

 PDF
PDF ePub
ePub Citation
Citation Print
Print



I. Introduction
Two implants are considered the minimum necessity to retain a mandibular denture in edentulous patients12. Previous studies have shown that mandibular two-implant-supported overdentures (ISRDs) provide significant enhancement in stability, retention, patient satisfaction, and quality of life3456. ISRDs may be used either with single attachments or attachments splinted together using a cast metal bar and clips7. Several types of single attachments are available for ISRDs such as ball attachments, locators, magnets, and rigid or non-rigid telescopic copings89.
The indications for different attachment systems for ISRDs are well-documented in literature, but some controversial opinions exist101112. However, no significant difference in satisfaction level13141516 and quality of life1718 were reported by patients receiving various attachment types of overdentures except for a few studies concerning magnetic attachments1920.The results of several clinical studies indicate that the retention mechanisms have similar effects on marginal bone levels212223. Still, there is no consensus opinion2425 about the influence of attachment systems on patient satisfaction or marginal bone level maintenance26 around supporting implants. Since overloading of ISRDs may lead to bone loss at the implant-bone interface2728, it is important to evaluate the influence of possible variables on load distribution in bone and around implants. In a recent clinical study, no statistically significant differences were found between single and bar attachment types, although the bone loss rate observed in those with single attachments tended to be lower29. On the other hand, as splinted implants act together as a group, less bone loss due to distribution of the loads by splinting of the implants can be expected30.
Although it is not a common type of implant superstructure, an implant-assisted removable denture (IARD) can be fabricated instead of an ISRD in cases with few anterior implants. In most IARDs, implants are placed under conventional removable partial dentures (RPDs) with abutment teeth to optimize stability and retention of the prosthesis31. This solution has shown a more helpful effect on oral health compared to conventional RPDs3233. While these advantages advocated for IARD treatment in the early 2000s3134, clinical studies evaluating its technical features and performance are scarce. A recent literature review reported that treatment with IARDs is a simple and cost-effective approach, but the absence of robust publications related to IARDs has limited significant conclusions31. Likewise, offering IARDs to edentulous patients as an alternative to ISRDs has been published only in case studies34353637. The consensus that had been reached in these reports34353637 was increased satisfaction due to the resolved need to remove anterior teeth during sleep or oral hygiene maintenance as with ISRDs. With this solution, patients reported increased confidence since the anterior part of the prosthesis is fixed and more comfortable due to reduced denture volume3435. Furthermore, this treatment option fulfills patient desire to show their teeth even after removal of the mandibular denture36. Therefore, this in vitro study was conducted to observe if the stress distribution in the mandible is advantageous for this type of prosthetic alternative or if it has a detrimental effect on force distribution.
Whether this kind of superstructure will reduce or increase maintenance requirements will be the subject of another clinical study. This in vitro study was performed to test different scenarios in terms of the influence of types of attachment and superstructure on stress distribution in the edentulous mandible. The null hypothesis of the study was that IARD and ISRD would not have a significant difference on stress distribution in the edentulous mandible.
II. Materials and Methods
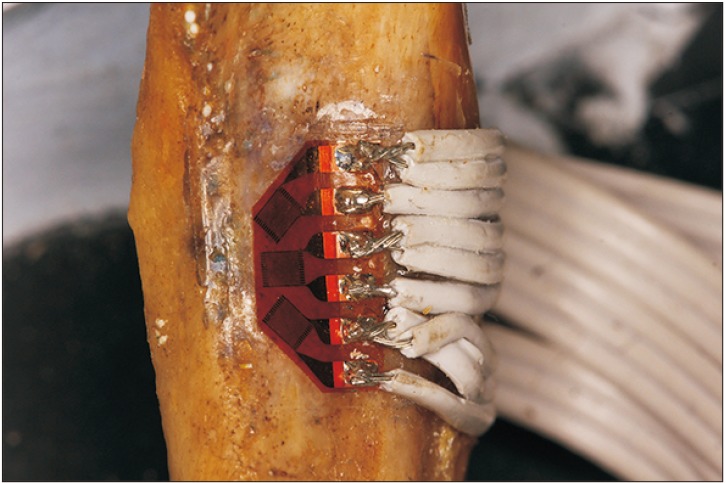
An edentulous mandible from a formalin-fixed human cadaver was selected from the Department of Anatomy, Faculty of Medicine, Istanbul University to use in this in vitro strain gauge (SG) measurement study. After removal of the mandible from the cadaver, locations where the SG rosettes (CEA 125UR, 350 Ω; Vishay Precision Group Inc., Malvern, PA, USA) would be applied were cleaned using pure alcohol. Surface smoothing was accomplished through the two-stage application of sandpaper. Six SG rosettes were applied at the following locations:
1) Right mylohyoid ridge (MRR)
2) Left mylohyoid ridge (MRL)
3) Symphysis midline (SM)
4) Right retromolar pad (RP)
5) Buccal shelf left (BP)
6) Right canine region (C)
The SGs were adapted, bonding material (M-Bond; Vishay Micro-Measurements, Raleigh, NC, USA) was applied to the bone, and the gauges were fastened to the bone to finger pressure. All connections were soldered afterward. After this process was complete, all single elements of the rosettes were circuit balanced and shunt calibrated electronically in situ.(Fig. 1)
A 2-mm-thick polyvinylsiloxane impression material (Affinis light body, Coltene/Whaledent AG, Altstätten, Switzerland) was adapted to the mandible to mimic soft tissue.(Fig. 2) An impression was fabricated from the equipped mandible with soft tissue using a reversible hydrocolloid impression material (Kromopan 100; Lascod, Florence, Italy) and was then filled with dental stone to obtain a working cast. A matching maxillary edentulous cast was selected from those used for pre-clinical education of dental students. Record bases and occlusion rims were prepared on the casts with average height and width values as described previously, and the maxillary cast with the mandible was mounted to a modified semi-adjustable articulator (Artex CT Articulator; Amann Girrbach AG, Koblach, Austria). Anatomically shaped acrylic resin artificial teeth (Trend GD Dent, Sakarya, Turkey) were arranged, and a pair of maxillary and mandibular complete dentures (MCDs) was processed and finished using heatpolymerized polymethylmethacrylate (Meliodent; Bayer UK Ltd., Newbury, UK). One MCD was duplicated from the original with a previously described method23 to create two identical dentures-one to use for the bar attachment situation and one with ball attachments. For fabrication of a surgical template, the mandibular denture was additionally duplicated using a clear heat-cured acrylic resin (Rodex, Rodent, Italy).
1. Surgical procedures
Two 3.8-mm-wide, 11-mm-long dental implants (Xive; Dentsply Sirona, York, PA, USA) were placed in the canine positions with the aid of a template prepared by an experienced oral and maxillofacial surgeon according to the guidelines determined by the manufacturer. During implant placement, special attention was given to obtain successful apicocoronal leveling of implant shoulders.
2. Prosthetic procedures
An implant-level impression was created using the closed impression technique with polyvinylsiloxane impression material (Affinis light body; Coltene/Whaledent AG). Upon removal of the impression, 2 implant analogues (Xive) were placed into the replicas in the impression, and the impression was filled with type IV dental stone (GC Fujirock EP; GC Dental, Tokyo, Japan) to obtain a working cast.
Three attachment types were used to retain the mandibular prosthesis.
1) Screw-retained abutments (Xive) were screwed to the analogues; and a two-implant retained bar was fabricated, screwed to the implants, and attached to the 3 MCDs with autopolymerizing acrylic resin (Meliodent; Kulzer GmbH, Hanau, Germany) after removal of adequate acrylic using a round bur (#140. 277. 040; Acurata Imperial, Thurmansbang, Germany).
2) Ball abutments (Xive) were screwed to the implants and attached to the remaining 3 MCDs with auto polymerizing acrylic resin (Meliodent; Kulzer GmbH) after removal of adequate acrylic using a round bur (#140. 277. 040).
3) A new set of screw-retained abutments (Xive) was added to the implants, and a 6-unit, anterior, metal fused to porcelain fixed bridge with extra coronal precision attachments and a bilateral distal extension RPD (Fig. 3) were fabricated38. Bilateral extracoronal precision attachments were used (Vario Soft 3; Bredent GmbH & Co.KG, Senden, Germany).
3. Experimental procedures
The modified semi-adjustable articulator together with the mandible that had been provided with SGs was placed under a universal testing machine (MTS Bionix-II Axial/Torsional Test System; MTS, Eden Prairie, MN, USA), and occlusal forces were applied thorough the center of the maxillary model. For strain data acquisition, a multichannel, multipurpose, universal data acquisition system (Model 8048, 128 Channel Configuration; Prosig, Fareham, UK) was used. The strains were collected in synchronization with the axial force values obtained from the MTS Controller Unit. A 40-kg load cell (ESIT, Istanbul, Turkey) was used for optimum force measurement accuracy during the tests. Quasi static tests were subsequently conducted 10 times for each implant, and attachment configurations were performed at each of the replicated “biting” conditions: centric occlusion and left and right chewing positions. The loading and unloading rates were both 7 N/s. To exclude possible minor misalignment errors due to assembly and production tolerances, a preload of 5 N was placed on the system as the reference state. Each member of the strain rosette represented a one-quarter bridge. Accordingly, a total of 18 channels of data were gathered. Thermal drift was not observed during any tests.
4. Statistical analyses
For statistical analysis of the results, IBM SPSS Statistics (ver. 21; IBM Corp., Armonk, NY, USA) was used to analyze the measured strains from 6 SGs at 3 different loading conditions. Comparison of quantitative data was accomplished with the Mann-Whitney U test for groups without normal distribution. For comparison of the 3 denture types, the Kruskal-Wallis test was used. The results were assessed at a 95% confidence interval for a significance level of 0.05.
III. Results
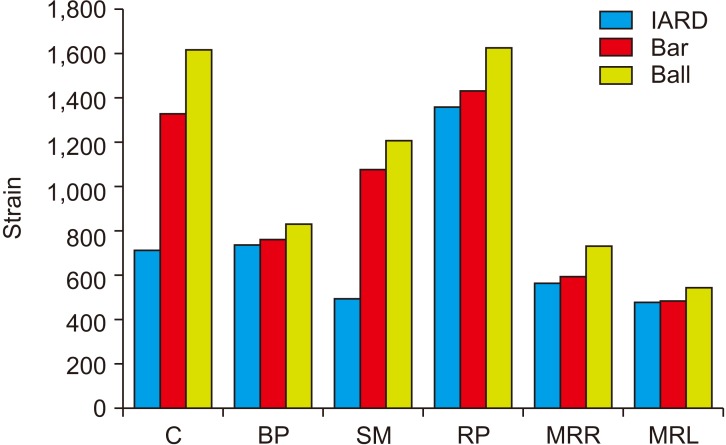
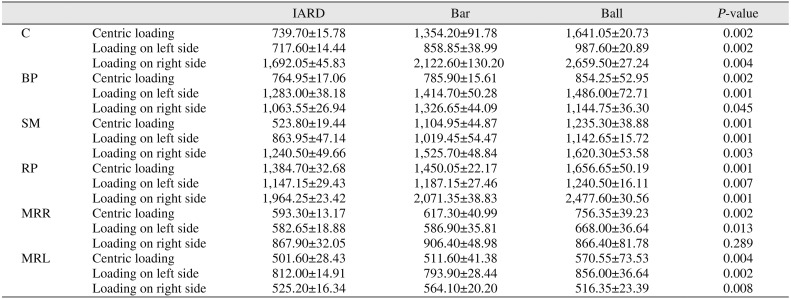
The lowest strain values were measured in the IARD. The only exception was the MRL region for the ball attachment situation (136.55), whereas the highest value was observed in the C region for the ball attachment situation (1,941.05).
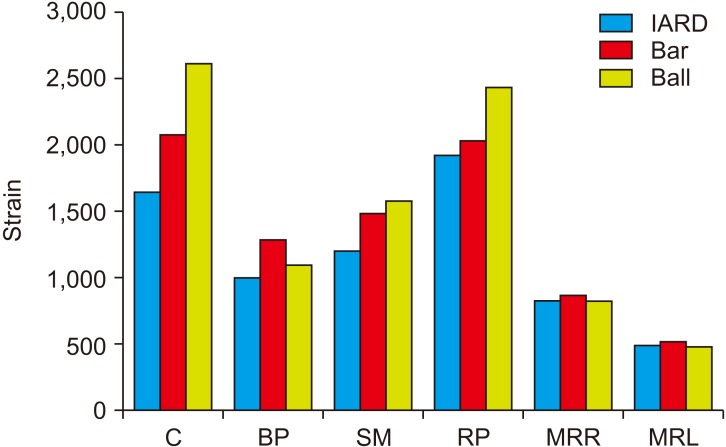
The lowest strain values were measured in the IARD, except for the MRL region for the ball attachment situation (586). The highest value was observed in the C region for the bar attachment situation (1,857.6).
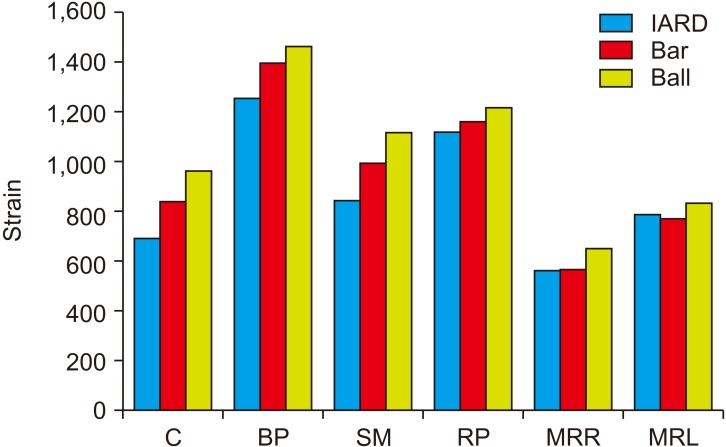
The lowest strain values were measured in the IARD. The highest value was observed in the C region for the ball attachment situation (1,192.05).
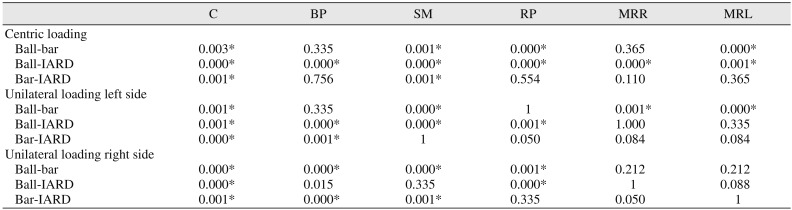
All P-values comparing attachment types are presented in Table 2.
IV. Discussion
The aim of this study was to explain the use of the presented new attachment system. If the results exhibited similar strain and/or stress distributions, the clinical treatment modalities for mandibular ISRDs could be modified to provide more economic, patient friendly, and safe solutions38. The null hypothesis of the study that IARD and ISRD would not differ on stress distribution in the edentulous mandible was rejected. The lower stress patterns observed in the IARDs show that this treatment option may be preferred for clinical use in some situations. Since information about functional loads on implants and the bone is essential to achieve long-term implant success, correct qualification and quantification of forces on implants are crucial10113940. Studies evaluating the IARD treatment option in two interforaminal implant situations are limited to a few case series34353637. The present study is the first report evaluating this type of IARDs.
Patients who can afford dental implants often have more esthetic demands and expectations of more rigid prosthetic solutions. Therefore, extracoronal precision attachments in IARDs were selected instead of conventional clasp-retained removable dentures in the present study. For biomechanical assessment of stress distribution in vitro, SG analysis is one of the most common methods used in dentistry38. The info gathered from SGs under differing experimental conditions should be regarded skeptically before clinical use because these measurements are limited to the bonded area of the gauge. The measured force levels in the present study are comparable to those measured in recent in vivo studies with SG abutments on implants4142.
When patients use ISRDs, loads are transferred to the alveolar bone surrounding the implants as well as to residual alveolar ridges and abutments. Therefore, ISRDs depend on both implant and mucosal support40. It is important not to create negative forces on implant abutments to avoid implant damage.
The thickness of the mucosa surrounding the alveolar ridge of the mandible was 2 mm in the present study, in agreement with previous studies3843. The effect of attachment type on stress distribution was studied in numerous investigations434445, and controversies could not be eliminated. The results of a recent systematic review showed no difference in marginal bone levels around implants supporting mandibular ISRDs when different attachment systems were used26. This suggests that, even if there are differences in the forces, they are not critical to bone loss.
The results of this in vitro study indicate that, compared to retentive anchors or bar attachments, the lowest strains occurred in the new tested denture system.
Strains in the posterior mandible, such as at the retromolar pad, buccal shelf, and mylohyoid ridge, were lower with the tested attachment system for ISRDs in the present study. This result is in agreement with another investigation that reported an inverse relationship between implant strain and bearing area loading value11. Our results showed that ISRDs had the lowest denture-bearing area loading, whereas single-attachment situations exhibited relatively low implant strain and high bearing area load. The results of the present study should only be considered for forces arising during vertical occlusal loading.
The anterior fixed bridge with the precision attachment partial denture eliminates two problems of conventional attachment systems tested in the present study. First, the stability of an overdenture is hard to achieve with single attachments especially in severely resorbed alveolar ridges11, and bar types of attachments generally require more space in the denture base and are more difficult to clean3. The proposed prosthetic solution eliminates the issues of stability and increased volume of the denture as a result of the bar system, especially in the anterior region. Second, the fixed part of the denture may increase the self-confidence of the patient. As shown in a recent study, wear of the matrices of single attachments are more noticeable when implants are divergently inserted4, requiring more maintenance over a shorter period of service. It was determined that the ideal solution in cases of divergent implants are splinted attachment types8. Therefore, the IARD solution is suitable for this kind of situation.
With the use of the described technique, it was not possible to quantify bone-implant interface strains, a limitation of the present study. Therefore, the results of the present study should be considered with caution. Although the in vivo situation was mimicked as ideally as possible, the results obtained from the in vitro experiments should be tested and confirmed in clinical follow-up studies before strict conclusions are drawn. However, the results encourage clinical use of the suggested fixed anterior bridge with precision attachments and RPD, since its esthetic and functional advantages are accompanied by favorable force distribution in the mandible. Use of IARDs is a good alternative to other attachment designs when 2 implants are inserted in the anterior region of the mandible.
V. Conclusion
Within the limitations of the present study, it can be concluded that an IARD may be a reasonable and valuable alternative to ball attachments or a bar in two interforaminal implants situations, especially when the patients prefer to have their teeth as fixed prosthesis even when they remove thir dentures. The in vitro results are qualitative in nature, and their clinical significance should be tested and confirmed in clinical studies.


 XML Download
XML Download