

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Periprosthetic joint infection (PJI) after total hip arthroplasty (THA) is an infrequent but devastating complication, with an incidence of 0.3% to 2% following primary hip arthroplasty12) and the rate seems to have increased over recent years3). Besides the impact on patient health, PJI is costly for the health system4). Debridement, antibiotics and implant retention (DAIR) is considered an attractive option for treating acute and hematogenous infections to minimize costs and morbidity of prosthesis exchange assuming that a biofilm is not yet established on the prosthesis surface. Importantly, however, the success of this procedure varies widely, with reported infection control rates from 26% to 91%56789101112131415161718).
Knowledge of factors associated with success or failure of DAIR in early infections could help guide the decision-making process when facing a periprosthetic infection. The main known predictive factors are related to the causative organism101920), symptom duration8101215), and patient comorbidities58).
The aims of this study were to i) determine the rate of success of DAIR in acute and hematogenous PJI after THA, ii) identify possible outcome predictors, and iii) analyze the clinical and radiological outcomes.
Go to : 
MATERIALS AND METHODS
We performed a retrospective cohort study of all patients diagnosed with acute postoperative or hematogenous infection after THA who underwent irrigation and debridement with prosthesis retention at a tertiary teaching hospital (Hospital Galdakao-Usansolo; Galdakao, Spain) between 2004 and 2015. Patient consent and approval from the institutional review board (No. 31/16) were obtained.
Infections were diagnosed based on Musculoskeletal Infection Society (MSIS) criteria21). When infection was suspected from clinical presentation (e.g., based on persistent wound drainage, erythema, pain, and fever), C-reactive protein (CRP) and erythrocyte sedimentation rate were assessed, and the joint was aspirated under sterile conditions for synovial fluid examination and culture.
Criteria for DAIR included postoperative acute infections diagnosed within three months of arthroplasty, and hematogenous infections characterized by an acute onset of symptoms, in previously well-functioning hip arthroplasty. Patients were excluded if either the cup or the stem were removed during surgery or when previous treatment other than DAIR had been carried out. Chronic periprosthetic infections were treated with one- or two-stage revisions depending on the conditions of the soft tissue, microorganism susceptibility, and patients' general status.
A successful outcome was defined as the absence of clinical infection, normal inflammatory markers and prosthesis retention without radiological signs of infection after a minimum follow-up of 12 months. We defined failure as the need to remove the prosthesis or to administer chronic antibiotic treatment as well as infection-related death. A second debridement was not considered a failure. Subsequent DAIR was decided upon by the treating surgeon based on patients' health status or clinical recurrence.
Medical records of patients were reviewed and demographic characteristics and concurrent comorbidity status were collected. Several variables were analyzed to evaluate their potential influence on outcomes: age, sex, body mass index, American Society of Anesthesiologists physical status classification system (ASA) score, Charlson comorbidity index (CCI)22), age-adjusted Charlson comorbidity index (ACCI)23), KLIC (Kidney failure, Liver cirrhosis, Index surgery, Cemented prosthesis, and C-reactive protein) score24), comorbidities, surgical indication (primary, revision surgery or femoral neck fracture), infection type (acute or hematogenous), duration of symptoms, age of prosthesis, CRP level (mg/L), cemented or non-cemented arthroplasty, mobile parts exchange, use of gentamycin sponges, use of antibiotic before DAIR, surgeon experience (general orthopedic surgeon or hip surgeon) and type of microorganism. Postoperative complications were studied.
All operations were performed at our institution by one of several surgeons with distinct levels of experience in hip arthroplasty. The decision of which surgeon carried out surgery was made based on staff availability. We investigated whether outcomes were associated with the experience of the surgeon, by classifying surgeons as general orthopedic surgeons (<25 THA/yr) or hip arthroplasty surgeons from the hip unit (>50 THA/yr)25). Hip and general orthopedic surgeons operated on six (23.1%) and 20 cases (76.9%), respectively. The previous incision was used in all cases. Surgery included thorough debridement and removal of necrotic tissue, radical synovectomy, copious irrigation with saline (9–12 L), and collection of at least five tissue samples. The decision to exchange or retain mobile parts was made by the treating surgeon; their replacement occurred in six cases (23.1%). Prostheses were confirmed to be stable and a drain was inserted in all cases. Empirical intravenous antibiotic therapy was initiated after taking intraoperative samples and adjusted in accordance with the recommendations of the institution's infectious disease service when causative organisms were identified and sensitivities determined. The protocol recommended two weeks of intravenous treatment followed by oral therapy with priority given to biofilm-active antibiotics (e.g., rifampicin and/or fluoroquinolones). The preferred duration of oral antibiotics was four to eight weeks, although it varied in some cases based on clinical evolution. Patients were referred for clinical and radiological assessment at four weeks, three and six months, one year, and every one to two years thereafter. The minimum follow-up period was 12 months.
In the study period, 30 hips (29 patients) with an early or hematogenous infection were treated with DAIR. Four cases were excluded from the study, given that the implant was found to be loose and removed (one cup, three stems). The remaining 26 hips (25 patients) were included in the analysis. The cohort consisted of 15 males (one bilateral case) and 10 females, with a mean age of 72.5 years (range, 52–85 years). The infections were acute postoperative in 16 cases (61.5%) and hematogenous in 10 (38.5%), and occurred after primary THA in 16 hips (61.5%) and after revision THA in 10 (38.5%). All revision surgeries were due to aseptic loosening and intraoperative cultures were found to be negative. The main indication for surgery was osteoarthritis (n=15), acute femoral neck fracture (n=5), developmental hip dysplasia (n=3), avascular necrosis (n=2), and rheumatoid arthritis (n=1). The most common type of implant fixation was cementless (n=18), followed by hybrid (n=6) and cemented (n=2). Using ASA score, five patients were classified as class II, 16 as class III, and five as class IV. The mean CCI score was 2.35 (range, 1–5) and the mean ACCI 5.2 (range, 2–8). The primary procedure had been performed at our institution in 22 cases and elsewhere in four. The most frequently isolated microorganism was Staphylococcus aureus (6 hips; 23.1%).
The mean follow-up was 48.5 months (range, 12–144 months). The median time between index procedure and DAIR was 23.5 days (range, 11–70 days) in acute postoperative infections and 24 months (range, 1.2–204 months) in hematogenous infections. The median duration of symptoms was 14 days (range, 1–59 days). The mean duration of postoperative antibiotic treatment was 2.5 weeks for intravenous antibiotics (range, 0.5–8 weeks) and 5.5 weeks for oral antibiotics (range, 1–8 weeks).
The clinical outcome was assessed using a visual analogue scale (VAS) to rate pain, from 0 (no pain) to 10 (worst pain); patient mobility based on the ability to walk; and the Harris Hip Score (HHS) with a maximum score of 100 points. The results were compared with preoperative functional assessment before index arthroplasty (excluding fractures). Radiological assessment was based on anteroposterior radiographs and axial radiographs of the affected hip obtained in order to detect any acetabular or femoral radiolucency and/or osteolysis. Acetabular radiolucencies were classified according to DeLee and Charnley26) and femoral radiolucencies according to Gruen et al27). Any implant migration, subsidence or cortical hypertrophy was recorded.
1. Statistical Analysis
A descriptive analysis of patient characteristics was carried out to characterize the study population, calculating frequencies and percentages for categorical data, and means, standard deviations, maximum, minimum and percentiles values for continuous variables. Univariate analysis was performed in the sample to identify risk factors, using chisquare or Fisher's exact test and Student's t-test or the nonparametric Wilcoxon test for categorical and continuous variables, respectively. All effects were considered significant at P<0.05. All statistical analyses were performed using SAS® ver. 9.4 (SAS Institute Inc., Cary, NC, USA).
Go to :
RESULTS
At the last follow-up, of the 26 infected hips, seven were free of infection (26.9%). The outcome was successful in 31.2% of the early postoperative infections and 20.0% in the hematogenous infections. One patient with bacteremia and sepsis required a second debridement to control the infection. Patients in whom the DAIR treatment failed required one-stage exchange (n=1), two-stage exchange (n=10), and suppressive antibiotic therapy (n=8).
Among the comorbidity variables studied (Table 1), male sex was identified as a predictor of failure (P=0.005), and debridement performed by a surgeon from the hip unit as a predictor of treatment success (P=0.028). Eradication of infection was achieved in 66.6% of cases operated by hip surgeons, compared to 15.0% of patients operated by general orthopedic surgeons. Increased DAIR failure was observed in patients with chronic pulmonary disease and steroid therapy (P=0.059 and 0.062, respectively). Success rates were higher among those with lower ACCI scores (≤5; 40.0%) compared with those with higher scores (>5; 12.0%) (P=0.178). The KLIC score was higher in the treatment failure group (P=0.078).
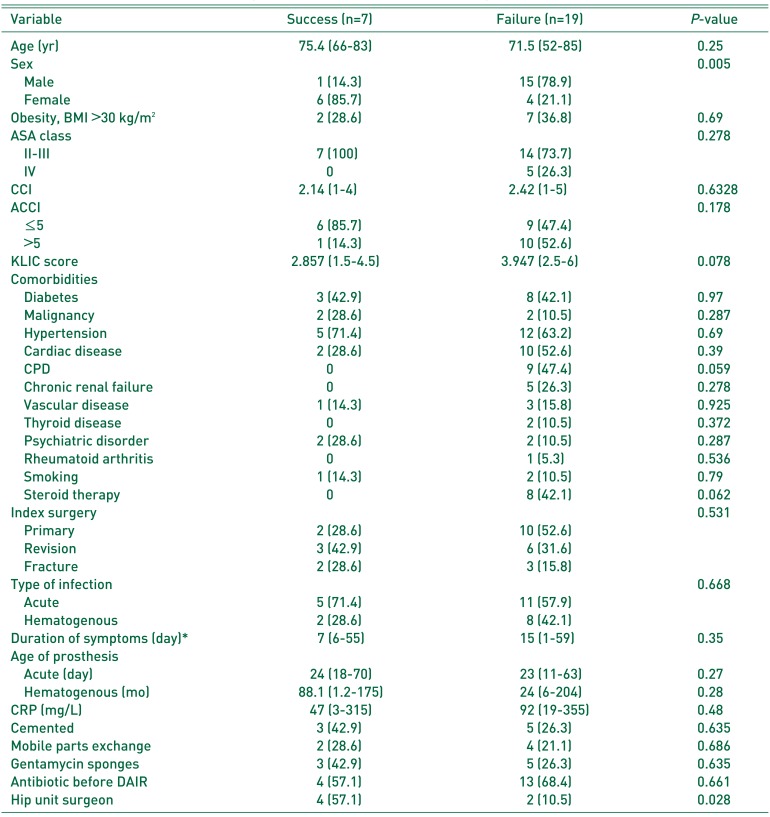
Table 1
Patient Characteristics and Surgical Details of Study Cohort according to Outcome
Values are presented as mean (range), number (%), or *median (range).
BMI: body mass index, ASA: American Society of Anesthesiologists physical status classification system, CCI: Charlson comorbidity index, ACCI: age-adjusted Charlson comorbidity index, KLIC: Kidney failure, Liver cirrhosis, Index surgery, Cemented prosthesis, and C-reactive protein, CPD: chronic pulmonary disease, CRP: C-reactive protein, DAIR: debridement, antibiotics and implant retention.
![]()
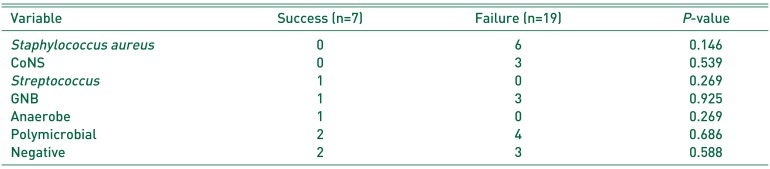
Regarding time from onset of symptoms to debridement, 11 days was a significant cut-off point for success in the hematogenous group (P=0.015). Considering both groups, debridement within the first 11 days of symptoms had a success rate of 45% (P=0.068). There was no significant difference in success rate between DAIR performed more or less than 30 days from the index procedure in the early postoperative group. Considering the causative pathogen, the treatment failed in all six cases caused by S. aureus (P=0.146) (Table 2).
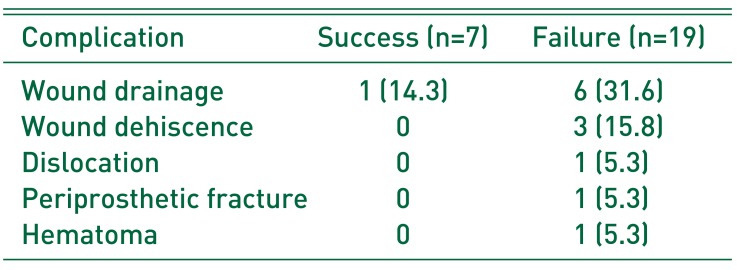
Overall, 13 local complications (50.0%) developed after debridement (Table 3). In the success group, there was only one case of wound drainage that healed after a second debridement. Seven patients died during follow-up; only one of these deaths was related to the infection.
Nineteen hips underwent a complete clinical assessment at the last follow-up. Mean pain VAS score was 1.58 (range, 0–8) and mean HHS was 74.2 (range, 36–95). Regarding mobility, 26.3% of patients were able to walk without help, 57.9% with a stick, and 10.5% with frame/crutches, while 5.3% were not able to walk. Significant improvement was seen in VAS and HHS scores from baseline in patients with pre- and postoperative assessment (P=0.0002 and 0.0018, respectively).
The mean HHS in the success group (n=7) was lower; 71.7 (range, 49–89) vs. 75.7 (range, 36–95) in the failure group (n=12). Patients that underwent a two-stage exchange (n=7) had a mean HHS of 82.3 (range, 64–94), while patients with chronic antibiotic treatment (n=5) had a mean HHS of 66.4 (range, 36–95).
Thirteen cases with the original implant were analyzed for radiographic assessment. Three cases showed osteolysis (one acetabular and two femoral) that was present prior to the debridement due to aseptic loosening. Only one patient showed radiological loosening due to the infection.
Go to :
DISCUSSION
The present study shows high failure rates when using DAIR for the treatment of early postoperative and hematogenous periprosthetic infections of the hip. Published rates of success with DAIR for infection of hip arthroplasty vary greatly between studies, probably due to differences in selection criteria (often including hip and knee arthroplasties), treatment protocols, follow-up, and causative organisms. Moreover, some published reports include several joints20) and other multiple debridement to control the infection5192829). In some studies, the success rate improved with repeated debridement. Grammatopoulos et al.12) reported an infection eradication rate of 68% with a single DAIR that improved to 85% with a second debridement in 20 cases. In our study, we only performed a second debridement in one case. The success rate was lower for hematogenous infections (20.0%) than for acute postoperative infections (31.2%). This is in accordance with other published series8) recognizing that it can be difficult to differentiate a hematogenous infection from a chronic infection.
Patient comorbidities have been described as a predictor of treatment failure. Azzam et al.5) observed that patients with ASA class 3 or 4 were more likely to fail and suggested DAIR should be limited to healthy patients. Fink et al.8) identified higher ASA class and smoking as independent risk factors associated with infection recurrence. Obesity has also been linked to poorer results15). We note increased DAIR failure related to chronic pulmonary disease (P=0.059) and steroid therapy (P=0.062). The level of comorbidity in our cohort was higher than in most previous studies81213152830) (Table 4). Previous studies have often used different scores to define patients' coexisting medical conditions. The CCI is the most widely used method to quantify the overall burden of comorbidities, being modified later by the inclusion of age as one additional item (ACCI).
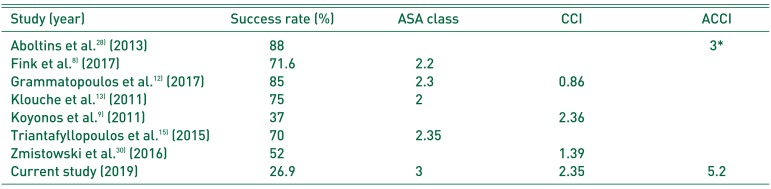
Table 4
Studies Reporting Comorbidity Index of Patients
| Study (year) | Success rate (%) | ASA class | CCI | ACCI |
|---|---|---|---|---|
| Aboltins et al.28) (2013) | 88 | 3* | ||
| Fink et al.8) (2017) | 71.6 | 2.2 | ||
| Grammatopoulos et al.12) (2017) | 85 | 2.3 | 0.86 | |
| Klouche et al.13) (2011) | 75 | 2 | ||
| Koyonos et al.9) (2011) | 37 | 2.36 | ||
| Triantafyllopoulos et al.15) (2015) | 70 | 2.35 | ||
| Zmistowski et al.30) (2016) | 52 | 1.39 | ||
| Current study (2019) | 26.9 | 3 | 2.35 | 5.2 |
![]()
Most recent studies report excellent outcomes when treatment occurred at experienced centres with specific units to treat orthopedic infections1218). There are few studies comparing the results as a function of surgeon experience. Bergkvist et al.29) classified participating surgeons as very experienced, moderately experienced and inexperienced in arthroplasty, but did not observe any differences between these groups. In our department, several surgeons carried out DAIR procedures with different amounts of experience in hip surgery. Debridement being performed by hip surgeons, rather than general orthopedic surgeons, was found to be a significant predictor of success. This is the first published study, to our knowledge, revealing differences in DAIR outcome as a function of the experience of the treating surgeon. We believe debridement could have been more meticulous when experienced hip surgeons performed it due to a better understanding of the field and management of possible complications. We think that the high percentage of general orthopedic surgeons (77%) between participating surgeons could be a reason of the low success rate of DAIR in our study and we recommend specialized hip arthroplasty surgeons should perform this procedure.
Duration of symptoms until DAIR is a well-studied factor influencing infection eradication. Previous reports have a related length of symptoms from two to eight days with treatment success8101215). In our study, we obtained significantly more favorable results when symptoms were present for fewer than 11 days in the case of hematogenous infections; however, the difference was not significant for the whole cohort. Another variable that may affect outcomes is the infecting pathogen. We did not observe any significant differences in treatment success by organism isolated, probably due to the small cohort, although the treatment failed in all cases infected by S. aureus, which have been correlated with worse prognosis101920).
There are few studies evaluating functional outcome after DAIR1213161728) and our results are similar to those series. The mean postoperative HHS was 74.2 points in our study. Tsukayama et al.16) reported a mean HHS of 70 points in early postoperative infections and 75 in acute hematogenous infections. Westberg et al.17) obtained a median HHS of 79 points in their series; in the group successfully treated the median HHS was 86 points, while in the treatment failure group the HHS was 66. In contrast, we note a better HHS in the failure group (75.7) than the success group (71.7). This can be explained by the fact that those who underwent two-stage revision obtained better HHS (82.3). The complication rate in our series was high (50.0%). Similar complication rates have been described in previous studies1217).
We recognize some limitations of this study. First, it is based on a retrospectively studied cohort, with a small number of patients, and the findings would have been stronger with a larger sample. Second, several surgeons performed the debridement and the surgical procedure might have differed. Third, the follow-up was relatively short. Fourth, it was difficult to identify an obvious source of infection in all hematogenous infections and some of them might be low virulence chronic infections that remained asymptomatic for a long time.
Go to :
CONCLUSION
We report a high failure rate of DAIR in a population with a high comorbidity index. Two-stage revision should be considered in patients with poor medical conditions. In our series, surgery being performed by a hip specialist was predictive of infection eradication, while outcomes were negatively associated with chronic pulmonary disease and steroid therapy. Further, outcomes were better if the surgery was undertaken shortly after the onset of symptoms (i.e., fewer than 11 days). The limitations of this technique must be considered for decision-making and we recommend experienced hip arthroplasty surgeons should carry it out.
Go to :
 XML Download
XML Download