

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Jaundice is the most common medical condition occurring within a few days after birth in newborns. Physiologic jaundice during the first week of life is seen in approximately 60–80% of neonates [123]. Two factors may lead to high levels of unconjugated bilirubin, including sterile intestines of neonates at birth, in which conjugated bilirubin cannot be converted to stercobilin or urobilirubin to be excreted from the body; and the conversion of bilirubin back to the unconjugated form by intestinal beta-glucuronidase enzyme in some neonates. Neonate feeding assists in the establishment of a normal intestinal flora and enhances meconium passage. Meconium contains abundant bilirubin. In cases of delayed feeding or inability to excrete meconium, beta-glucuronidase exposure is prolonged in the intestine, elevating the possibility of converting unconjugated bilirubin to the conjugated form [23]. Inadequate fluid intake, significant weight loss, and decreased bowel movements may also increase neonatal risk of hyperbilirubinemia [2].
Phototherapy is the most common intervention for neonatal hyperbilirubinemia. It reduces the level of total bilirubin or slows down its accumulation in almost all patients, regardless of the cause [4]. While considered to be safe, many possible side effects include transient erythematous rash, loose stools, hyperthermia, dehydration [5], and gray baby syndrome [6]. The mother and baby can suffer psychologically and emotionally, due to the physical separation during phototherapy [78]. Although blood transfusion is expensive and time consuming, it is the most effective method for the rapid removal of excess bilirubin from circulation [4]. The mortality and morbidity associated with blood transfusions is not fully understood [8].
Elevated serum total bilirubin can result in bilirubin encephalopathy that leads to kernicterus with a risk of permanent severe neurodevelopmental disabilities or death.
Herbs from shatru, jujubes, manna and clay are also used for the treatment of hyperbilirubinemia in Iran [9]. Another treatment for elevated bilirubin levels is the intake of probiotics. Probiotics are live microorganisms that, upon consumption, have beneficial effects on the microbial flora. Most probiotics belong to a large group of bacteria that commensally live in the human gut flora [1011]. The main effect of probiotics is to stabilize the intestinal microflora. Constant consumption of probiotics has been observed to reduce the incidence of various diseases; hospitalized children and those who do not consume milk or are living in deprived conditions are vulnerable to diseases. Probiotic products are available for sale in the commercial market in the form of tablets, capsules, powders, fortified yogurt, milk and cheese [12]. Apart from the effect of probiotics in the treatment of hyperbilirubinemia, they are also used for the treatment of children with acute diarrhea, necrotizing enterocolitis, and allergies [131415]. This study aimed to investigate the effect of synbiotics on hyper-bilirubinemia treatment in term neonates.
MATERIALS AND METHODS
This study is a clinical trial conducted on 83 full-term and exclusively breast-fed neonates without pathologic jaundice, who were admitted to Shahid Madani Hospital, Khorramabad, Iran, in the first 6 months of 2015, with serum bilirubin levels between 15 and 20 mg/dL. Those suffering from sepsis, fauvism, congenital anomalies, asphyxia, heart disease, and intrauterine growth restriction were not included in the study. The neonates were randomly placed into two groups: synbiotic (SG, n=40) and control (CG, n=43). Randomization was carried out using sequential numbers obtained from the computer center of the neonatal ward. The CG underwent only routine treatment of hyperbilirubinemia (i.e., phototherapy). For phototherapy, fluorescent lamps were used in the neonatal ward and the eyes and genitals of newborns were covered. The distance between fluorescent lamps and babies was 30–50 cm. For every two hours of phototherapy, there was a half hour break from phototherapy devices while neonates were breastfed with open eyes.
The neonates in the SG received 5 drops/day of synbiotics (Pedilact drop; Zist-Takhmir Co., Tehran, Iran) in addition to routine phototherapy. For sanitary purposes, each neonate had separate stocks of synbiotics stored at 2–8°C in the refrigerator. Synbiotics were often placed at room temperature for 10 minutes prior daily administration.
The serum bilirubin levels were measured daily for feeding, urine and stool frequency in both groups. The weight (grams) of neonates was also measured daily. Those with bilirubin levels <11 mg/dL were discharged. This study was approved by the Research Ethics Board of Lorestan University of Medical Sciences (IRCT Code. IRCT2015112925287N1).
Data analysis
Descriptive statistics were evaluated as means, standard deviations, and frequencies. To compare statistics, repeated measures analyses and t-tests were used with a significance level of <0.05. Data were expressed as mean±SEM (standard error of the mean). To evaluate the hypothesis of equal variance in outcomes, a covariance matrix for random effects was used.
RESULTS
In this study, 83 full-term neonates with hyper-bilirubinemia were striated into two groups: SG (n=40) and CG (n=43; Fig. 1). The final bilirubin level was 9.38±2.37 and 11.17±2.60 mg/dL in SG and CG, respectively. The average length of hospitalization in the SG and CG was 2.5±0.58 and 2.9±0.89 days, respectively. The mean and SEM values of both groups are shown in Fig. 2. The effects of synbiotic intervention on bilirubin levels, urine frequency and defecation were statistically significant compared to CG (p<0.05). In the SG, mean total bilirubin levels were lower (0.62 vs. 0.73 mg/dL), while urine (6.860 vs. 5.500 times per day) and stool frequency (5.528 vs. 3.903 times per day) were significantly higher compared to controls (Fig. 3).
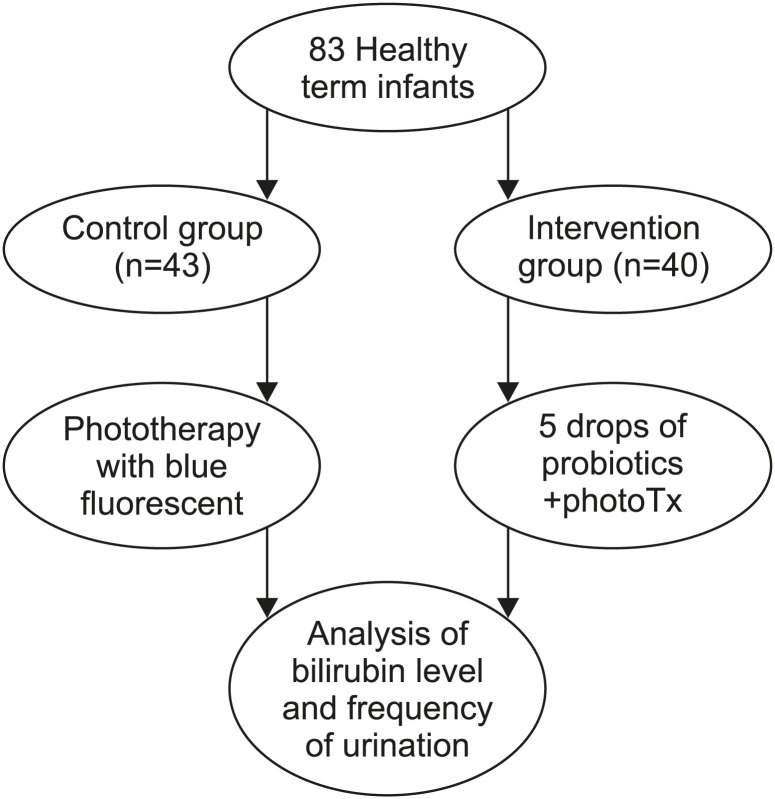
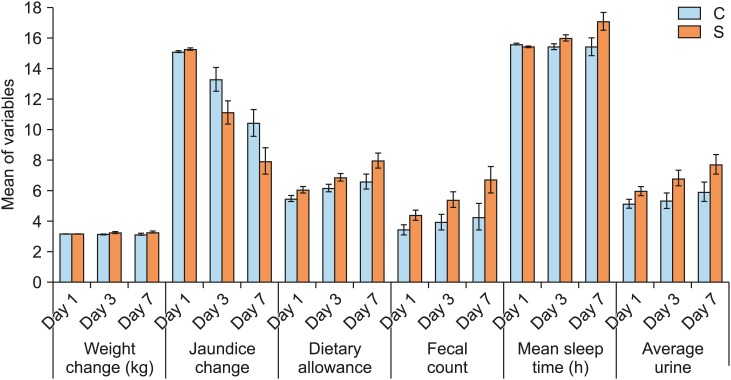
Fig. 2
Variables examined in the synbiotic (S) and control (C) groups (mean±standard error of the mean).

Fig. 3
Variables examined in the symbiotic (S) and control (C) groups during hospital stay (mean±standard error of the mean).
According to Table 1, it was observed that there is a significant difference between the average number of days of hospitalization between the groups. The average number of days of hospitalization in the probiotic group was lower than the control group. There was a significant difference in the bilirubin levels, frequency of stools, feeding and urine frequency in both groups during hospital stay (p<0.05; Fig. 3). The mean frequency of defecation and total levels of bilirubin were significantly different between-groups (p<0.05). The frequency of feeding was higher in the synbiotic group as compared to control group. For all the above-mentioned parameters at three different times, the bilirubin level, defecation, urine frequency and feeding, there was a significant difference (p<0.05) observed. There was no significant difference within the groups studied.

DISCUSSION
The present study investigated the effects of probiotic-supplemented phototherapy compared with phototherapy alone during hyperbilirubinemia treatment in term neonates. Hyperbilirubinemia is one of the most frequent problems in newborns and 60% of term neonates encounter jaundice in the first week of life. Elevated amounts of unconjugated bilirubin in the serum and across the blood-brain barrier result in bilirubin encephalopathy, kernicterus and a risk of permanent severe neurological impairments [161718].
A meta-analysis conducted by Chen et al. [19], systematically evaluated the safety and efficacy of probiotic supplementation for pathologic neonatal jaundice, and showed that it was a safe and efficient treatment for pathological neonatal jaundice. In a systematic review by Deshmukh et al. [20], the safety and efficacy of probiotics in reducing the need for phototherapy and the duration for neonatal hyperbilirubinemia was assessed. Limited low-quality evidence showed that the supplementation of probiotics may decrease phototherapy duration in neonatal jaundice. The routine use of probiotics as preventive measures or for the treatment of neonatal jaundice would be recommended.
In a study using probiotics in combination with phototherapy, there was a decrease in the length of hospitalization for neonates with hyperbilirubinemia and no adverse effects were detected [21]. In another study, probiotic yeast were administered daily in premature neonates with a birth weight under 1,500 grams. Short-term intake of probiotics decreased the length of phototherapy, by improving intestinal transit time and inhibiting reabsorption of bilirubin [4]. Lactobacillus acidophilus consumption in experimental animal models reduced enzyme fecal activities including nitroreductase, glucuronidase, and azoreductase [2223].
Newborns that are breastfed may be vulnerable to early-onset exaggerated physiologic jaundice due to the relative deprivation of calories during the first few days of life [24]. A reduced amount and feeding frequency may result in mild dehydration and delayed meconium passage. As compared to formula-fed newborns, breastfed infants are 3-6 times more vulnerable to jaundice (<12 mg/dL) or severe jaundice (<15 mg/dL [257 µM/L]) [2526].
In the present study, there was no initial difference in weight, bilirubin levels, defecation, feeding, sleep, or urination before the commencement of the study. However, following the administration of treatment and observation at days 1, 3, and 7, the subjects gained weight, but this difference was not significant (p>0.05). There was a sharp decrease in the level of bilirubin in the treatment group on the 7th day compared with the control group, showing that the intervention method was effective (p<0.05). However, the frequency of defecation, feeding, sleep and urination significantly increased (p<0.05; Fig. 2).
In conclusion, this study showed a reduction in hyperbilirubinemia and length of hospitalization using synbiotics as an adjuvant therapy. Further studies, involving larger sample sizes and with longer follow-up, are required to validate the routine use of synbiotics in neonatal jaundice.
 XML Download
XML Download