

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
A usual source of care (USC) refers to a medical institution or physician that one mainly visits when sick or for seeking medical advice.1 A USC plays an important role in primary care because it becomes a gatekeeper to a higher medical institution or specialist.23 According to previous studies, a USC can induce appropriate use of medical services and contribute to the improvement of health behaviors,456 reduce unmet medical needs, and improve access to primary care.789
Studies on the association between having a USC and medical expenses or medical utilization have been actively conducted. Many studies demonstrated that a USC reduced medical expenses,41011121314151617 but there were also conflicting results that it increased18192021 or had no significant effect on medical expenses.222324
One of the explanations for the results indicating that having a USC increased medical expenses is the endogeneity of having a USC. In other words, people who have frequent visits to doctors are more likely to have a USC due to the effects of latent factors, especially including health conditions or medical demands. In such cases, having a USC can result in the increase in medical care utilization.62526 This is an important issue in studies on having a USC and medical care utilization, and endogeneity could have more affect especially in countries where a USC has not been systemized; however, there have been few studies that controlled for this.
This study tried to overcome limitations of endogeneity by including only those who had medical demands and controlling latent factors. In addition, a panel analysis was used and medical expenses were classified further into types of use (outpatient and inpatient departments) and categories of medical institutions, and the total medical expenses were analyzed. In Korea, Ministry of Health and Welfare announced a rule on the standard services of the health care organizations by type for efficient utilization of medical resources: clinics for ambulatory patients, hospitals for inpatients and tertiary hospitals for severe patients. In reality, however, this distinction has been lost. All medical institutions try to see more patients even in the realm of ambulatory care services for managerial purposes. In this situation, medical expenses were analyzed by category to determine how having a USC affects the proper role of each medical institution.
Korea has adopted a fee-for-service payment system. In addition, the patient referral system has not been well-established.2728 In particular, there is no legal or institutional obligation to have a USC, which causes problems such as segmented medical care, duplication of examination, and increased medical expenses while freely using various medical institutions. Therefore, there is a growing interest in a USC structure with policies on topics such as promoting continuous care for patients with hypertension or diabetes mellitus in a single medical institution, and the need for relevant study is also increasing.
The purpose of this study was to empirically analyze the causal relationship between having a USC and medical expenses using panel data which represents the entire Korean population. This can be used as source data for health care policies that can induce appropriate medical expenses and desirable medical care utilization.
METHODS
Study subjects and data
This study used Korea Health Panel Data of 2012, 2013, and 2016 (3 years) including questions about having a USC, from among data after 2010 when the method of calculation of medical expenses was fixed. The Korea Health Panel Data are from a nationally representative survey conducted by the Korea Institute for Health and Social Affairs and the National Health Insurance Service.29 Sample households are recruited using a stratified 2-stage cluster sampling method with probabilities proportion, and the survey is conducted by computer aided personal interview method for 6,000–7,000 households annually. 30 The study subjects included individuals aged 20 years and older among those who responded to the questionnaire about having a USC. Those who responded with “I do not get sick easily” or “I rarely visit medical institutions” as the reason for having no USC were excluded to analyze only those who had medical demands. The number of final analysis subjects was 6,120 in 2012, 6,593 in 2013, and 7,598 in 2016 (Fig. 1).

Variables
The variables used in this study are shown in Table 1. An explanatory variable was having a USC. To the question about having a USC (“Do you have any medical institution where you regularly visit, when you get sick or when you would like to have tests or therapeutic consultation?”), if one responded with “Yes,” it was defined as having a USC, and if one responded with “No,” it was defined as not having a USC.
Table 1
Description of variables

![]()
An outcome variable was medical expenses, and it was classified as total medical expenses, outpatient expenses, inpatient expenses, clinic expenses, and hospital expenses. All medical expenses were calculated by adding the copayment amount, payment covered by National Health Insurance Corporation, and non-covered items.
Other control variables comprised the predisposing factors, enabling factors, and need factors with reference to the Andersen Model.31 The predisposing factors included gender, age, educational level, and place of residence, the enabling factors included income level, and the need factors included subjective health status and Charlson comorbidity index (CCI). Age was categorized by age at 10-year intervals; regarding regions, Seoul and Gyeonggi regions were classified as the Capital, the five metropolitan cities as Metropolitan, and the rest as other areas. Educational level was categorized into three parts: below elementary school, below high school, and above. Income levels were categorized into three parts based on deciles distribution: deciles 1, 2, 3, and 4 were low-income level; deciles 5, 6, and 7 were medium-income level; and deciles 8, 9, and 10 were high-income level. The income level is a gross household income and calculated by dividing the gross income per household by the square root of the number of household members. The subjective health status was categorized using answers to the question “What do you think of your current health status?” The answer of “very good” or “good” was categorized into the good health group, that of “moderate” was categorized into the moderate health group, and that of “poor or “very poor” was categorized into the poor health group. As CCI is an index designed to predict mortality, it is often used as a tool to reflect comorbidity and the severity of disease.3233 CCI was calculated based on the major diagnostic and sub-diagnostic codes of medical history of the Korea Health Panel Data and used as a continuous variable without categorization. Disease codes used in the CCI calculation are shown in Supplementary Table 1. The presence of chronic diseases was identified if any of the seven major chronic diseases (high blood pressure, diabetes, hyperlipidemia, tuberculosis joint disease, ischemic heart disease, and cerebrovascular disease) were present
Statistical analysis
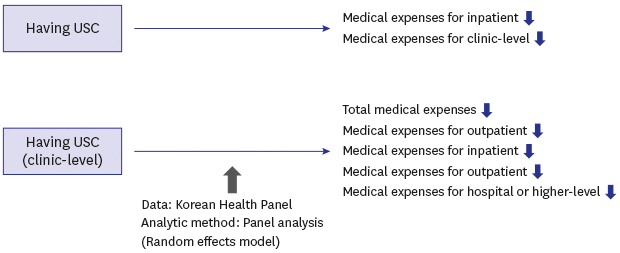
The sociodemographic characteristics in accordance with whether the subjects have a USC are shown as a percentage by year. The panel analysis on the effect of having a USC on each of total medical expenses, outpatient expenses, inpatient expenses, clinic expenses, and hospital expenses was performed using the random effects model. In addition, the panel analysis on the effect of having a clinic-level and hospital-level USC among the group having a USC, on each of the total medical expenses, outpatient expenses, inpatient expenses, clinic expenses, and hospital expenses, compared to that in the group without a USC, was conducted using the random effects model.
The model used in the analysis is shown in Equation 1 below. The model was based on Anderson Model and previous studies.3435 Medical expenses, the outcome variable, were logarithmically transformed. For statistical analysis, SAS9.4 (SAS Institute Inc., Cary, NC, USA) and STATA13 (StataCorp LP., College Station, TX, USA) were used.
Yti: t: time, i: medical expenses of patients (total, outpatient, inpatient, clinic-level, hospital or higher-level)
Dti: t: time, i: 1 for patients with a USC (total, clinic-level, hospital-level), 0 for patients without a USC (total, clinic-level, hospital-level)
Xti: t: time i: explanatory variables of patients (predisposing, enabling, and need factors)
μi: i: patients' unique effect
εti: error term
Ethics statement
The study was approved by the Institutional Review Board of Jaseng Hospital of Korean Medicine in Seoul, Korea (JASENG 2019-01-002). Informed consent was waived because KHP data, which this study used, were provided without personal information by a consortium of the Korea Institute for Health and Social Affairs and the National Health Insurance Service.
RESULTS
Sociodemographic characteristics of subjects according to having a USC
Sociodemographic characteristics of subjects according to having a USC by year are shown in Table 2. Regarding gender, the proportion of women in the no USC group was higher than that of the USC group, while the proportion of men in the USC group was higher than that of the no USC group. Regarding age, the proportion of individuals in the 20–59 years group in the no USC group was higher, while the proportion of individuals of older age were higher in the USC group. As age increased, the probability of having a USC also increased. Additionally, there were more individuals with good subjective health status in the USC group than the no USC group. The proportion of individuals with chronic disease was higher in the USC group. The mean CCI was higher in the USC group than in the no USC group.
Table 2
Status of having a USC by year

| Variables | 2012 | 2013 | 2016 | |||
|---|---|---|---|---|---|---|
| No. | % | No. | % | No. | % | |
| Total | 2,909 | 4,109 | 4,892 | |||
| Clinic-level | 1,804 | 62.3 | 2,702 | 65.9 | 3,392 | 69.4 |
| Hospital-level | 1,063 | 36.7 | 1,361 | 33.2 | 1,460 | 30.0 |
![]()
Status of USC type (clinic-level, hospital-level) by year are shown in Table 3. Proportion of clinic-level USC among total USC was 62.3% in 2012, 65.9% in 2013 and 69.4% in 2016. Changes of status of having a USC were also shown in Supplementary Table 2. The most common situation was having a USC for three years (26.5%). There were not many cases where USC status changed every year (15.7%).
Table 3
Sociodemographic characteristics of subjects according to having a USC
Data are presented as %.
USC = usual source of care, CCI = Charlson comorbidity index.
aUSC: group with a USC; bno USC: group without a USC.
![]()
Effect of having a USC on medical expenses
The effect of having a USC on medical expenses is shown in (Table 4). The USC group spent 20% less on inpatient expenses and 25% less on clinic expenses compared to the no USC group. Total medical expenses, outpatient expenses, and hospital expenses were also lower, but were not statistically significant.
Table 4
Effect of having a usual source of care on medical expenses (multiple panel regression with random-effect model)a

USC = usual source of care, CI = confidence interval.
aAdjusted for gender, age, region, educational level, income level, subjective health status, chronic disease, Charlson Comorbidity Index; bDifference: = eβ − 1.
![]()
Effect of having a clinic-level USC on medical expenses
Effect of having a clinic-level USC on medical expenses is shown in Table 5. Having a clinic-level USC decreased total medical expenses by 12%, outpatient expenses by 9%, inpatient expenses by 35%, and hospital expenses by 74%, but increased clinic expenses by 29%. Meanwhile, having a hospital-level USC decreased clinic expenses and increased hospital expenses.
Table 5
Effect of having a clinic-level and hospital-level usual source of care on medical expenses (multiple panel regression with random-effect model)a

USC = usual source of care, CI = confidence interval.
aAdjusted for gender, age, region, educational level, income level, subjective health status, chronic disease, Charlson Comorbidity Index; bDifference: = eβ − 1.
![]()
DISCUSSION
The findings of this study suggest that inpatient and clinic expenses were lower in the group with a USC than in the group without a USC. Total, outpatient, inpatient and hospital expenses were lower in the group with a clinic-level USC than in the group without a USC. Many previous studies have shown that having a USC reduced medical expenses, such as admission rates and medical expenditures,10 drug spending,12 and outpatient spending.36 On the other hand, there have been studies that suggest that having a USC may increase medical expenses, especially in Korea.18192021
The results that having a USC increases medical expenses can generally be interpreted as follows. First, having a USC improved access to medical care and reduced unmet medical needs. Second, having a USC encouraged medical consultation and led to the utilization of excessive medical care and medical resources. However, considering that all Korean citizens were covered by national health insurance,37 and annual average physician visit per capita was the highest among OECD countries,38 the first interpretation is less convincing. The second interpretation is also inappropriate because it is incompatible with many previous studies.410111213141516
One of the explanations for the high medical expense of the group having a USC was the endogeneity of having a USC. In other words, if unobserved preferences such as medical demand and health status increase not only the use of medical care but also the probability of having a USC, it could seem that having a USC increases medical expenses.62526 In particular, such endogeneity was more likely to occur in a country like Korea where having a USC was not institutionalized. In order to solve this problem, this study excluded those who reported having no USC because of absence of medical demand. Unlike the results of many previous studies conducted in Korea,18192021 the results showed that having a USC significantly decreased inpatient expenses and clinic expenses. It also decreased total medical expenses, outpatient expenses, and hospital expenses; however, they were not statistically significant.
In Korea, having a USC was not institutionalized, and there were many cases where hospital-level institutions were used as a USC.27 Therefore, the concept of having a USC as surveyed by the Korea Health Panel was restricted to “major visiting medical institution” and did not have the characteristics of primary care. Therefore, this study further analyzed the effect of clinic-level USC on medical expenses to assess the effect of a USC with attributes of primary care such as comprehensiveness, initial contact, etc. As a result, having a clinic-level USC significantly decreased total medical expenses, outpatient expenses, inpatient expenses, and hospital expenses. The effect of clinic-level USC on reducing medical expenses was higher than that of total USC levels; in particular, the effect of reducing hospital expenses was high. This result supports the findings of a previous study that the clinic-level USC reduced the medical expenses of large hospitals.2427 Additional studies such as quality research on what the public thinks about the concept of USC are needed to clarify conceptualization.
In this study, the random effects model of panel analysis was used. The choice between fixed effects model and random effects model for panel analysis is still a controversy. The Hausman test is a commonly known statistical method for selecting a fixed effects model or random effects model. In this study, the Hausman test recommended using the fixed effects model by rejecting the null hypothesis. However, Clark and Linzer39 asserted that the Hausman test results cannot be a golden rule in selecting a model because the correlation between the characteristics of the individual and the explanatory variables is very rarely 0 in the actual data. They opined that the random effects model is appropriate if changes within an analysis of interested variables are significantly small or the number of individuals is much larger than the number of repeated measures. The number of individuals included in this study was about 6,000 to 8,000 per year, but the number of repeated measures was only three, and having a USC was the variable which was bivariate and showed minor changes for the individual (Supplementary Table 2). Therefore, this study analyzed the data by using a random effects model rather than a fixed effect model, although the Hausman test suggested a fixed effect model. Most of the results using the fixed model were not statistically significant. It is expected that analysis using a fixed model will be more viable when more data are released in the future (Supplementary Table 3).
Inadequate adjustment for health status and disease severity is a limitation of this study. The health status of individuals who had a USC or who did not have a USC, and individuals with hospital-level USC or with clinic-level USC among those who had a USC varied. To overcome the problem, analysis subjects were limited to those with medical demand, and CCI and subjective health status were included as explanatory variables. However, the study results might have remained confounding because the study was not a randomized experimental study.
Medical expenses can be divided into direct costs and indirect medical expenses, such as traveling costs or time required. This study analyzed only direct medical expenses, without considering indirect medical expenses. Additional studies are required in this regard.
The healthcare delivery system and primary care infrastructure in Korea has not been established well.2834 The annual increase in medical expenses and doctors consultations per capita have been at the top among OECD countries for several years now, leading to high medical expenses.3840 In the Korean context, this study suggests that a policy should be developed to encourage individuals to have a USC, especially a clinic-level USC, to help reduce medical expenses and promote desirable medical care utilization. Furthermore, the findings of this study are expected to have important implications for other countries with similar healthcare systems to that of Korea, such as a fee-for-service payment system. If the effect of having a USC is further analyzed by disease group, it will help design specific policies for those groups. In conclusion, having a clinic-level USC reduced total medical expenses, outpatient expenses, inpatient expenses, and hospital expenses. A policy on having a clinic-level USC is suggested to reduce current medical expenses and encourage desirable medical care utilization.
 XML Download
XML Download