

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The prime consideration in the management of children in dentistry is dental anxiety. It is defined as an abnormal fear or dread of visiting the dentist for preventive care or therapy and unwarranted anxiety over dental procedures [1], and may have psychological, cognitive, and behavioral consequences. It is shown that dental anxiety may persist into adulthood, leading to neglect or avoidance of dental needs that affects the oral health considerably [23]. Recognition and assessment of dental anxiety is especially important in children needing special care with respect to dental fear and anxiety [4].
Till date, the literature shows various methods of assessing dental anxiety, including indirect methods (physiologic measurements of pulse rate, blood pressure, and muscle tension) [5] or projective techniques (children's dental fear picture test) [6] that require skills in carrying out interviews, and administering and scoring tests. The latter exhibited questionable reliability and validity due to difficulties in the interpretation of stories and standardizing scores. Psychological tests commonly used in children include the Corah's dental anxiety scale (CDAS) [7], modified child dental anxiety scale (MCDAS) [8], and children's fear survey schedule dental sub-scale (CFSS-DS) [9], as well as picture tests such as the Venham picture test (VPT), facial image scale (FIS), and Raghavendra, Madhuri, Sujata – pictorial scale (RMS-PS) [4101112]. However, each scale has certain limitations. An ideal anxiety scale should be easy to apply clinically, less time consuming, appealing, applicable in younger children with limited cognitive and linguistic skills, and incorporate a scoring system. Considering the aforementioned points, a new anxiety scale, animated emoji scale (AES), was designed using motion emoticons/animojis. This was based on the interest and attraction of today's generation towards multimedia, and their preference of motion pictures on electronic devices rather than still cartoons on paper. Validity of any psychometric instrument is determined by assessing whether the instrument measures what is intended, by correlating it with the instrument designed to measure the same phenomenon.
Thus, the aim of this study was to validate the new AES for dental anxiety assessment in children, and to compare it with more frequently used picture tests such as FIS and VPT.
MATERIALS AND METHODS
1. Sample size estimation:
The sample size was estimated using the G Power software, version 3.1.9.2. Based on the published literature [10] and considering the effect size to be measured (ρ) at 27%, i.e., correlation coefficient between the variables at 0.27, power of the study at 80%, and margin of error at 5%, the total sample size was estimated to be 102.
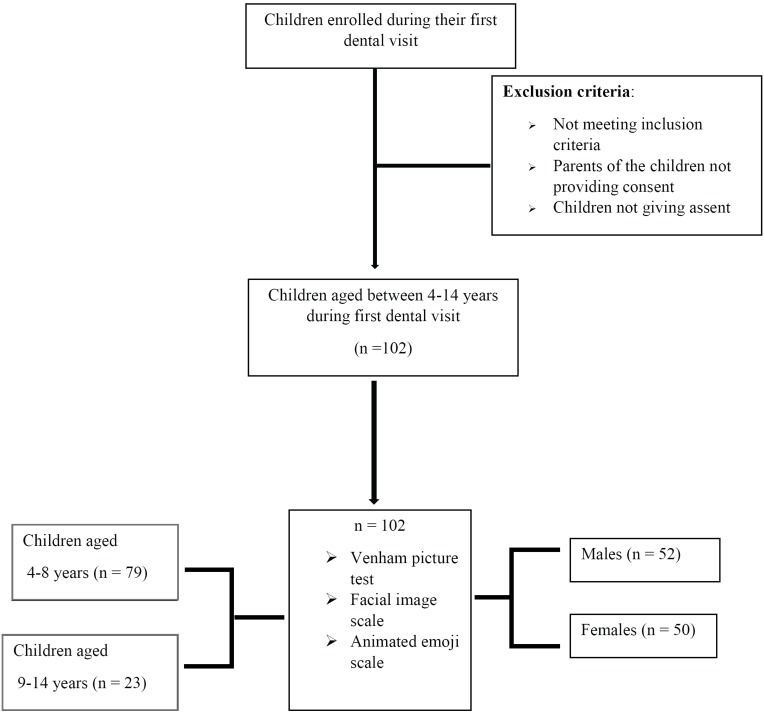
This study randomly recruited 102 children, aged 4–14 years, visiting the Department of Pediatric and Preventive Dentistry, M.R. Ambedkar Dental College and Hospital, at their first dental visit; we conducted a simple dental examination. Only those children who gave their assent and whose parents provided informed consent were selected as a part of the study investigating the emotions of children towards dentistry. These children exhibited otherwise normal mental and physical natures. The study was initiated after obtaining approval from the Institutional ethical committee and review board (IRB Number: MRADC&H/ECIRB/0827/2016-17). All children reporting to the department for their first dental visit and fulfilling the above criteria were consecutively included in the study until the desired sample size was achieved.
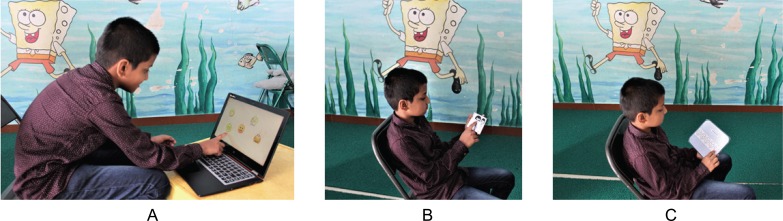
Each child's dental anxiety was measured using three different scales: AES, VPT, and FIS. The order of presentation of the scales to each child was based on a computerized sequence generation; all the scales were presented to each patient by a single investigator, and the anxiety scores were immediately recorded to ensure reliability and avoid bias (Fig. 1).
The AES has five graphic interchange formats of animated emoji faces showing different feelings ranging from very happy/laughing to very unhappy/sad and crying (most positive to most negative feelings). The child was asked to choose one of these animated emojis on the electronic display that best matched their feelings at that moment. The scale had scores from 1 (very happy emoji) to 5 (very unhappy emoji) as shown in Fig. 2 and Video 1.
The FIS comprises a row of five faces ranging from very happy to very unhappy. The children in our study were asked to point at the face that they most associated with at that moment. The scale was scored by giving a value of 1 for the most positive face and 5 to the most negative face (Fig. 2).
The VPT comprises eight cards with two figures on each card, one denoting an anxious figure and the other, a non-anxious figure. The children were asked to point at the figure that mirrored their emotion at that moment. All cards were shown in a consecutive order. A score of 1 and 0 were recorded when the children pointed at the anxious and non-anxious figures, respectively. The number of times the anxious figure was chosen was summed to attain the final score (minimum score, 0; maximum score, 8; Fig. 2).
Once all the three scales were presented to the child and anxiety scores were collected, the information of the most preferred scale of the children was also recorded.
The data collected was tabulated and subjected to statistical analyses using SPSS statistical software package, version 22.0. Descriptive analysis of all the explanatory and outcome parameters was performed using frequency and proportions for categorical variables, and using mean and standard deviation (SD) for continuous variables. Independent student t-test and Friedman's test were used to compare the mean age and the mean anxiety rating scores of different rating scales between sexes, respectively. Pearson correlation test was used to correlate the anxiety rating scores between different rating scales. Chi square test was used to compare the preference/liking of the different anxiety rating scales between sexes. The level of significance was set at P < 0.05.
RESULTS
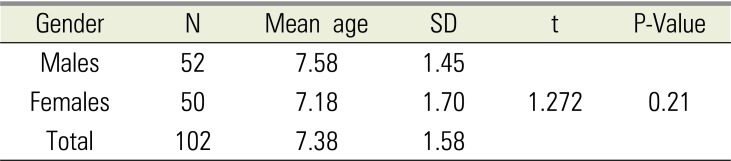
Among the 102 children enrolled at their first dental visit, 52 were male and 50 were female, with mean ages of 7.58 ± 1.45 and 7.18 ± 1.70 years, respectively; there was no significant difference in the mean ages of male and female children (Table 1). As the patients were recruited in a sequential manner, there were 79 children in the 4–8 years age group and 23 children in the 9–14 years age group.
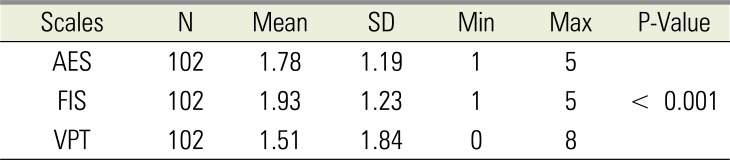
The mean anxiety scores measured using AES, FIS, and VPT, represented as mean ± SD, were 1.78 ± 1.19, 1.93 ± 1.23, and 1.51 ± 1.84, respectively. There was significant difference in the mean anxiety scores between the three scales with Friedman's test (P < 0.001). (Table 2).
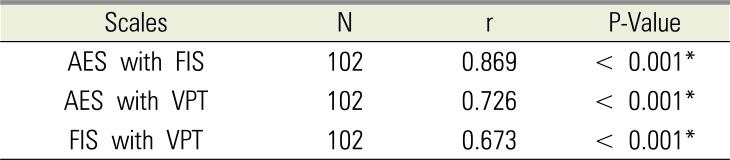
1. Correlation of AES with FIS and VPT
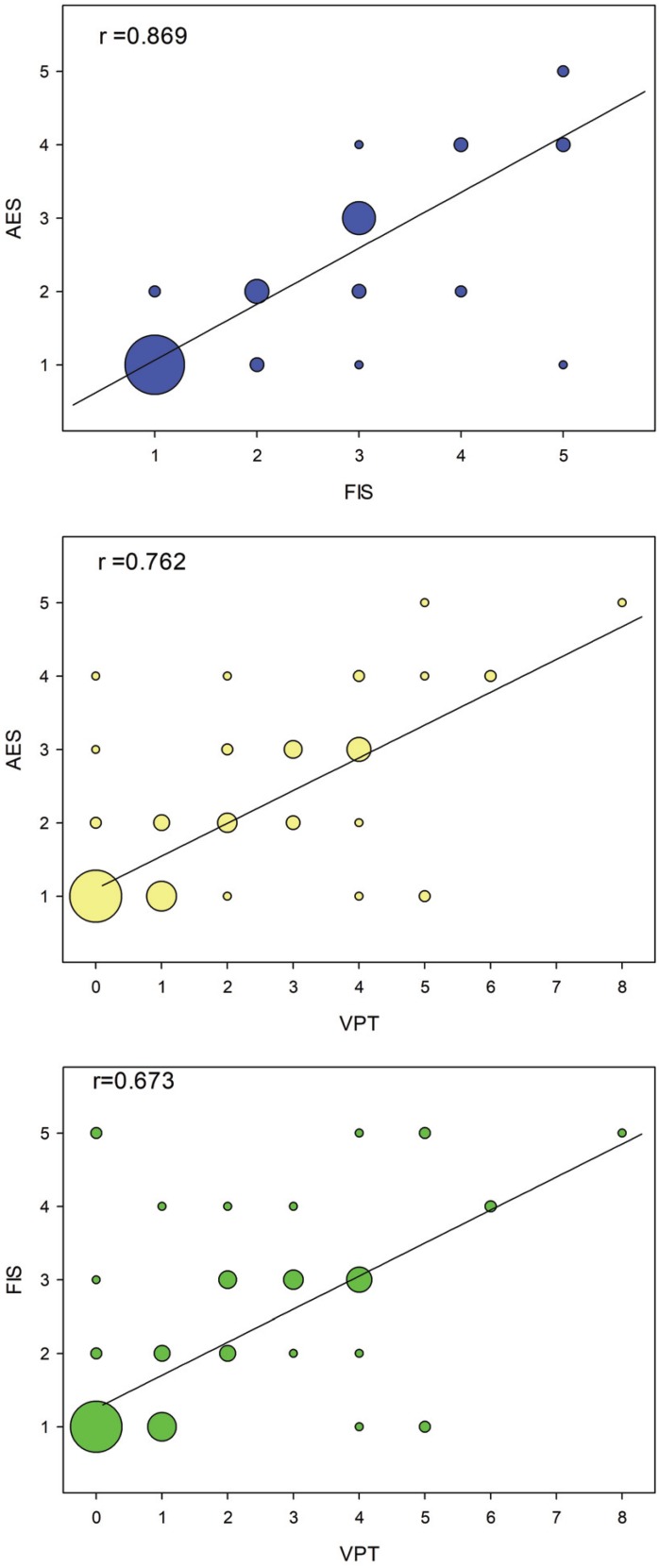
Pearson correlation test was performed to evaluate the correlation of AES with VPT and FIS. A very strong correlation (r = 0.726, P < 0.001) was found between AES and VPT, which indicated that AES measured anxiety similar to VPT. Strong correlations between AES and FIS (r = 0.869, P < 0.001) and between FIS and VPT (r = 0.673, P < 0.001) were seen, indicating that anxiety was determined similarly between the scales (Table 3, Fig. 3).
2. Preference and liking for different anxiety tests
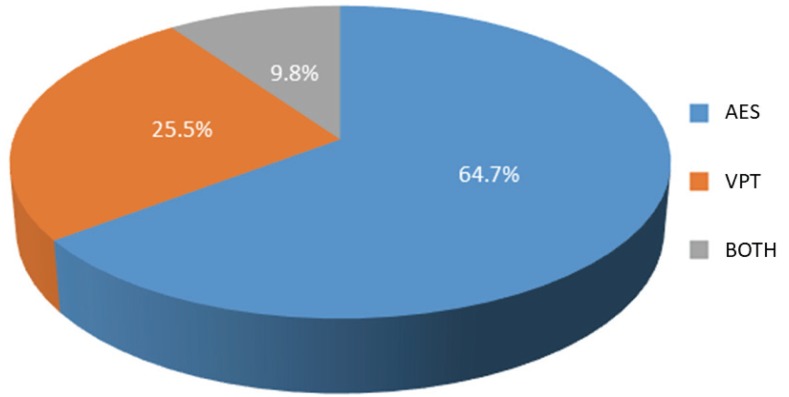
The participants in this study preferred AES over VPT and FIS, and none of them preferred FIS. The preference of the different scales by the children in all the groups was in the order of AES > VPT > FIS. This liking was more pronounced in females and in the younger age groups (70% and 69.6%, respectively). However, there was no statistically significant difference observed in the different age groups and sexes with respect to the preference between particular anxiety scales (Table 4 and Fig. 4).
DISCUSSION
Dental anxiety in children is a very common problem developing mostly in childhood and adolescence [1314], and is often distressing to the child, parents, and dental practitioners. Approximately half of the children report low to moderate dental anxiety, while 10%–20% report high levels [1516]. During the visit to a dental clinic, the child faces unfamiliar people, representing potentially threatening and invasive situations for children. Those who are more vulnerable may find it difficult to cope with these new experiences and hence become anxious. Unsurprisingly, anxiety related behaviors have been recognized as the most difficult part of child guidance in dental operatory [1718]. Therefore, it is necessary to identify and quantify anxiety.
According to Buchanan [4], an ideal anxiety assessment scale should be short in length to maximize response from the children and minimize the time for administration, should include items most relevant to the pediatric dental experience, should easily hold the attention of the child, and should be simple to score and interpret. Moreover, the scale should be easy to apply in younger children with limited cognitive ability and linguistic skills.
Our study compared FIS and VPT with AES, as they were picture scales used for measuring anxiety in young children during their first dental visit.
Present study showed a strong correlation between all the scales (Table 3). However for the study interest the comparison of mean anxiety scores among the scales using Friedman's test (Table 2) showed significant difference. This difference can be attributed to lower mean anxiety score of VPT (1.51) as compared to AES (1.78) and FIS (1.93). Lower mean anxiety scores with respect to VPT obtained is similar to the findings of Buchanan and Niven [4], Shetty RM et al [10] and is in contrast to the study by Sadana et al [6].
The validity of the novel AES was supported by its high degree of agreement with VPT and FIS. Dental anxiety measurements with AES showed a very strong correlation with VPT, and children preferred the former as there was no confusion with the figures as seen in VPT cards, where certain figures looked similar and were often time consuming to interpret. Furthermore, the current generation children are exposed to expressing their feelings using emojis on multimedia on various social networking applications; hence, this makes AES highly attractive to young children as it comprises of motion emoticons. VPT had all cards with male pictures and a young female might find it difficult to correlate them with her anxiety, whereas AES has emojis common to both males and females.
A strong correlation was also found between AES and FIS. FIS according to Buchanan and Niven [4] is a good scale to measure dental anxiety in children. In FIS, young children often face difficulties interpreting the drawings of facial expressions, and hence, none of the subjects in our study preferred FIS over the other two scales used. In younger children with limited linguistic and cognitive abilities, AES offers many advantages. It is very attractive, easy for children to relate with feelings, less time consuming, universal (no languages or questionnaires are used), common to both sexes, and offers immediate scoring of dental anxiety, thus helping the dental team to use appropriate behavior management modalities for efficient and effective dental treatment. AES is a novel and child-friendly alternative for assessment of anxiety in children. Dental anxiety measured using AES was similar to that measured using VPT and FIS. AES offers a simple, attractive, quick, easy, and efficient method for assessing dental anxiety in children during their dental visit. Thus, it helps in directing the use of appropriate behavioral management techniques in establishing a trustworthy relationship and good rapport between the child, parent, and pediatric dentist.


 XML Download
XML Download