

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The prevalence of type 2 diabetes mellitus (T2DM) is increasing worldwide. The prevalence of diabetes in Korea increased from 8.6% in 2001 to 13.7% in 2016.1 Chronic complications from diabetes, such as retinopathy, nephropathy, neuropathy, and cardiovascular, cerebrovascular, and peripheral arterial diseases, can increase morbidity and mortality.2 T2DM is also associated with an increased risk of bone fractures,345 because complications associated with diabetes such as hypoglycemia, peripheral neuropathy, orthostatic hypotension, vision impairment, and cardiovascular diseases can increase fall risk.678 Additionally, advanced glycation end products, which are associated with diabetic complications, can increase the stiffness of the collagen network9 and attenuate osteoblast differentiation.10
Therefore, several studies have investigated the effects of anti-diabetic drugs on musculoskeletal health. Thiazolidinediones (TZD) activate peroxisome proliferator-activated receptor gamma, stimulating adipocyte differentiation and inhibiting osteoblastogenesis.11 TZD use is therefore associated with reduced bone mineral density (BMD) and increased fracture risk. Although some studies have reported that sulfonylureas have neutral effects on bone metabolism, sulfonylureas may have positive anabolic effects on fractures by increasing endogenous insulin secretion.12 Metformin has been associated with fracture risk reduction by inhibiting osteoclast differentiation through the reduction of activator of nuclear factor kappa B ligand expression.13
Dipeptidyl peptidase-4 inhibitors (DPP-4i) inhibit the action of DPP-4, which degrades incretins, and increase the plasma levels of glucagon-like peptide-1 (GLP-1), GLP-2, and glucose-dependent insulinotropic polypeptide (GIP).14 Increased incretin levels are thought to affect bone metabolism; therefore, several studies have investigated the effects of DPP-4i on fracture risk, but the results in humans are controversial. A meta-analysis of 28 randomized controlled trials found that DPP-4i reduces the risk of fractures in T2DM patients.15 However, other studies have found that DPP-4i had no significant effect on the risk of fractures.51617
Thus, in this study, we analyzed the effects of DPP-4i on fractures in a Korean population with T2DM using data from a population-based cohort. The incidences of osteoporosis and fractures in DPP-4i users were compared with those in DPP-4i non-users and controls.
Go to : 
METHODS
Study subjects
Participants were extracted from the National Health Insurance Service–National Sample Cohort 2.0 (NHIS-NSC2.0), a population-based cohort established by the NHIS in Korea. NHIS provides benefits for diagnostics, injury treatments, rehabilitation, disease prevention, births, etc., and maintains national records on healthcare services and prescriptions (such as data on participants' insurance eligibility, medical care providers, heath examinations, and medical treatment).18 NHIS-NSC2.0 was defined to improve the first cohort version (NHIS-NSC) by reinforcing the accuracy of claims data and improving information protection. A sample (n = 1,108,369; within 2% of the national population) was extracted from people who maintained their national health insurance or medical care status in 2006. For these subjects, information was collected retrospectively from 2002 to 2005 and prospectively from 2006 to 2015. The data collected included sociodemographic information, diagnostic data, healthcare services provided, and healthcare service providers.
The subjects were divided into two groups based on their diabetes diagnosis from 2009 to 2014 (Fig. 1). Subjects older than 50 years of age without a history of diabetes between 2007 and 2009 were included in the analysis. Subjects without diabetes between 2009 and 2014 were used as the control group. The index date for the control group was defined as the first year in the database. For the subjects who were diagnosed with diabetes between 2009 and 2014, the index date was defined as the date of diagnosis during 2009–2014. The follow-up period for the two groups differed because not all subjects had information from as early as 2009, and this enabled us to recruit more subjects in our analysis. Subjects with a history of cancer between 2007 and 2015 were excluded. Subjects who died within 6 months of the index date, or with less than 180 days of data, were also excluded. Subjects with diseases related to secondary osteoporosis (hyperparathyroidism, Cushing's syndrome, vitamin D deficiency, multiple myeloma, leukemia, lymphoma, and rheumatic arthritis) were excluded. Subjects diagnosed with diabetes were classified as either DPP-4i users or DPP-4i non-users.
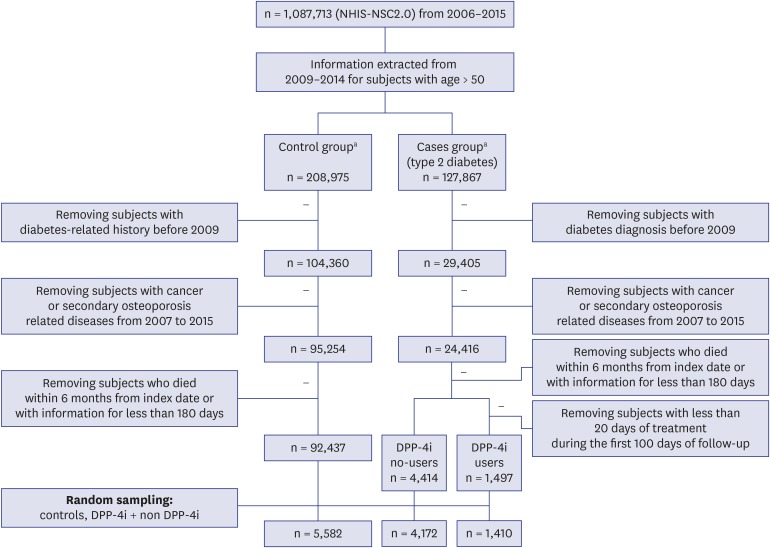 | Fig. 1Study progression.NHIS-NSC2.0 = National Health Insurance Service–National Sample Cohort 2.0, DPP-4i = dipeptidyl peptidase-4 inhibitors.
aControl group: subjects without diabetes between 2007–2014; case groups: subjects without a diabetes diagnosis from 2007 to the index date (index date: first year of diabetes diagnosis; ≥ 2009).
|
Data and measurements
Subjects and their diagnoses were classified using International Classification of Diseases (ICD)-10 codes. A diabetes diagnosis was indicated by the ICD-10 codes E11.X, E12.X, E13.X, or E14.X. Drug use was defined as the use of a drug prescribed for more than 20 days during the period from the index date up to 100 days. This strategy guaranteed that the subjects took the treatment starting from the index date.
The primary endpoint was the incidence of a composite outcome consisting of osteoporosis diagnosis, osteoporotic fractures, vertebral fractures, non-vertebral fractures, and femoral fractures. The secondary endpoints were the incidences of osteoporosis diagnosis, osteoporotic fractures, vertebral fractures, non-vertebral fractures, and femoral fractures individually. Osteoporosis diagnosis, osteoporotic fractures, vertebral fractures, non-vertebral fractures, and femoral fractures were defined using ICD-10 codes and fracture-related procedure codes (Table 1). To confirm the first diagnosis of osteoporosis or fractures, we checked that the ICD-10 code for that diagnosis had not been assigned before 6 months prior to the index date.
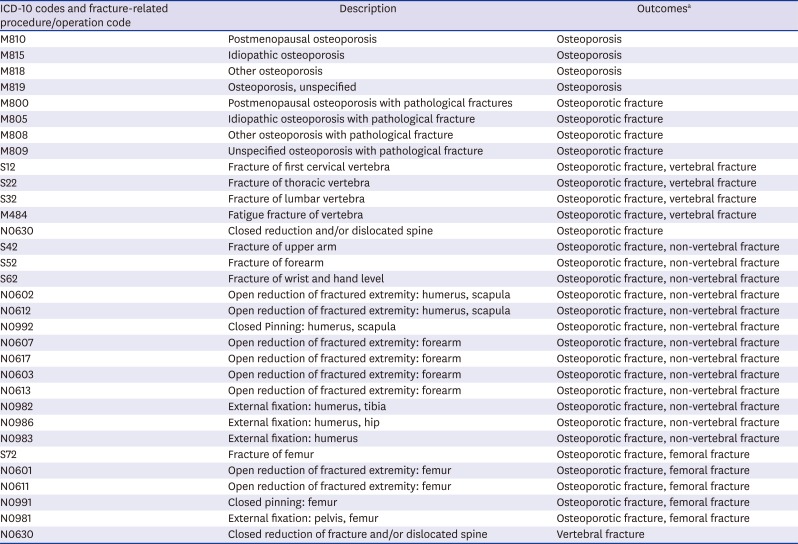
Table 1
ICD-10 codes for bone fractures/osteoporosis and fracture-related procedure codes
ICD = International Classification of Diseases.
aOutcomes: osteoporosis, osteoporotic fracture, vertebral fracture, non-vertebral fracture, femoral fracture.
![]()
The variables extracted for each subject included demographic information (age, gender), diabetes complications severity index (DCSI), Charlson comorbidity index (CCI), the use of anti-diabetic drugs (metformin, sulfonylurea, meglitinide, TZD, α-glucosidase inhibitor, sodium glucose cotransporter 2 inhibitor [SGLT2 inhibitor], GLP-1 agonist, and insulin), the use of hypertension medications (angiotensin II receptor blockers [ARB], angiotensin-converting enzyme [ACE] inhibitors, calcium channel blockers [CCBs], diuretics, and beta blockers), and dyslipidemia treatments (such as statin and fibrate). The DCSI allowed measurement of the severity of the diabetes-related complications based on seven categories: cardiovascular disease, nephropathy, retinopathy, peripheral vascular disease, stroke, neuropathy, and metabolic complications.19 The CCI was used to measure the level of comorbidity. The CCI included age, myocardial infarction, congestive heart failure, peripheral vascular disease, cerebrovascular accident, transient ischemic attack, dementia, chronic obstructive pulmonary disease, connective tissue disease, peptic ulcer disease, liver disease, diabetes, and hemiplegia.20 Data were collected for all subjects (DPP-4i users, DPP-4i non-users, and controls) every year from the index date.
Statistical analyses
Baseline characteristics of the subjects in the three groups (controls, DPP-4i users, and DPP-4i non-users) are expressed as means and standard deviations for continuous variables, and as percentages for categorical variables. To compare the characteristics between groups, we performed a χ2 test or Fisher's exact test for the categorical variables, and an analysis of variance or Kruskal-Wallis rank sum test for continuous variables. A survival analysis using Cox models was performed to measure the risk of osteoporosis and bone fractures in the three groups over time. Possible effects of the DPP-4i treatment were analyzed. All statistical analyses were performed using SAS version 9.3 (SAS Institute Inc., Cary, NC, USA) and R version 3.4.4 (R Foundation for Statistical Computing, Vienna, Austria).
Ethics statement
This study was approved by the Institutional Review Board (IRB) of Kyung Hee University Hospital (IRB No. KHUH 2017-06-002-006). The informed consent was obtained from all participating subjects.
Go to :
RESULTS
Baseline characteristics of the subjects
A total of 11,164 subjects were extracted from NHIS-NSC2.0 cohort and classified as DPP-4i users (n = 1,410), DPP-4i non-users (n = 4,172), or controls (n = 5,582) (Table 2). The mean follow-up period was 3.11 years for DPP-4i users, 4.09 years for DPP-4i non-users, and 3.62 years for controls. DPP-4i users were younger than DPP-4i non-users (P < 0.001), whereas controls were younger than DPP-4i users (P < 0.001). There was a higher proportion of men than women in all three groups. More DPP-4i non-users (84.30%) than DPP-4i users (58.44%) took metformin (P < 0.001). Similarly, more DPP-4i non-users than DPP-4i users took sulfonylurea, meglitinide, α-glucosidase inhibitors, and TZD (P < 0.05). There was no difference in insulin or SGLT2 inhibitor use between DPP-4i users and non-users. Significantly more DPP-4i non-users than DPP-4i users took the following hypertension medications: ARB (26.53% vs. 10.92%, P < 0.001), ACE inhibitors (2.78% vs. 0.92%, P < 0.001), CCB (25.55% vs. 9.50%, P < 0.001), diuretics (16.75% vs. 4.82%, P < 0.001), and beta blockers (9.88% vs. 3.26%, P < 0.001). More controls than DPP-4i users took CCB (14.85% vs. 9.50%, P < 0.001), diuretics (8.01% vs. 4.82%, P < 0.001), and beta blockers (5.82% vs. 3.26%, P < 0.001). Significantly more DPP-4i non-users than users or controls took statins to treat dyslipidemia (DPP-4i non-users, 25.72%; DPP-4i users, 13.40%; controls, 8.65%; P < 0.001). The DPP-4i users had a significantly higher CCI value (mean = 1.87) than that of the control group (mean = 0.37, P < 0.001). The DPP-4i users also had a significantly higher DCSI value (mean = 0.51) than that of the control group (mean = 0.10, P < 0.001). There were no differences in CCI or DCSI between DPP-4i users and non-users.
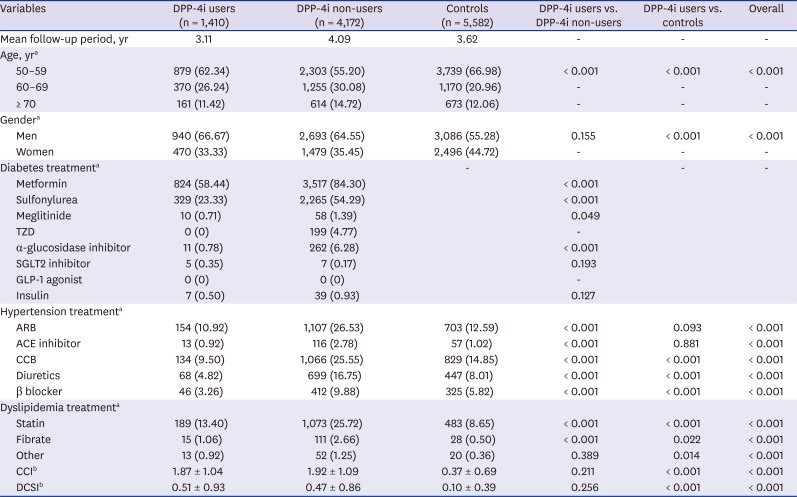
Table 2
Baseline characteristics
Data are presented as mean ± standard deviation or number (%).
DPP-4i = dipeptidyl peptidase 4 inhibitor, TZD = thiazolidinedione, SGLT2 inhibitor = sodium glucose cotransporter 2 inhibitor, GLP-1 agonist = glucagon-like peptide-1 agonist, ARB = angiotensin II receptor blocker, ACE inhibitor = angiotensin-converting enzyme inhibitor, CCB = calcium channel blocker, CCI = Charlson comorbidity index, DCSI = diabetes complications severity index.
aby analysis of variance; bby Kruskal–Wallis rank sum test.
![]()
The effects of DPP-4i use on osteoporosis and fractures
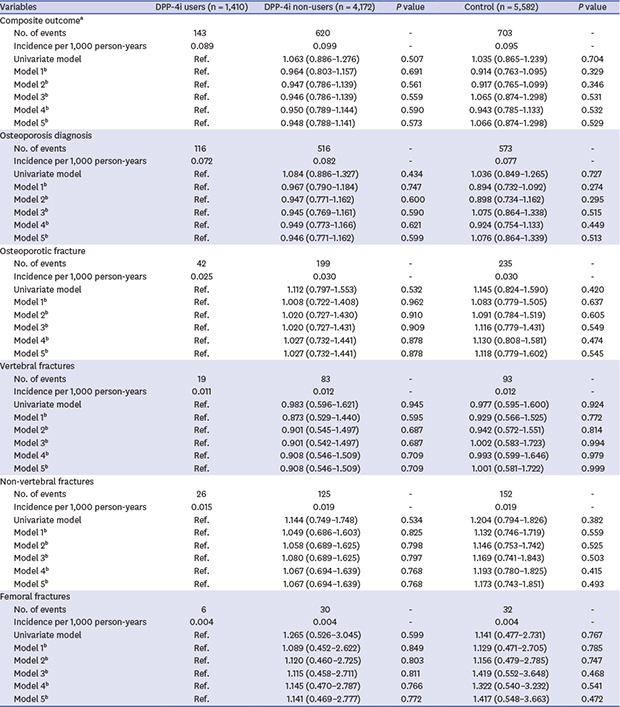
The incidence of the composite outcome (osteoporosis, osteoporotic fractures, vertebral fractures, non-vertebral fractures, and femoral fractures) per 1,000 person-years was 0.089 in DPP-4i users, 0.099 in DPP-4i non-users, and 0.095 in controls (Table 3). The hazard ratio (HR) for the composite outcome was 1.063 (95% confidence interval [CI], 0.0886–1.276) in DPP-4i non-users and 1.035 (95% CI, 0.865–1.239) in controls compared with DPP-4i users. The results were consistent after adjustment for covariates such as age, gender, CCI, DCSI, hypertension treatment, or dyslipidemia treatment.
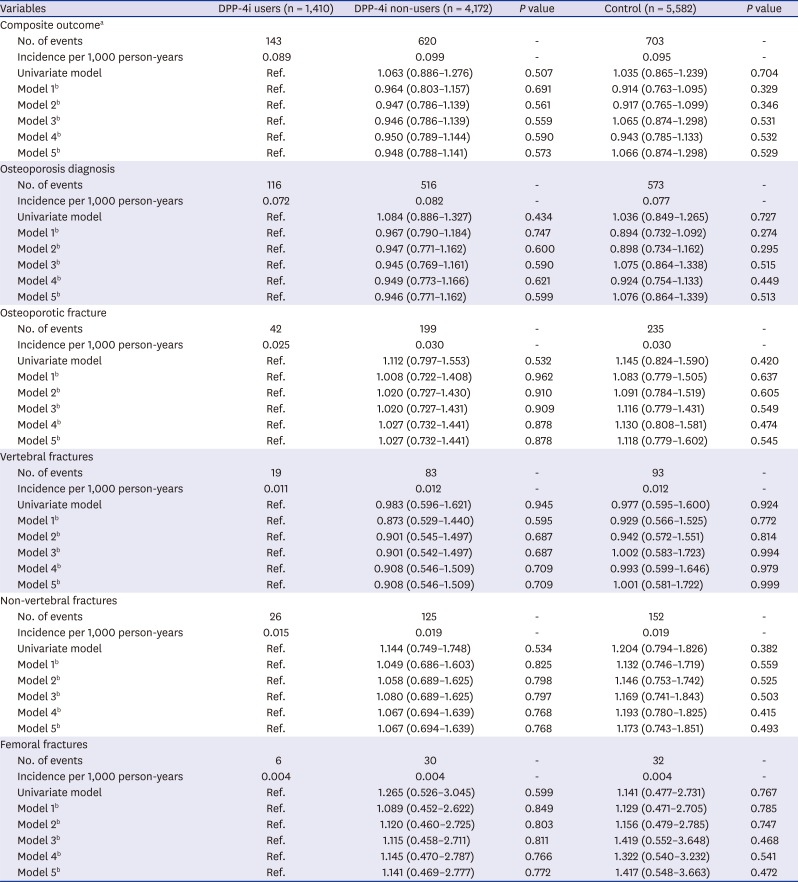
Table 3
The effect of DPP-4i on fracture risk
Multivariate Cox models.
DPP-4i = dipeptidyl peptidase 4 inhibitor, Ref. = references, DCSI = diabetes complications severity index, CCI = Charlson comorbidity index.
aComposite outcome: osteoporosis, osteoporotic fractures, vertebral fractures, non-vertebral fractures, femoral fractures; bModel 1: corrected for age and gender, model 2: corrected for age, gender, hypertension treatment, and dyslipidemia treatment, model 3: corrected for age, gender, hypertension treatment, dyslipidemia treatment, and CCI, model 4: corrected for age, gender, hypertension treatment, dyslipidemia treatment, and DCSI, model 5: corrected for age, gender, hypertension treatment, dyslipidemia treatment, CCI, and DCSI.
![]()
The incidence of osteoporosis diagnosis per 1,000 person-years was 0.072 in DPP-4i users, 0.082 in DPP-4i non-users, and 0.077 in controls. The incidence of osteoporotic fractures per 1,000 person-years was 0.025 in DPP-4i users, 0.03 in DPP-4i non-users, and 0.03 in controls. The incidence of vertebral fractures per 1,000 person-years was 0.011 in DPP-4i users, 0.012 in DPP-4i non-users, and 0.012 in controls. The incidence of non-vertebral fractures per 1,000 person-years was 0.015 in DPP-4i users, 0.019 in DPP-4i non-users, and 0.019 in controls. The incidence of femoral fractures per 1,000 person-years was 0.004 in DPP-4i users, 0.004 in DPP-4i non-users, and 0.004 in controls. The HRs for osteoporosis diagnosis, osteoporotic fractures, vertebral fractures, non-vertebral fractures, and femoral fractures in DPP-4i non-users and controls were not significantly different from those in DPP-4i users, both before and after adjustment (Table 3). The results of subgroup analyses according to gender and age were consistent (data not shown).
Go to :
DISCUSSION
In this study, we analyzed the effects of DPP-4i on osteoporosis and fractures by comparing the incidence of osteoporosis and fractures between DPP-4i users and DPP-4i non-users, and found no significant effect of DPP-4i on fracture risk. DPP-4i users did not have a significantly different risk than non-users of the composite outcome (i.e., all outcomes considered simultaneously: osteoporosis, osteoporotic fractures, vertebral fractures, non-vertebral fractures, and femoral fractures), nor did they have a significantly different risk of any outcome considered separately.
DPP-4i reduces plasma glucose levels by inhibiting degradation of endogenous incretins, and increases plasma levels of GLP-1, GLP-2, and GIP.14 Some studies have reported that GIP and GLP-2 may affect bone metabolism. GIP stimulates insulin and amylin secretion from pancreatic β cells and glucagon from pancreatic α cells.21 Amylin is structurally homologous to calcitonin and acts similarly to calcitonin in calcium homeostasis.22 Amylin inhibited bone resorption in vivo and fusion of mononucleated osteoclast precursors into multinucleated osteoclasts in vitro.23 GIP receptors are present in normal bone and osteoblast-like cell lines, and GIP increases intracellular calcium levels, cellular cAMP content, type 1 collagen expression, and ALP activity in these cells.24 In GIP- receptor-knockout mice, bone formation is decreased, resulting in reduced bone size.25 After GLP-2 administration, significant suppression of bone resorption and increased total hip BMD were reported.2627
The results of this study do not support the beneficial effect of DPP-4i on bone metabolism. Although DPP-4i use is associated with increased bone formation, it is associated more with mechanisms related to the suppression of bone resorption. Thus, the potential positive effect of DPP-4i on osteoporosis and fractures might be more apparent in postmenopausal women with markedly increased bone resorption. However, our study population consisted of many more men than women, which may have affected the results. Additionally, the effects of DPP-4i on bone metabolism observed in vivo or in vitro may have lower potency in humans, because various diseases or medications that more strongly affect bone metabolism may be present in practice. We adjusted for these confounding factors as much as possible in this study. A randomized controlled trial is needed to minimize the impact of confounding factors.
A previous study reported the effects of diabetes medications on fracture risk in a Korean population using a nationwide medical claims database.28 Choi et al.28 performed an analysis on the effects of anti-diabetic drugs (sulfonylurea, an alpha-glucosidase inhibitor, and metformin) and a combination of treatments (metformin and sulfonylurea, metformin and TZD, sulfonylurea and TZD, and metformin and DPP-4i) on the risk of fractures in a Korean population. They found a decreased risk in the group treated with metformin and DPP-4i, suggesting that DPP-4i has a protective effect when administered with metformin. By contrast, our study focused on the effect of DPP-4i alone. The longer follow-up period and more detailed outcomes classified by osteoporosis diagnosis, osteoporotic fractures, vertebral fractures, non-vertebral fractures, femoral fractures, and composite outcome were advantages of our study. Additionally, morbidities were assessed using the DCSI and adjusted for the CCI in this study. We adjusted for some medications for hypertension and dyslipidemia that may affect bone metabolism. The results are conflicting, but ARB, ACE inhibitors, beta blockers, and thiazide diuretics have been reported to affect bone metabolism in some studies.293031 Statins have been reported to reduce the risk of osteoporosis.32
Our study had some limitations. First, the baseline of the cohort started at the advent of DPP-4i use in Korea. Therefore, the number of DPP-4i users was small at the beginning of the study compared with the present. Second, because this study used claims-based data, it was difficult to ascertain continuous use of drugs in all subjects during the follow-up period. Nevertheless, subjects treated with DPP-4i for more than 100 days were analyzed, and most users had used this treatment continuously. We also used the standard methodology of many claims-based studies. Third, because the proportions of use of other medications may be extracted from the combination use, it could affect the results. Nevertheless, despite the limitations, the results of this study provide additional information on the effect of DPP-4i on the risk of fractures in a Korean population and support previous results. Further studies including more women with a better design and longer follow-up period are needed in the future.
In conclusion, this study found that DPP-4i had no significant effect on the risk of fractures in a Korean population.
Go to :
 XML Download
XML Download