

 PDF
PDF ePub
ePub Citation
Citation Print
Print



I. Introduction
Limited mouth opening may be caused by various diseases, such as temporomandibular disorders, fracture of the condylar process, neurological disorders, rheumatoid arthritis, inflammatory disease, tumors and hyperplasia of the coronoid process12. Masticatory muscle tendon-aponeurosis hyperplasia (MMTAH) is a new clinical condition associated with limited mouth opening.
In 2000, Inoue et al.3 reported a patient with hyperplasia of only the masseter muscle aponeurosis, accompanied by limited mouth opening and a square mandible. Moreover, Murakami et al.4 reported 10 chronic severe mandibular hypomobility patients exhibiting square mandible with hyperplasia of the mandibular angle. Beckers5 reported a patient with bilateral masseter muscle hypertrophy accompanied by limited mouth opening in 1977 from Switzerland. Her mandible appeared square and bilateral resection of the masseter muscles did not improve limited mouth opening. Thus, cases of limited mouth opening accompanied by a characteristic square mandible have been reported.
In 2005, MMTAH was recognized as a new disease at the conference of the Japanese Society for Oral and Maxillofacial Surgeons. Subsequently, the disease was defined and approved at the conference for the Japanese Society of Temporomandibular Joint in 20086. In 2009, the disease name of MMTAH was first published in an international journal by Yoda et al.7. Thereafter, MMTAH came to be very well known disease. In 2014, a case of MMTAH was reported from Switzerland by Worni et al.8. In 2015, Lehman et al.9 reported four female patients who presented limited mouth opening. Although they were not diagnosed with MMTAH, we consider that these must have been cases of MMTAH10. Furthermore, anesthesiologists reported cases of MMTAH that resulted in difficult laryngoscopy after the initiation of anesthesia11.
II. Clinical Features
The main symptom of MMTAH is limited mouth opening. Because the condition progresses very slowly from adolescence, patients have few subjective symptoms and limited mouth opening may only be identified by dentists during visits to dental clinics. In the 142 patients reported at the conference for the Japanese Society of Temporomandibular Joint, the maximum opening at the first medical examination was 5 to 43 mm (mean, 23.5 mm)11. Patients usually have no pain in the region of the temporomandibular joint or muscles, and the lateral and anterior movements of the mandible are not limited.
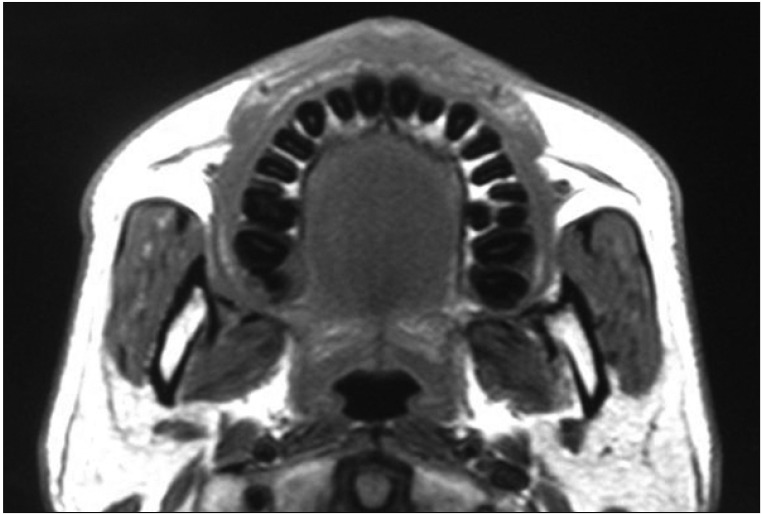
A characteristic feature of this disease is a square mandible with a small gonial angle and flattening of the occlusal planes1213.(Fig. 1, 2) The square mandible, which exhibits a prominent mandibular angle, may be due to hyperplasia of the aponeurosis and tendon. Both coronoid processes are thickened anteroposteriorly, but there is no contact between the coronoid process and the zygomatic arch on mouth opening.
Magnetic resonance imaging (MRI) shows a hyperplastic aponeurosis and masseter muscle. In horizontal MRI sections, the bilateral overhang of the masseter muscle along the anterior border of the mandibular ramus is noted, and low intensity areas showing the aponeurosis are detected on the lateral aspect and inside the masseter muscle14. Minowa et al.15 reported that aponeuroses are rarely found below the lower half of the anterior margin of the masseter muscles. However, thickened aponeuroses are often observed to extend into this lower half in patients with MMTAH. On maximum mouth opening, intraoral palpation along the anterior border of the masseter muscle reveals a hard cord-like structure resulting from hyperplasia of the aponeuroses, which is consistent with the MRI findings.(Fig. 3)
III. Diagnosis
The diagnostic criteria for MMTAH are as follows: (1) limited mouth opening that progresses very slowly from adolescence and no limitation of lateral or anterior mandibular movement; (2) intraoral palpation reveals a hard cord-like structure along the overhang of the anterior border of the masseter muscle on maximum mouth opening (Fig. 4); and (3) a square mandible7.
Although MRI can help visualize tendons and aponeuroses, the criteria for diagnosing hyperplasia in these tissues have not yet been established.
IV. Pathophysiology
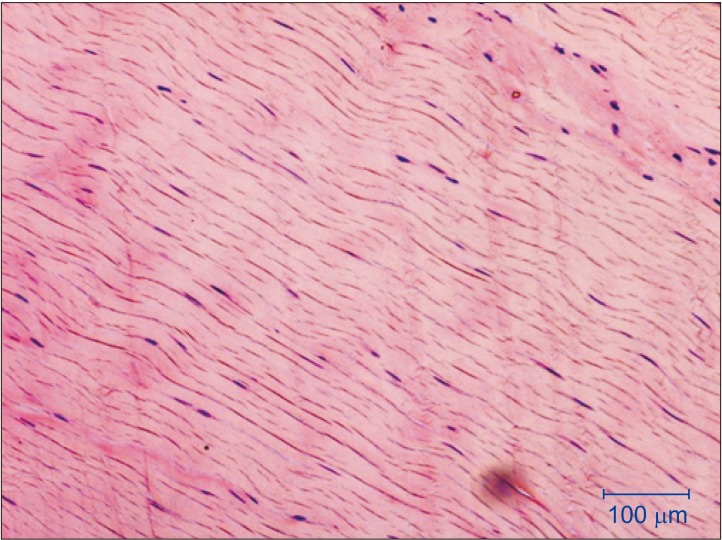
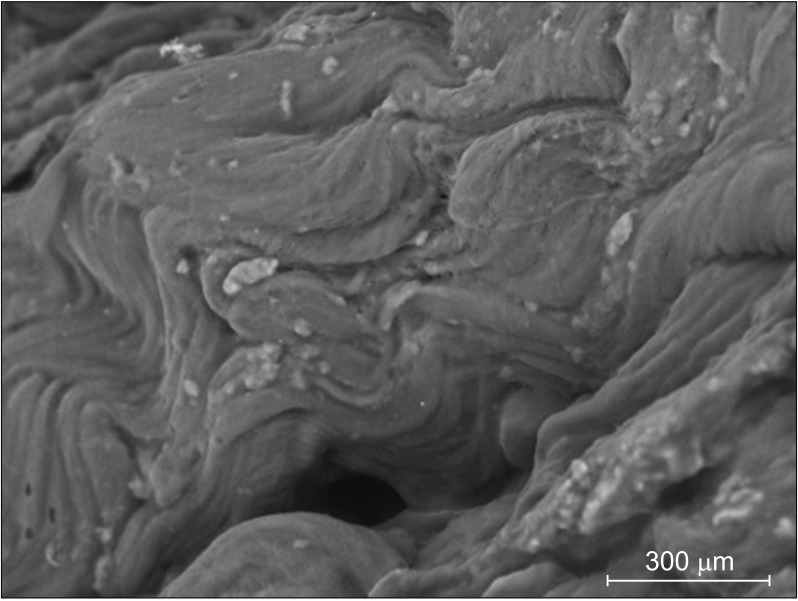
Tendon and aponeuroses tissues in MMTAH show normal structures on macroscopic examination17.(Fig. 5) This finding suggests that tendon tissues in MMTAH undergo hyperplasia. However, the aberrant sound heard on cutting tendon tissues with scissors indicates hardness of the tendon tissues, suggesting occurrence of anomalous changes7. Electron microscopy reveals mineralized nodules in the tendon tissues of MMTAH patients, in comparison to tendon tissues of individuals without facial deformity (FD)18.(Fig. 6) On energy dispersive X-ray analysis, silicon, calcium, and phosphorous are observed in the tendons of MMTAH patients18.
Moreover, according to a proteomic analysis of the temporalis muscle tendon of MMTAH patients and in comparison to FD, fibrinogen fragment D and β-crystallinA4 (CRYBA4) were upregulated, while myosin light chain 4 (MYL4) was downregulated in MMTAH patients1920. Inactivation of myosin II causes abnormalities in the collagen fibers of the tendon along with downregulation of MYL4, suggesting that MYL4 reduction is associated with pathological conditions in MMTAH. CRYBA4, which plays a vital role in protecting cells in non-lens tissues from damage caused by environmental and/or metabolic stress, is upregulated in the tendons of MMTAH patients, thus indicating that it may have a role in the stress response or pathology associated with the development of MMTAH.
V. Etiology
The etiology of MMTAH remains unclear. MMTAH is more common in women and parafunctional habits such as a clenching or grinding are often associated with the condition. It is therefore suggested to be an acquired disease due to work hypertrophy3. We examined the effect of estrogen on the tenocyte function and the relationship between mechanical stress and crystallin beta A4 (Cryba4), using murine TT-D6 tenocytes. A physiological dose of estrogen increased the levels of scleraxis and tenomodulin (markers of tendon development) in TT-D6 tenocytes. A mechanical loading assay using tensile force revealed that tensile force increases the Cryba4 levels in tenocytes21. This suggests that mechanical stress may affect tendon differentiation.
However, all cases of MMTAH progress very slowly from adolescence and show bilateral involvement. These clinical futures suggest the possibility of congenital disease. Thus, we hypothesize that this disease has both environmental and genetic factors, as a multifactorial genedisease22.
VI. Treatment
Conservative treatments such as mouth opening training, pharmacotherapy, occlusal splint have shown no significant Conservative treatments such as mouth opening training, pharmacotherapy, occlusal splint have shown no significant effects in patients with MMTAH. The standard therapy is surgical treatment, including anterior partial aponeurectomy of the masseter muscle, and coronoidectomy7. Coronoidectomy should be performed to remove the tendon arising from the posterior and superior aspects of the coronoid process. Although mandibular anglectomy is also reported2324, we think that it is unnecessary for the improvement of the limited mouth opening. However, mandibular anglectomy can still be performed for aesthetic reasons.
We previously reported a case presentation with videos25, in which we introduced the surgical procedures for MMTAH patients in detail. Surgical treatment is performed under general anesthesia. Muscular relaxation does not improve the restricted mouth opening.
An incision is made in the oral mucosa, the same as in sagittal split ramus osteotomy, and the anterior margin of the mandibular ramus is exposed. The masseter muscle will then be visible on the outer aspect of the mandibular ramus. The aponeurosis is revealed and exhibits a silvery-white color on the exfoliating upward and outward of the masseter muscle.(Fig. 7) The aponeurosis are detached from the muscle tissue and excised as large as possible using scissors or electrosurgical knives. Aponeurectomy of the masseter muscle should be performed bilaterally.
The temporal tendon attached to the coronoid process is then exposed. An abnormal sound can be heard on exfoliating this periosteum with a raspatory. Then the anterior, lateral and medial tendons are removed from the coronoid process. (Fig. 8) Although the posterior tendon should be cut as much as possible, it is often difficult to excise it completely. By clasping the coronoid process tightly with the help of a Pean or Kocher forceps, the coronoid process is excised using cutting instruments, such as a Lindemann drill or an ultrasonic surgical instrument. Coronoidectomy should be performed bilaterally. After confirming that the mouth has opened more than 45 mm, the surgical incision can be closed using sutures. Continuous intraoral drainage is effective for reducing postoperative swelling and conducting mouth opening training.
Immediate oral intake and training in intentional clenching are required postoperatively to prevent open bite. Mouth opening training should be started 5 days after surgical treatment. Postoperative mouth opening training is an important prognostic factor. The training involves widely opening the mouth for 30 seconds with the help of a mouth opener. This is repeated more than 3 times, using analgesics to control the pain. The patient is discharged once they can open their mouth more than 40 mm without using the mouth opener. This training should be continued for at least 6 months.
VII. Long-term Results
In previous reports, patients who underwent surgical treatment showed good long-term results7. MRI after 1 year reveals that the temporal muscle is reattached to the resected stump of the bone, and a reduction in the cross-sectional area of the masseter muscle26.
We compared the outcomes of patients who underwent surgery (19 patients) and those who did not (9 patients)27. The mean increase in mouth opening after 2 years was 20.2 mm in the surgical group and 2.4 mm in the non-surgical group. Adequate mouth opening training for 6 months after surgery was a key factor for obtaining good outcomes. Thus, the general condition and personality of individual patients should be evaluated carefully before surgery to predict whether or not they will be able to endure the pain associated with postoperative mouth opening training.
VIII. Conclusion
MMTAH is still new and is hardly recognized in Korea. However, there are definitely MMTAH patients in Korea. This author hypothesizes that it is probably misdiagnosed as a refractory temporomandibular disorder. Surgery is useful for the management of MMTAH. It is my hope that the wide recognition of MMTAH will contribute to the health of patients.





 XML Download
XML Download