

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
With increasing numbers of total hip replacements (THR) due to aging populations1234), periprosthetic femoral fractures (PFFs) are a major challenge for orthopaedic surgeons. Among several complications associated with primary THR, the prevalence of PFFs has been increasingly reported; the incidence varies in different literature reports from 0.1% to 4%567). The Vancouver classification system is a useful tool which has been confirmed to be reliable and valid for the diagnosis and management of PFFs8). There is little controversy regarding the treatment of trochanteric fractures (Type AG and AL) or of fractures distal to the stem (Type C) relating to fixation techniques. However, Vancouver type B1 fractures with stable stem should be treated using open reduction and internal fixation with cortical strut allografts or a cable-plate. The Vancouver type B1 fractures, defined as fractures around or just distal to a well-fixed femoral stem are clearly associated with many complications because of their inherent instability9). Cable-plate systems have become commonly used for the fixation of type B1 periprosthetic fractures, and Tadross et al.10) reported on seven hip periprosthetic fractures treated with cable and plate fixation. Although three patients achieved union and satisfactory results, the other four patients were considered to have failed because of nonunion (n=2) and malunion (n=2).
An analysis of prognostic factors relating to the treatment of PFF using cable-plates was lacking. The treatment of PFFs requires particular care because stable fixation is difficult in this situation as compared to ordinary fractures; significant effort has been spent to properly classify and treat PFFs1112). The purpose of this study was to assess clinical outcomes and analyze potential prognostic factors in the treatment of PFFs using the cable-plate construct.
Go to : 
MATERIALS AND METHODS
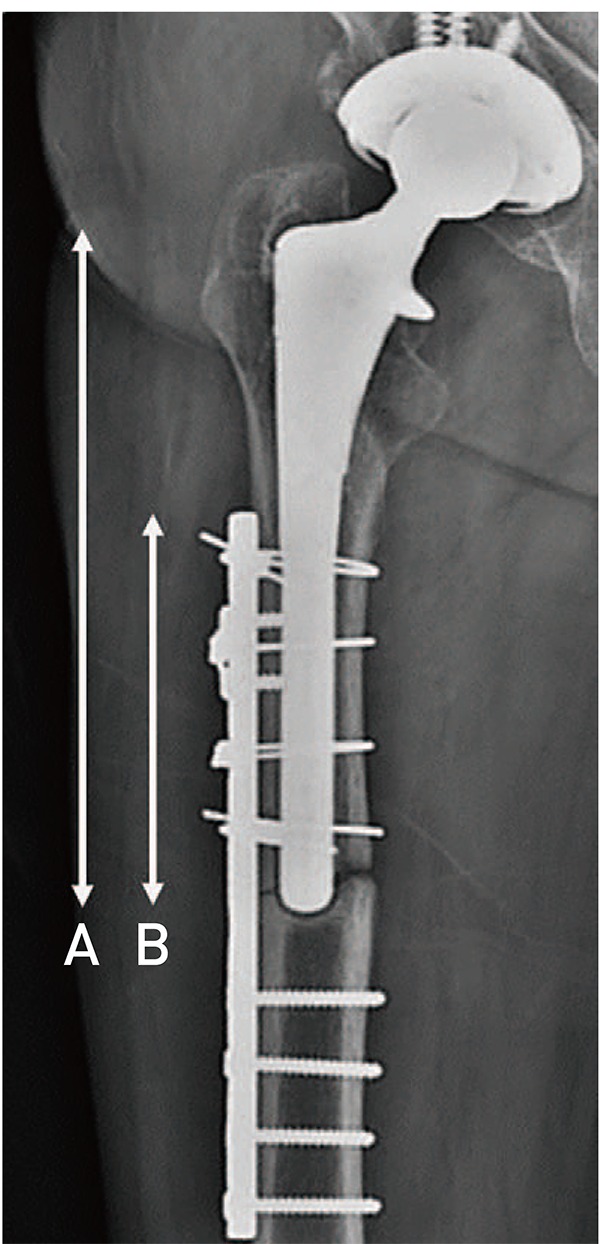
We retrospectively reviewed a consecutive series of 41 patients (41 hips) of the Vancouver type B1 fractures treated by osteosynthesis using the cable-plate construct for fixation between January 2003 and February 2016. The Cable Ready® plate (Zimmer, Warsaw, IN, USA) was used as the cable-plate system in 25 cases. When unicortical proximal locking screws were considered to be available for additional fixation, we used the AO locking compression plate (Synthes GmbH, Oberdorf, Switzerland) in 16 cases with cable fixation of the proximal segment. This study included 20 males and 21 females, with an average age of 67.3±12.1 years (range, 42–86 years). The mean follow-up period was 31.5±11.6 months (range, 12–58 months). All previous hip arthroplasty procedures were conducted using a cementless femoral stem, and the injury mechanism was a low-energy fall from standing height or falling out of bed or a chair in all patients. We analyzed the factors affecting fracture healing after PFFs between the union group (Group I) and healing failure group (Group II), including: i) fracture pattern (spiral or transverse), ii) implant type (cable-plate or locking compression plate), iii) plate overlap percentage of stem length (Fig. 1), iv) number of screws or cables used, v) patient's age, vi) sex, and vii) T-score at bone mineral density (BMD). This study has been approved by INHAUH Institutional Review Board (number: 2016-12-017).
1. Surgical Procedures
All surgical procedures were performed by one senior surgeon in the operating room with laminar flow. Through an extended posterolateral approach, the anatomical reduction was performed with minimal stripping of periosteum. The stability of femoral stems was assessed by the presence of thigh pain before injury, the stem subsidence and the radiolucent line around femoral stem. After fracture reduction under direct vision, we used the cable-plate construct with sufficient length for the stability of fracture site and adequate proximal fixation of the PFFs. Distal to the tip of femoral stem, at least six cortices (range, 6–16) were fixed through bicortical screws of 4.5-mm diameter13). When a healing failure was predicted intraoperatively due to the unstable fixation of plate related to fracture pattern or osteoporotic bone, fresh frozen cortical strut onlay allograft was additionally performed to improve stability or bone quality; the allograft was placed in the anterior or medial aspect of the femur depending on feasibility of application. Fresh-frozen cortical strut onlay allografts with an average length of 18 cm (range, 16–20 cm) were augmented with cerclage wires and bicortical screws. Image intensification was used intraoperatively to re-assess fixation.
2. Clinical Assessment
All patients were monitored clinically at postoperative six weeks, three and six months, and annually. We used the Harris hip scoring and pain visual analogue scale (VAS) for evaluation of the postoperative outcomes. Patient-related complications (e.g., wound infection [superficial or deep], symptomatic pulmonary embolism or deep vein thrombosis, neurovascular injuries, postoperative death), were recorded.
3. Radiographic Assessment
Postoperative radiographs were assessed for evidence of fracture healing and construct loosening or consolidation. We defined union as the appearance of bridging callus on at least one cortex on both anteroposterior and lateral radiographs. Delayed union was defined as healing that has extended beyond six months from the time of surgery. A healing failure was defined as a complication that required revision surgery. Implant-related complications, including implant failure and subsequent need for revision surgery, were also assessed.
4. Postoperative Management
All patients used crutches or a walker with toe-touch weight bearing after six weeks postoperatively. Progressive weight bearing was then encouraged, with all patients encouraged to bear weight fully after a maximum of three months from the date of fracture fixation.
5. Statistical Analyses
Various statistical tools were used to analyze the union group (Group I) and healing failure group (Group II). All statistical analyses were performed with IBM SPSS Statistic program ver. 19.0 (IBM Corp., Armonk, NY, USA), and P<0.05 was considered statistically significant. In the univariate analysis, the Student t-test or Mann–Whitney U-test was used for analysis of continuous variables, and the χ2 test or Fisher exact test was used for categorical variables. In the multivariate analysis, logistic regression was performed using statistically significant factors in the univariate analysis. The paired t-test was used to compare functional scores between preoperatively and final follow-up.
Go to :
RESULTS
The functional score (Harris hip score) and pain VAS revealed a significant improvement at the time of the final follow-up (65.6±3.7 to 94.1±5.2 and 6.7±1.1 to 2.1± 1.4, respectively; all P<0.05). Fracture union was obtained in 29 hips (70.7%; Group I) after an average of 13.5 weeks (range, 12–24 weeks) (Fig. 2). Healing failure of surgical treatment was observed in 12 cases (29.3%; Group II), which were a delayed union (n=10) and nonunion (n=2) (Fig. 3). A total of two cases had an atypical periprosthetic fracture (Group I [n=1), Group II [n=1]); there was no significant difference between the two groups. A total of three cases were successfully treated by cortical strut onlay allograft related to the unstability or poor bone quality.
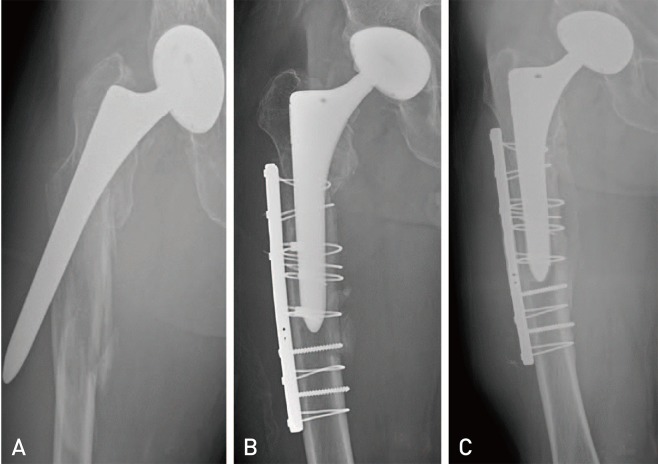 | Fig. 2(A) Preoperative X-ray of a 57-year-old male with Vancouver type B1 spiral fracture, having severe osteoporosis with bone mineral density −3.8, who visited after slip down. (B) Postoperative X-ray after open reduction and internal fixation carried out with cable-plate construct. Fracture union was obtained four months after surgery. (C) Follow-up X-ray two years after surgery showing good union and stable fixation of femoral stem.
|
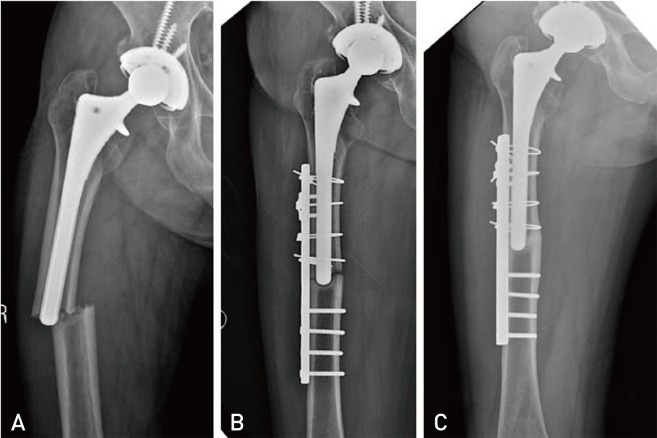 | Fig. 3(A) Preoperative X-ray of a 72-year-old female with a Vancouver type B1 transverse fracture around or just distal to a well-fixed femoral stem, having severe osteoporosis with bone mineral density −4.0, who visited after slip down. (B) Postoperative X-ray after open reduction and internal fixation carried out with cable-plate construct. (C) Follow-up X-ray 10 months after surgery showing delayed union.
|
All cases were treated by cable-plate construct without stem change, including a 10-hole cable-plate (n=17), an 8-hole cable-plate (n=8), a 13-hole locking compression plate (n=6), and an 11-hole locking compression plate (n=10); all were placed in the lateral aspect of the femur. Plates were stabilized with an average of 3 or 4 cables (range, 2–8) tightened by a custom tensioner in the proximal segment of the femur. An average of three or four unicortical proximal screws (range, 2–7) ranged in length from 14 to 16 mm were used to stabilize the locking compression plates which were placed in the proximal segment of the femur.
There were no significant differences in number of screws and cables used between two groups. Neither the age of the patient at the time of the surgery or the implant type influenced clinical outcomes (all P>0.05). Transverse type fractures around or just distal to a well-fixed femoral stem was noted in six cases (50.0%) of Group II, presenting significantly higher rate of complications compared to spiral type fractures (P=0.040). A statistically significant difference of BMD between two groups was observed. The mean T-score (−3.1±0.9) at BMD in Group II, a value known to be associated with surgical complications was significantly lower than Group I (T-score of −2.2±1.1 [P=0.011]). The mean percentage of plate overlap to stem length (81.0±8.8%) in Group I was significantly higher than that of Group II (67.0±6.3%) (P<0.001) (Table 1). However, in the multivariate analysis using logistic regression, the percentage of plate overlap to stem length (P<0.001) and T-score at BMD (P=0.033) were independent prognostic factors for union after treatment using the cable-plate in PFFs (Table 2).
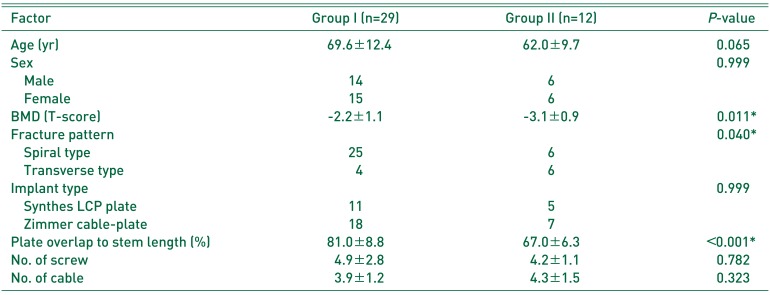

Table 1
Prognostic Factors Affecting Clinical Outcomes as Assessed Using Univariate Analysis
![]()
Table 2
Prognostic Factors Affecting Clinical Outcomes as Assessed Using Multivariate Analysis with Logistic Regression
![]()
No clinical complications, such as wound infection (superficial or deep), symptomatic pulmonary embolism or deep vein thrombosis and neurovascular injuries, were detected.
Go to :
DISCUSSION
The principal finding of this study was that the preoperative T-score at BMD and plate overlap percentage to stem length were significantly lower in the healing failure group compared with the union group, and fracture patterns around or just distal to a well-fixed femoral stem were strongly correlated with union rate after surgery. These findings should be useful for physicians and help them predict prognosis in the clinical setting, which require the physician to perform surgeries with caution to help improve stability or bone quality.
Displaced fractures around or just distal to a well-fixed femoral stem, the Vancouver type B1 fractures could be typically treated with open reduction and internal fixation; however, the standard guidelines for proper fixation methods remain unclear. Although distal fragment fixation is generally reliable with standard locked or non-locked bicortical screws, biomechanical purchase of the proximal segment is difficult due to the presence of the hip prosthesis with or without a cement mantle14). Available options for proximal fixation of plate include cables with cerclage wires, unicortical screws, allograft struts, and more recently, plate designs that allow bicortical fixation by directing offset locking screws tangentially around either side of the hip stem14). Some concerns remain, such as the limitation that screw fixation with proximal unicortical locked screws in the vicinity of a THR can create stress risers in local bone leading to refracture15). The increased strength afforded by cortical screws placed near (or through) the cement mantle may be offset by the risk of prosthesis loosening due to violation of the cement mantle1516). Cables, rather than other alternatives, can be used for stable fixation, and fixation strength also tends to increase with the number of cables used. These cables can also help bring the plate into contact with the bony contour, which is an effective method for reducing soft tissue impingement and the risk for plate pullout. The cable-plate is effective when proximal screws are not available, such as when a prosthesis occupies the canal of the bone, designed to support axial loading due to column support of the cables. In this study, fracture union was obtained in 29 hips using the cable-plate construct (70.7%) without any complications.
The prognosis of treatment for PFFs may vary depending on the fracture location or fracture pattern. The tip of the hip stem itself functions as a stress riser and is one of the contributing factors in such fractures17). Long oblique or spiral fractures are the most stable, so plates offer the advantage of providing rotational stability by screws fixed on either side of the fracture181920). However, regarding rotational unstability and lower contact area, transverse type fractures tend to unite slowly1821). The transverse type fracture distal to a well-fixed stable stem should be treated more carefully because of inherent instability. In principle, the plate should be of sufficient length for firm fixation because a longer plate with empty screw holes at the fracture site provides a longer working length than a short plate. Previous reports recommend that the plate used for internal fixation must be of sufficient length to allow as much overlap of the femoral stem as possible1222). A longer plate ending near the end of the bone is preferable to the one ending in the metadiaphyseal zone. Recent papers have also mentioned Less Invasive Stabilization System (LISS), promising early results with locking compression plate including axial and angular stability2324). These studies concluded that the preservation of fracture site vascular supply via use of minimally invasive insertion techniques decreases periosteal stripping and reduces blood loss. Min et al.25) concluded that the radiological and clinical outcomes of LISS using locking compression plate in patients with Vancouver type B1 PFFs were shown not to be inferior to open reduction and resulted in fewer intraoperative complications than open reduction. Therefore, a sufficient plate overlap to stem length may be essential to prevent healing failure without longer dissection. In this study, Group II (i.e., those with healing failure including delayed union or a nonunion) had a significantly lower plate overlap percentage to stem length, as compared to Group I (i.e., those who achieved union).
PFFs present an important challenge to an orthopaedic surgeon due to a greater degree of osteoporosis than in the situation when the primary surgery had been performed for arthritis9). As the cortical host bone does not provide adequate stability for anchorage, reconstruction with cortical strut onlay allografts may be considered. Fractures involving the medial cortex or those that are short and transverse in origin will benefit from the addition of both plate fixation and cortical strut onlay allografts to ensure biplanar fixation26). Howell et al.27) showed high rates of fracture union using the cable-plate and cortical onlay allograft combined fixation methods for fractures that occur around well-fixed implants. Similarly, Kim et al.28) suggested that cortical strut onlay allografts facilitate the mechanical stability and the biological fracture healing in addition to plate fixation of Vancouver type B1 PFFs. However, a recent systematic review of 37 manuscripts with 682 Vancouver B1 fractures revealed an increased infection rate for those patients treated with allograft augmentation (8.3% vs. 3.8%) and time to union (6.6 months vs. 4.4 months) as compared to those treated without allograft29). In this study, the transverse type fractures just distal to a well-fixed stem occurred in a total of 10 patients, and four of them showed a stable fracture union without complications. Two cases with severe osteoporosis were successfully treated by cortical strut onlay allograft, while the other two with normal range of BMD could be treated without allograft.
The limitations of this study need to be acknowledged in the interpretation of findings for practice. First, this study was a not randomized and chronological study with separate cohorts obtained with change in practice. There was no power calculation to guide sample size related to the retrospective study with a relatively small sample size. Although there was a relatively small number of patients, the follow-up period was sufficient to detect delayed union or reduction loss in the investigated cases, and our findings highlighting risk factors in the treatment of PFFs using the cable-plate construct can suggest important clinical implications. Second, osteoporosis could be important risk factor for affecting prognosis after fixating plate. The distribution of patient's age was between 42 to 86 years in this study. Although BMD in four patients less than 60 years of age could not measured, it was thought that bone quality of young age (less than 60 years) might be good. Third, there was no analysis related to the effect of cortical strut onlay allograft as an additional procedure, which can be a prognostic factors in the treatment of PFFs. Therefore, further prospective studies with larger numbers and another surgical procedures are also required to investigate the clinical outcomes of patients treated with osteosynthesis for the Vancouver type B1 PFFs around or just distal to a well-fixed femoral stem.
Go to :
 XML Download
XML Download