

 PDF
PDF ePub
ePub Citation
Citation Print
Print



I. Introduction
Intravascular papillary endothelial hyperplasia (IPEH) was first described in 1923 by Masson1 as hemangioendotheliome vegetant intravasculaire. It is a benign vascular lesion that predominantly occurs in the skin and subcutaneous tissue of the trunk, fingers, and head and neck regions. Oral IPEH lesions are uncommon and a review of oral lesions conducted in 2004 reported only 91 cases of the oral mucosa and lips2.
IPEH is an inflammatory vascular lesion with a trauma etiology and nonspecific clinical characteristics. Due to the complex presentation, it should be differentiated from other soft tissue tumors, especially angiosarcoma.
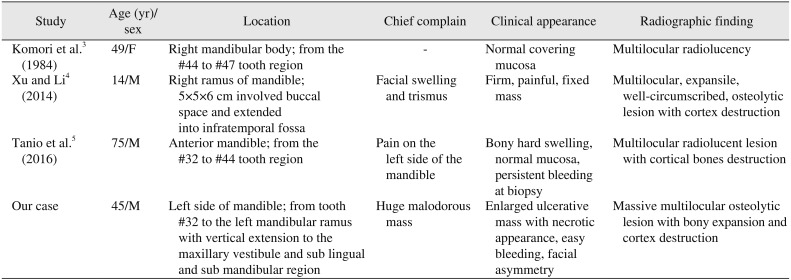
According to the literature, only three cases of IPEH in the maxillofacial skeletal tissues have been reported previously345.(Table 1) This article describes a case of pure IPEH involving half of the mandible. The lesion mimicked a malignant tumor and because of the uncommon location, huge size, and complicated histology, representing a considerable diagnostic challenge.
II. Case Report
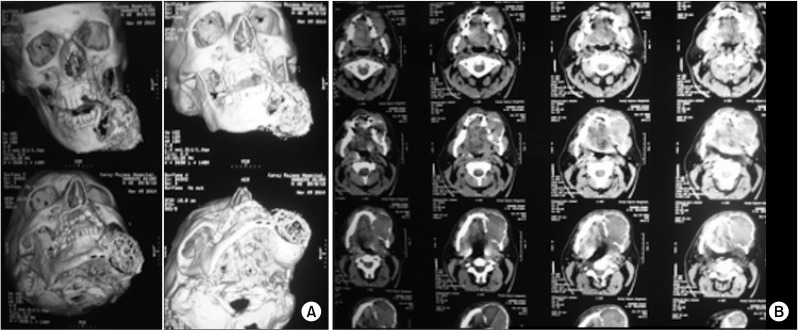
A 45-year-old male was referred to the Department of Oral and Maxillofacial Surgery of Taleghani Hospital (Shahid Beheshti University of Medical Sciences, Tehran, Iran) in 2011, with a chief complaint of a huge malodorous mass in the mouth. Five years ago, during dental visit, the patient first noticed a small prominent lesion on the left side of mandible. The patient did not seek treatment and the lesion gradually progressed to a large destructive mass. The mass grew suddenly and considerably in the past two months. Extraoral examination revealed obvious facial asymmetry due to bulging of the left side of face from the buccal to the submandibular region.(Fig. 1) The skin was intact without any sloughing or color change. The patient suffered from paresthesia of the left infraalveolar nerve and severe halitosis. Intraoral examination revealed a huge, expansile lesion from tooth #32 to the left mandibular ramus, which caused tooth displacement. Vertical extension to the maxillary vestibule and sublingual region was evident. The bulky lesion displaced the tongue and interfered with mouth movement. The lesion was covered by ulcerative and necrotic tissue.(Fig. 2) The patient reported easy bleeding of the lesion, which was spontaneous or caused by minor trauma. Due to its dark appearance, the first clinical diagnosis by the Department of Oral Medicine was melanoma. Panoramic radiography and computed tomography revealed an extended multilocular osteolytic lesion with bony expansion and cortical destruction. There was obvious tooth displacement and root resorption.(Fig. 3, 4)
Based on the clinical and radiographic examinations, the differential diagnosis focused on malignant bony tumors including intraosseous odontogenic carcinoma, clear cell odontogenic carcinoma, ameloblastic fibrosarcoma, and osteosarcoma.
Incisional biopsy was performed and histologic sections showed a necrotic lesion with mixed inflammatory cells and fungal hyphae, likely Mucorales.
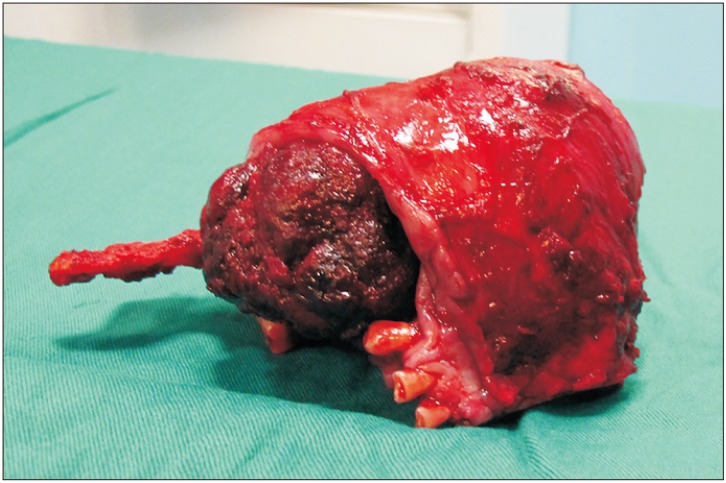
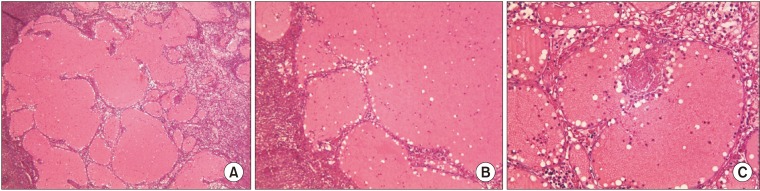
Because pathology confirmed a diagnosis of mucormycosis, the patient underwent left hemimandibulectomy with bone and soft tissue resection (Fig. 5) and reconstruction with a reconstruction plate and a pectoralis major myocutaneous pedicled flap. Definitive histopathologic examination of the resected specimen confirmed a vascular tumor characterized by numerous papillae formation in the vessels. The papillae were covered by one to two layers of endothelial cells and encompassed a hyalinized fibrous tissue core. The vascular lumen was dilated with thrombosis and many hemorrhages. (Fig. 6) Surgical margins showed inflamed granulation tissue with cholesterol clefts and reactive bone formation. The intraoral part of the tumor was covered by an ulcerated epithelium with a fibrinopurulent membrane in some areas. There was no evidence of malignancy. The lesion was finally diagnosed as pure-type IPEH. The postoperative course was uneventful and there was no recurrence during seven years of follow-up.
III. Discussion
IPEH is a rare vascular lesion of the skin and subcutaneous tissue and can be distinguished by multiple papillary processes and proliferation of endothelial cells6.
Masson first described this lesion as a form of endothelial cell neoplasm causing subsequent vascular obstruction and tissue necrosis7. Other investigators focused on the reactive process of the lesion following thrombus organization and endothelization8. Hyperemia or lymph stasis and local production of angiogenic growth factors are another suggested pathogenesis of this lesion. Expression of Ki-67 during active phases of the cell cycle suggest a neoplastic source of the lesion9, but due to granulation tissue formation, a reactive etiology of endothelial cell proliferation is the most likely pathogenesis of IPEH10. Most prior studies cited hormonal impacts and the female predilection of the lesion11. IPEH is more common in older patients and the most common regions are the head and neck (23%), lower extremities (17%), and fingers (16%)12. It rarely occurs in the oral cavity and most intraoral sites are the lower lip followed by the tongue, buccal mucosa, and upper lip13.
In 1983, Hashimoto et al.14 described three subtypes of IPEH: (1) pure, developing in the dilated vessels of the figure and head-neck region; (2) mixed, forming over a preexisting lesion like a hemangioma, artero-vascular malformation, pyogenic granulomatosis, aneurysm, or chronic disease with venous thrombosis; or (3) extravascular, originating from previous hematoma with a history of trauma.
Similar to the common occurrence of phleboliths in vascular lesions, numerous microcalcifications may be seen in IPEH that cause vascular occlusion and tissue necrosis. Because of the diverse presentations of this lesion, computed tomography with contrast media or magnetic resonance imaging reveals the vascularity and extent of lesion, but have limited usefulness in differential diagnosis15.
Clinical manifestations of the lesion are not specific and it is difficult to differentiate from other neoplasms or vascular lesions. Thus, according to location and size, IPEH may mimic different lesions such as mucoceles, hemangiomas, hematomas, intravenous pyogenic granulomas, phlebectasias, salivary gland tumors, nevi, Kaposi's sarcomas, or angiosarcomas.
Angiosarcoma is the most important malignant lesion to differentiate from IPEH. Areas of organized thrombus in the dilated vessels and proliferation of endothelial cells in papillary form toward the lumen are important for diagnosis of IPEH. The circumscribed and intravascular location of the lesion and presence of thrombotic material, along with absence of nuclear hyperchromia, cellular pleomorphism, atypical mitosis, foci of necrosis, and irregular capillary vessels are also major features differentiating IPEH from angiosarcoma16.
Complete excision with healthy margins is the accepted treatment plan. Cohen et al.17 used sclerotherapy with sodium tetradecyl sulfate prior to resection with the aim of minimizing bleeding and improving esthetic results in one case of mixed IPEH of lip. Other treatment methods like endoscopic surgery and use of beta-adrenergic antagonists were reported according to the site involved18. In the case of multiple intracranial lesions or anatomic limitations that could result in incomplete resection, adjuvant radiotherapy or chemotherapy have been associated with a good prognosis19.
Although recurrence of the IPEH is rare, incomplete resection or recurrence of the primary vascular lesion are possible causes. Furthermore, in the case of recurrent IPEH, thorough investigation to rule out angiosarcoma is needed.
The case reported here is notable because of some particularities: First it is the fourth reported case of IPEH in the mandible. Since the first mandibular lesion was reported in 19843, Xu and Li4 reported one case of IPEH at the mandibular ramus with expansile and osteolytic characteristics in 2014. The lesion appeared with swelling and trismus and was initially thought to be a case of fibrous dysplasia, ameloblastoma, and giant cell tumor. In 2016, Tanio et al.5 reported a mixed IPEH associated with hemangioma of the anterior segment of the mandible, in which embolization of the inferior alveolar artery was performed followed by successful removal. None of the reported lesions were as large or as long-term as this case, with significant intraoral and extraoral extension. The large size of this lesion and subsequent local circulation disorder resulted in tissue necrosis and fungal infection, leading to the diagnostic challenge and variation in pathologic results encountered in this case.
According to the literature, not only are mandibular IPEH lesions rare, but the occurrence of IPEH in skeletal tissue is also uncommon13. Jain et al.20 reported one case of IPEH in the hard palate masquerading as adenoid cystic carcinoma.
Resection of multiple recurrent IPEHs affecting the skin and tibia in a 75-year-old male over the course of three years was reported by Higashi et al.21 in 2009. The patient had hepatitis C, hepatoma, and associated coagulopathy and it was suggested that liver dysfunction and induced microthrombus formation were the probable etiology.
The spine, skull, and skull base are other skeletal sites involved in IPEH that have been reported in the literature22232425.
In conclusion, IPEH as an inflammatory vascular soft tissue lesion may occur in hard tissue of the head and neck region, without a history of trauma. Tissue necrosis and mixed infection are the result of circulation disruption. Differentiating this lesion from malignant vascular tumors like angiosarcoma is an important and challenging task for oral and maxillofacial pathologists and surgeons.



 XML Download
XML Download