

 PDF
PDF ePub
ePub Citation
Citation Print
Print



I. Introduction
Sagittal split osteotomy (SSO) is the most commonly performed osteotomy for correction of class II or class III skeletal deformities. One of the common complications of SSO is inferior alveolar nerve (IAN) injury, which presents as postoperative numbness in the lower lip and mental area1. The prevalence of postoperative paresthesia following SSO ranges from 9% to 84.6%2. IAN injury defined as both direct and indirect operative trauma. This trauma results in changes in sensibility or other forms of altered sensation of the lower lip and/or mental region3. In addition, injury to the IAN is unpredictable even when surgery is performed by an expert surgeon4.
Sensory disturbances following SSO have the potential to affect patient performance because of their effects on speech, eating, drinking, and social interactions5. Patient complaints regarding sensory disturbances are important issues faced by surgeons after SSO. Reported paresthesia after SSO can be considered a determining factor of the severity of nerve injury after osteotomy6.
Various factors have been suggested to be responsible for the development of IAN injury after SSO, including the fixation method, patient age, the surgical procedure, improper splinting, magnitude of mandibular movement, experience of the surgeon, and timing of postoperative neurosensory evaluation4. In addition, the IAN may be distracted or compressed based on movement of the distal segment of the mandible in class II or class III deformities. The fixation method (positional screws or miniplates) may affect the frequency of paresthesia7. The placement of semi-rigid fixation plates and screws may result in nerve injury either directly or through compression of the nerve between bony segments after fixation8.
Clinical diagnosis of neurosensory disturbances after SSO is mostly based on clinical sensory testing. Examinations can be either mechanoceptive or nociceptive9. Clinical examination is sometimes difficult because of the heterogeneity of the methods, variability in the definitions of neurosensory disturbance, and change over time during follow-up10.
The reliability of subjective reporting is controversial. Subjective reports are used widely to evaluate postoperative paresthesia because of the lack of objective factors in the diagnosis of sensory nerve damage11. It has been suggested that paresthesia and sensory disturbance after SSO are primarily overestimated, but may be underestimated with increasing time from surgery. It seems that patients adapt or become accustomed to what they consider “normal” over time. Normal sensation was different among patients in various studies12. Debate continues over which type of evaluation (sensory testing or patient reporting) should be used to assess nerve injury and recovery13. If evaluation is used for decision-making regarding microsurgical nerve repair, electrophysiological assessment of nerve integrity or stimulus detection measures may be valuable. Patient adaptation to altered sensitivity1415 or the effects of medication16 can be evaluated by stimulus perception or self-report13.
We hypothesized that paresthesia occurs in patients with class II skeletal deformities more than in patients with class III deformities and also in patients in whom positional screws are used for fixation. The aim of this study was to compare the amount of postoperative paresthesia in patients with class II and class III skeletal deformities with different fixation methods including the use of positional screws or miniplates.
Go to : 
II. Materials and Methods
The authors designed a prospective cohort study. The sample was derived from a population of patients treated at the Oral and Maxillofacial Surgery Department of Shiraz University of Medical Sciences (Shiraz, Iran) between September 1, 2012 and October 31, 2014. The research was approved by the Medical Ethics Committee of Shiraz University of Medical Sciences (approval No. 8793062). Also, all procedures followed the policies and principles of the Declaration of Helsinki during all clinical procedures.
The authors designed a prospective cohort study. The sample was derived from a population of patients treated at the Oral and Maxillofacial Surgery Department of Shiraz University of Medical Sciences (Shiraz, Iran) between September 1, 2012 and October 31, 2014. The research was approved by the Medical Ethics Committee of Shiraz University of Medical Sciences (approval No. 8793062). Also, all procedures followed the policies and principles of the Declaration of Helsinki during all clinical procedures.
Subjects were divided into four groups; Group 1: patients with a class II skeletal deformity that underwent miniplate fixation of each osteotomy site, Group 2: patients with a class II skeletal deformity that underwent fixation by three positional screws at each osteotomy site, Group 3: patients with a class III skeletal deformity that underwent miniplate fixation at each osteotomy site, and Group 4: patients with a class III skeletal deformity that underwent fixation by three positional screws at each osteotomy site.
The amount of mandibular movement was assessed via lateral cephalogram. The change in the distance between the upper and lower incisors was measured before and immediately after surgery.
All patients were followed one year postoperative.(Table 1) To assess the level of paresthesia, visual analogue scale scores were interpreted as follows: 0 to 2 mild discomfort, 2 to 4 mild to moderate discomfort, 4 to 6 moderate discomfort, 6 to 8 moderate to severe discomfort, and 8 to 10 severe to intolerable discomfort2.

Table 1
Sex and age of the patients and the amount of mandibular movement in the four groups
![]()
1. Surgical approach
The surgical method described by Epker17 was followed. An incision was made over the anterior portion of the vertical ramus, extending to the mesial aspect of the first molar.
Subperiosteal dissection was carried down to the inferior border of the mandible, where a lateral channel retractor was placed. A long bur was used to make a horizontal bone cut through the medial cortex of the ramus, just above and approximately posterior to the lingula. The medial osteotomy line was extended 3 to 4 mm beyond the lingula. The vertical cut was made through the buccal cortex, distal to the second molar or further anterior. The two osteotomies were then connected with a #701 fissure bur. A spreader and a narrow osteotome were used to gently lift the lateral cortex, and the osteotome was used to create a step along the connecting cut to ensure that the split remained close to the lateral cortex. Patients in groups 1 and 3 underwent fixation with a four-hole miniplate with a bar and four screws at each osteotomy site. In groups 2 and 4, patients underwent fixation with three positional screws using a trocar.
2. Statistical analysis
Statistical analyses were performed using the IBM SPSS Statistics software (ver. 19; IBM Co., Armonk, NY, USA). ANOVA was used to compare age, the amount of mandibular movement, and the level of paresthesia among groups. The chi-square test was applied to compare sex among groups. The Pearson correlation test was used to assess associations of age and amount of mandibular movement with paresthesia. Pairwise comparison of groups in terms of paresthesia was performed using Scheffe's post hoc test. We considered P-values <0.05 statistically significant.
Go to :
III. Results
Eighty subjects were divided into four groups with 20 subjects in each group. Mean age (±standard deviation) was 22.76±4.21 years and mean mandibular movement was 4.12±0.89 mm. Analysis of the data did not demonstrate a significant difference in sex, age, or mandibular movement among the studied groups (P<0.05).(Table 1) The mean level of paresthesia was 3.12±2.15. Pearson correlation demonstrated a significant correlation between mandibular movement and paresthesia (P=0.001). There was no correlation between age and paresthesia (P>0.05).
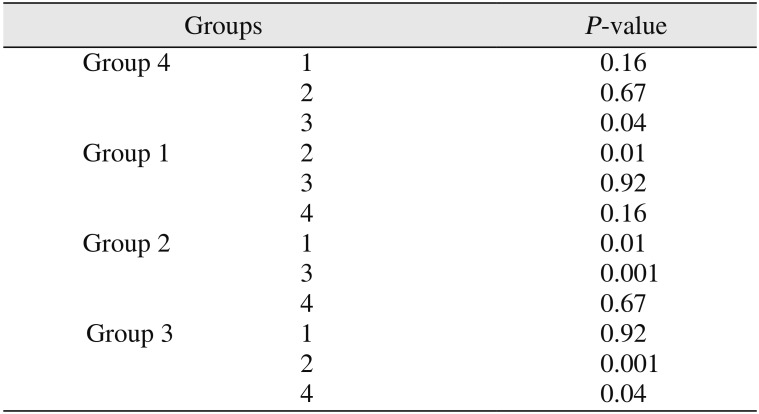
The mean level of paresthesia was 2.82±1.87 in males and 3.30±2.30 in females (P>0.05). The mean level of paresthesia was 2.40±1.70 in Group 1, 4.40±2.23 in Group 2, 2.00±1.29 in Group 3, and 3.70±2.40 in Group 4. Comparison of paresthesia among these groups showed a significant difference (P<0.05). Further post hoc testing revealed a significant difference between groups 1 and 2, groups 2 and 3, and groups 3 and 4.(Table 2)
Go to :
IV. Discussion
Nerve manipulation and retraction for the medial osteotomy cut, the actual splitting procedure, excessive stretching of the nerve during segment manipulation, and compression of the nerve during fixation have been considered factors responsible for nerve disturbance during SSO13. In the current study, we evaluated paresthesia among different skeletal deformities and fixation methods in four groups one year postoperative. The groups had similar age and sex characteristics, and similar mandibular movement.
In the current study, mean paresthesia was higher in screw-type fixations than plate fixations used for both setback and advancement of the mandible. Screw-type fixations are used bicortically, while plates are typically fixed monocortically. An animal study on monkeys showed that nerve injury occurred in both monocortical and bicortical fixation during setback of the mandible via SSO. Although considerable recovery was detected after both forms of fixation at 12 weeks, nerve function was reported to be much better after plate fixation than after screw fixation18.
In the current study, we found a positive correlation between the amount of mandibular movement and postoperative paresthesia. Anatomical characteristics of the mandible such as the intrabony course of the mandibular canal or thickness of the bone at the osteotomy site may also increase the risk of nerve disturbance during SSO19. The close contact between the mandibular canal and the external cortical bone increases the risk of neurosensory disturbances as well20. The prevalence of nerve injury after SSO in class III cases is dependent on the position of the mandibular canal and the size of the mandibular angle21. Mandibular anatomy varies in retrognathia and prognathia. Individuals with retrognathia have a small mandible with a short body and the IAN is stretched during SSO for mandibular advancement. In subjects with prognathia, the mandible is huge with a long body and the IAN is not stretched but may be twisted during SSO. These characteristics may lead to differences in the frequency of nerve disturbance between these two types of deformities. In our study, no differences were detected between class II and class III skeletal patients with regard to postoperative paresthesia, but a positive correlation was seen between the amount of mandibular movement and paresthesia. Ylikontiola et al.22 considered age, the intraoperative magnitude of mandibular movement, and the degree of manipulation of the IAN important factors in nerve dysfunction after SSO.
Clinical neurosensory testing generally consists of two basic types according to the specific receptors stimulated through nociceptive, mechanoceptive, and cutaneous contact. Mechanoceptive testing consists of the two-point discrimination test (TPD), static light touch, and brush directional stroke tests. The pin-prick and thermal discrimination tests are a subgroup of the nociceptive testing group23. In this study, paresthesia was evaluated subjectively (self-reported). The absence of objective data is a main limitation of this study. Improvement of paresthesia in patients who underwent bilateral SSO (BSSO) was attributed to recovery of the IAN or adaptation to changes in nerve function, especially in bilateral paresthesia. It is a disadvantage of self-reported paresthesia as an evaluation test in neurosensory paresthesia. Therefore, future studies are needed to investigate paresthesia objectively.
Go to :
V. Conclusion
According to the results of this study, bicortical fixation by screws can be considered a risk factor for nerve disturbance. Furthermore, although the type of skeletal deformity had no effect on postoperative paresthesia, the amount of mandibular movement had a positive correlation with paresthesia.
Go to :
 XML Download
XML Download