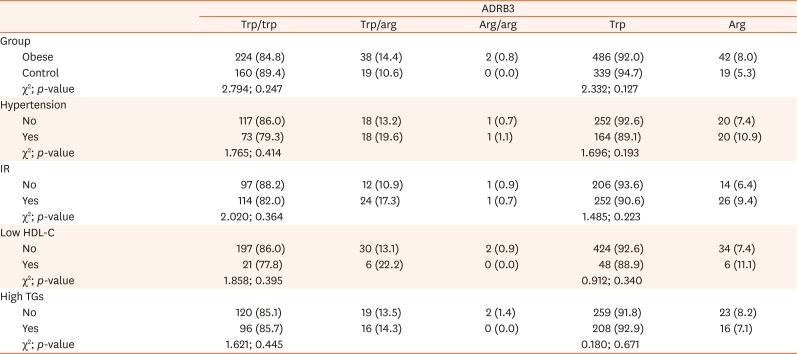
The demographic and clinical characteristics of the study groups are given in Table 2. The screened ADRB3 genotypes were not different between the obese and control groups, and the frequencies of trp/trp, trp/arg, and arg/arg genotypes were 86.0%, 13.2%, and 0.7% in the obese group and 89.4%, 10.6%, and 0.0% in the controls, respectively (p=0.896). The allele frequencies were also similar (p=0.95; Table 3).
Table 2
Clinical and laboratory characteristics of study participants
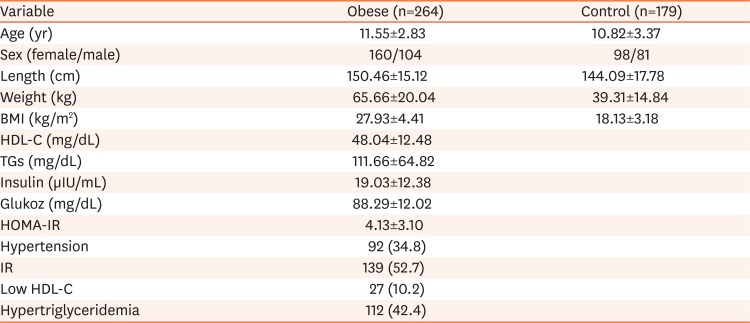
Table 3
Clinical characteristics of study participants according to the genotypes of ADRB3 polymorphisms
Genotypic distribution satisfied the Hardy–Weinberg equilibrium (χ2, p=0.9998) in the obese group.
No relationships between the polymorphism genotypes and lipid levels or HOMA scores were found in obese children (Table 4).
Table 4
Means of quantitative variables based on ADRB3 genotypes
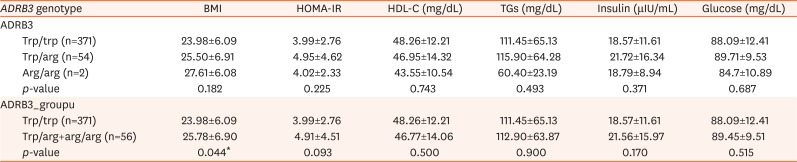
Values are presented as mean±standard deviation.
ADRB3: β3-adrenergic receptor, BMI: body mass index (kg/m2), HOMA-IR: homeostasis model assessment of insulin resistance, HDL-C: high-density lipoprotein cholesterol, TGs: triglycerides, Trp: tryptophan, Arg: arginine.
*The difference is statistically important.
A total of 107 of 264 obese cases had IR. Polymorphism frequency was not different between children who had or did not have IR (p=0.140; Table 5).
Table 5
Distribution of ADRB3 gene based on qualitative variables (in all groups)
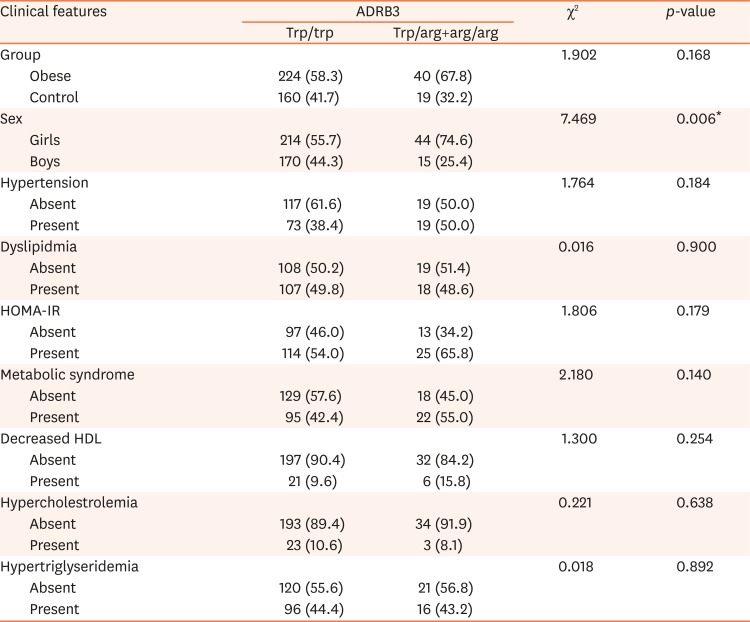
The distribution of the ADRB3 gene according to sex is illustrated in Table 6.

DISCUSSION
Results of studies on association between trp/arg polymorphism of the ADRB3 gene and obesity in children are contradictory. In this study, we investigated the association between trp/arg polymorphism in the ADRB3 gene and both obesity and obesity-related disorders in Turkish children and adolescents. Our study revealed that the trp/arg and/or arg/arg polymorphism of the ADR3 gene was not associated with obesity in Turkish children and adolescents. However, a statistically significant difference was found between boys and girls. Obesity was more prevalent in girls than in boys, and a positive correlation was noted between heterozygosity and BMI.
The sympathetic nervous system plays a crucial role in regulating energy expenditure. Reduced resting metabolic rate and energy expenditure are predictive markers of obesity (weight gain). Catecholamines, which serve as mediators of the sympathetic nervous system, are also important regulators of lipolysis and function through β1–β3 adrenergic receptors. The effects of adrenergic receptors on adipose tissue are regulated by thermogenesis. ADRB3 trp64arg polymorphism is associated with weight gain, increased visceral fat, abdominal obesity, and difficulty in losing weight [1214151617203435]. However, several studies have reported contradictory results [2122232436]. A recent Brazilian study reported that high HOMA-IR scores and presence of MS are associated with trp/trp genotypes in obese and hypertensive adults [36], and such inconsistencies might be partially explained by ethnicity, age, or population differences in the studied samples. In a twin study with a high similarity in genetic and environmental background, the risk of obesity, IR, or type 2 diabetes unexpectedly increased with heterozygosity for ADRB3 trp64arg [37]. Recent studies on obese children revealed no relationship between HOMA-IR and ADRB3 genotype similar to our present study [151723].
Another study demonstrated that trp64arg polymorphism is significantly associated with the three key components of MS in obese children, namely, increased visceral fat accumulation, aggravated lipid metabolism, and hypertension [1738]. Similar to our results, Urhammer et al. [39] and Li et al. [40] did not find an association between heterozygosity and obesity. In addition, they found no differences between heterozygotes and homozygotes for the wild-type allele in BMI, body fat distribution, fat cell size, fasting levels of insulin, glucose, or lipids, BP, or adipocyte lipolysis in isolated white fat cells [3940].
In the present study, our results revealed no relationship between ADRB3 genotype and obesity in children. Moreover, trp64arg polymorphism of the ADRB3 gene was not associated with obesity-related parameters, such as IR, dyslipidemia, and hypertension. In addition to its effect on lipolysis and biological energy production, ADRB3 might modulate peripheral vascular tone and increase BP [38]. Some clinical studies have indicated a possible relationship between arterial hypertension and trp64arg polymorphism of the ADRB3 gene, as well as a relationship between this genotype and high mortality among hypertensive patients [4142]. Another study revealed that obesity and hypertension are related to polymorphisms in the ADRB3 gene [34].
Sympathetic nervous activity is related to body weight or BP through β-adrenoceptors. ADRB3 might modulate peripheral vascular tone and increase BP [38]. In a recent study conducted in Japanese children, Trp64Arg polymorphism of the ADRB3 gene was found to affect visceral fat accumulation, and is associated with high BP in the same subjects [17]. Another study from Japan reported no association between Trp64Arg polymorphism and high BP in children [18]. However, this result should be interpreted with caution because our study does not represent all Turkish children.
Nonetheless, our results are consistent with previous studies conducted to investigate the association between the ADRB3 trp64arg polymorphism and BMI [1243]. BMI increases with age through adolescence, and the age-related changes in BMI differ between males and females [44]. A previous Brazilian study involved more females than males, similar to our present study, in which the trp64arg group (85%) was greater than the trp64trp (68%) group [36]. However, recent studies showed that trp64arg carriers are more common in boys than in girls [1516]. Thus, BMI-related analyses possibly yielded different results between our study and previous studies conducted in adults and children. Other possible explanations for our different results include the following: (i) racial, ethnic, and lifestyle differences between Turkish subjects and those from other ethnicities, (ii) limitations in any association study that analyzes polymorphisms of only one gene in the analysis of complex disorders, such as obesity, (iii) no relationship exists between the trp64arg allele and early onset obesity; significant weight gain in trp64arg homozygous or heterozygous obese individuals has previously been shown to occur after adolescence [12]; results of some studies suggested that different genes are involved in weight regulation depending on the age [45], and (iv) mutation of ADRB3 in its heterozygous form has a negligible effect on body weight [39].
In conclusion, our study results can aid in elucidating the mechanism underlying complex diseases, such as obesity. Long-term follow up of obese and overweight children might clarify the interactions between the genetic bases of obesity, such as polymorphism and metabolic consequences, or comorbidities of obesity, such as IR, dyslipidemia, and hypertension. Future studies will be necessary to assess the possible associations between sex and the ADRB3 gene and identify ADRB3 polymorphism as a new risk factor of childhood obesity and related disorders.
 XML Download
XML Download