

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Venous thromboembolism (VTE) is a common complication after major orthopedic surgery and can lead to pulmonary embolism (PE), deep vein thrombosis (DVT) and sudden death1). According to recently published data, the rates of VTE (11.3–76.5%) and PE (1.4%) in Asian populations are increasing at almost the same rate as that reported in the West after joint arthroplasty234). According to the corresponding author's previous study5) on the prevalence and risk factors of VTE after joint arthroplasty in an Asian cohort not administered prophylaxis, the prevalence of VTE in Asians is lower than in Caucasians. Nevertheless, there is still need for chemical thromboprophylaxis6).
In the past, heparin-based or acetylsalicylic acid thromboprophylaxis was used to reduce the incidences of VTE and fatal PE78). However, adverse outcomes (e.g., on-treatment bleeding), were a concern for extended prophylaxis9). Recently, chemical prophylaxis with the oral factor Xa inhibitor, rivaroxaban (RXB), was introduced as an easier, safer option to prevent the risk of bleeding10). Factor Xa functions at the point of convergence between the extrinsic and intrinsic pathways of the coagulation cascade and combines with factor Va to activate thrombin, which cleaves fibrinogen to fibrin and results in clot formation. Therefore, the aim of the present study was to determine the potential benefit of oral chemical thromboprophylactic agent (RXB) by comparing the prevalence of VTE in Korean patients administered or not administered RXB for prophylaxis following arthroplasty.
Go to : 
MATERIALS AND METHODS
1. Patients and Study Design
Informed consent was obtained from all the individuals participating in the study. The study was proactively approved and monitored by Inha University Hospital Institutional Review Board (No. INHAUH 2019-05-007). This prospective study was conducted in 2,603 patients (males: 948; females: 1,655), who underwent hip or knee arthroplasties including bilateral arthroplasties or revision surgery at Inha University Hospital. The mean age of study participants at the time of surgery was 68.2 years (range, 29–98 years), and mean height, weight, and body mass index (BMI) were 157.8 cm, 59.1 kg, and 23.2 kg/m2, respectively. Mean follow-up was 46.5 days (range, 37–48 days) after surgery. All operations were performed by a single arthroplasty specialist (MKH), and spinal, epidural alone, or an epidural with general anesthesia was employed. No definitive exclusion criteria were applied. If a patient was using a thrombolytic agent for any reason, we stopped the drug for 5 to 7 days before surgery after consulting doctors from associated departments. The original drug was re-prescribed after RXB discontinuation. Our before-and-after study design was conducted by collecting data prospectively based on RXB administration since January 2010. The 1,608 patients who underwent surgery before January 2010 did not receive oral chemical prophylaxis after surgery, whereas 995 patients who underwent surgery after January 2010 were administered oral RXB. Demographics of the 2,603 study subjects are presented in Table 1.
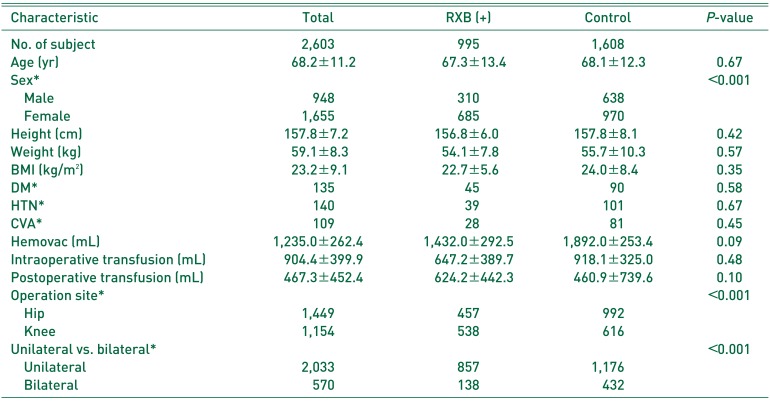
Table 1
Demographic Characteristics in the RXB and Control Groups
![]()
All 2,603 patients underwent a preoperative Doppler ultrasonography on both legs to ensure they were free of VTE. When VTE occurred, the patient had to wait until it had been completely removed by thrombolytic agents before arthroplasty was performed. A compression stocking was applied for 6 weeks after surgery. Patients that underwent primary hip arthroplasty were allowed joint motion exercise, weight-bearing and ambulation restricted adduction and internal rotation of the hip joint after hemovac removal. Discharge was scheduled two weeks after surgery. Patients that underwent primary knee arthroplasty were allowed continuous passive motion exercise, weight-bearing and ambulation after hemovac removal, and patients that underwent revision hip arthroplasty were allowed joint motion exercise in bed for 6 weeks postoperatively, and then allowed ambulation. Discharge was scheduled for 6 weeks postoperatively for revision arthroplasty patients.
A hemovac was inserted into every operative wound. Amounts of hemovac drainage were checked daily in the morning. In patients receiving primary hip or knee arthroplasty, hemovacs were removed if the daily amount of blood drainage was less than 100 mL, and in revision hip or knee arthroplasty patients, hemovacs were removed if daily drainage was less than 50 mL. Time elapsed after surgery was not considered when deciding on hemovac removal. Patients that underwent surgery after January 2010 received oral RXB (Xarelto®; Bayer HealthCare AG, Wuppertal, Germany) 10 mg once daily from the day after hemovac drainage removal to postoperative day (POD) 14. For example, if a hemovac was removed on POD 3, oral RXB was administered on the mornings of POD 4 to 14. The dosage of RXB used was based on the results of a global study11). This postoperative protocol was used continuously from 2010 to 2017.
2. Diagnosis
Doppler ultrasonography of both legs was performed in an outpatient department 6 weeks after surgery on all patients that underwent elective primary arthroplasty and on all revision arthroplasty patients during hospitalization. The presence of VTE was evaluated under radiologist supervision. If any suspicious findings were observed, angiographic computed tomography (CT) was used to confirm VTE location. During admission, if any tenderness or swelling suspicious of DVT occurred in a lower extremity, angiographic CT and PE CT were performed routinely for the diagnosis of VTE or asymptomtic PE. When sudden chest pain, tachycardia, dyspnea, or a mental change occurred after surgery, blood laboratory tests, including D-dimer and angiographic and PE CT were performed under suspicion of symptomtic PE. Locations of thrombi were classified as ipsilateral or contralateral. Distal thrombi (below the knee joint) included the posterior tibial vein, anterior tibial vein, and fibular vein, and proximal thrombi included the iliac vein, femoral vein, and popliteal vein.
3. Perioperative Factors
In a previous study conducted by the corresponding author on the prevalence and risk factors of VTE in an Asian cohort after joint arthroplasty, female sex, the need for revision surgery, a simultaneous bilateral procedure, a cerebrovascular accident (CVA), and a high preoperative platelet (PLT) count were considered risk factors of VTE5). In the present study, hematologic factors (e.g., hemoglobin [Hb] level, hematocrit, platelet count, albumin, prothrombin time, activated partial thromboplastin time) were noted before surgery, immediately after surgery, and on POD 1, 2, and 3. Medical histories including hypertension, diabetes mellitus, smoking history, history of CVA (only thromboembolic stroke not hemorrhagic stroke or malignancy) and weight, height, BMI, anesthesia and operation records (including operation time), and intraoperative blood loss were analyzed. Postoperative blood loss (hemovac volumes) and transfusion requirements during and after surgery were also analyzed.
Transfusions were used based only on Hb levels. If Hb levels were <9 g/dL, packed red blood cells were transfused to increase Hb to >9 g/dL. Hb levels were checked daily when a hemovac was inserted. After hemovac removal, Hb levels were checked twice weekly until POD 14 and then weeks until 6 weeks after surgery if hospitalized.
4. Outcomes
Outcomes were defined as the presence of thrombi anywhere (proximal or distal including symptomatic or asymptomatic DVT or PE) and death during follow-up (6 weeks after surgery). Efficacy of oral chemical thromboprophylaxis was assessed by comparing outcomes in the RXB and non-prophylactic groups. The safety outcomes included incidences of on-treatment bleeding events beginning after taking RXB until 2 days after last intake on POD 16. On-treatment bleeding was defined as: 1) major bleeding (i.e., bleeding that was fatal or which occurred in a critical organ), 2) the bleeding requiring re-operation, 3) nonsurgical site bleeding, which may have been associated with a fall in the Hb level of at least 2 g/dL or which may have required transfusion of 2 or more units of whole blood or packed cells, or 4) hemorrhagic wound complications (e.g., persistent wound discharge or infection not severe enough to require re-operation).
5. Statistical Analysis
Continuous variables are expressed as means±standard deviations and discrete variables as frequencies and percentages. Independent sample t-tests were applied to evaluate differences between group means. The chi-square test, Fisher's exact test or Mann-Whitney U-test were used to compare continuous variables. Statistical significance was accepted for P-values <0.05. Binary logistic regression analysis was performed to evaluate the efficacy of oral chemical thromboprophylaxis (RXB), and multiple logistic regression analysis was used to identify independent predictors of VTE and PE. Variables with P-values of <0.05 by univariate analysis were included in the model. Model fit was evaluated using the Hosmer-Lemoshow goodness-of-fit test; two-tailed P-values of <0.05 were considered statistically significant. The statistical analysis was performed using SPSS ver. 13.0 (SPSS Inc., Chicago, IL, USA).
Go to :
RESULTS
The RXB group and the non-prophylactic (control) group were compared with respect to age, sex, and percentages of hip/knee and bilateral arthroplasties. Results are summarized in Table 2. Univariate analysis showed sex, operation site, and procedure laterality (unilateral vs. bilateral) were significantly associated with VTE incidences, and these variables remained significantly after adjusting for confounders (Table 3).

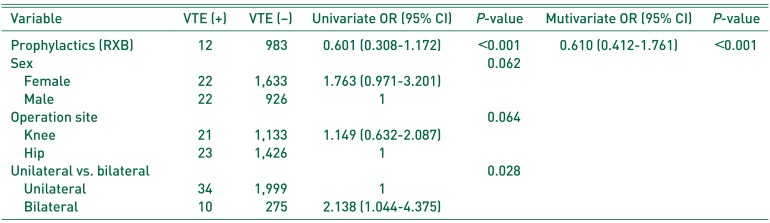
Table 2
Labaratory Findings in the RXB and Control Groups
![]()
Table 3
Risk Factors of VTE as Determined by Univariate and Multivariate Analysis
![]()
1. Incidence of Venous Thromboembolism
Forty-four of the 2,603 study subjects were diagnosed with VTE before POD; 12 patients in the RXB group and 32 patients in the control group were diagnosed with VTE. In the RXB group, VTE developed after arthroplasty in 12 patients (1.21%) and 2 patients (0.38%) developed PE. In the control group, VTE developed after arthroplasty in 32 patients (1.99%), and four patients (0.24%) developed PE. The odds ratio (OR) of VTE or PE were 0.61 (P=0.013) and 1.58 (P=0.320), respectively.
Of the 44 patients that developed DVT, 18 patients presented with lower limb tenderness and swelling. Twelve patients had discomfort before discharge. Thirty patients were diagnosed within 2 weeks of surgery, and the other 14 patients were diagnosed at routine follow-up by Doppler ultrasonography at 6 weeks after surgery. Among the 44 people diagnosed with DVT, proximal and distal thrombi were present in 18 patients (0.40%) and 24 patients (0.61%), respectively. The remaining 2 patients showed both distal and proximal VTE. Proximal thrombi were present in 8 of 20 patients (40.0%) that underwent hip arthroplasty, whereas the remaining 12 patients (60.0%) developed distal DVT. The 4 knee arthroplasty group developed distal and proximal DVT. In all 44 patients DVT developed ipsilaterally. Two out of the 6 patients who developed PE and who showed positive Doppler ultrasonography of the lower leg were treated with heparin and antithrombotic agents without inserting an inferior vena cava (IVC) filter; the remaining 4 patients were treated with heparin and oral antithrombotic agents with a preventative IVC filter. All study subjects underwent postoperative Doppler ultrasonography at 6 weeks after surgery. Preoperative Doppler ultrasonography could not to be performed on 231 of the study subjects; all were fracture patients hospitalized via our emergency department during weekends and who underwent surgery on Mondays. Ten of the study subjects showed evidence of previous DVT prior to surgery and were treated with anticoagulants before operation. These anticoagulants were stopped 5 to 7 days before surgery after confirming no DVT by preoperative Doppler ultrasonography.
2. Incidence of Venous Thromboembolism according to Operation Site and Surgical Procedure
Twenty-two of the 1,449 patients (1.51%) who underwent hip arthroplasty developed DVT, whereas twenty-two of 1,132 (1.94%) who underwent knee arthroplasty patients developed DVT. The incidence of DVT was significantly higher in the knee arthroplasty patients compared with the hip arthroplasty patients (OR, 1.17; P=0.001). Ten of the 385 patients (2.59%) who underwent a bilateral simultaneous operation developed VTE. Of the 2,033 patients who underwent unilateral arthroplasty, 34 patients (1.67%) developed DVT. In addition, the incidence of DVT in those who underwent a bilateral simultaneous operation was significantly higher than in unilateral arthroplasty patients (OR, 1.57; P=0.036).
The incidence of DVT among unilateral arthroplasty patients tended to be lower compared with those who received RXB prophylaxis (OR, 0.66; P=0.270), and similarly, for hip arthroplasty patients (OR, 0.35; P=0.376) and for knee arthroplasty patients (OR, 0.41; P=0.191) also tended to be lower for those administered RXB. Table 4 summarizes the incidences of DVT in the RXB and controls groups by surgical methods. VTE after revision arthroplasty developed in 10 of 408 patients (2.45%), that is, the relative risk (RR) was 1.58 times higher than in the primary arthroplasty group (1.54%). Patients that underwent revision hip arthroplasty (2.14%; P=0.043) had a 1.50 times higher RR than those that underwent primary hip arthroplasty (1.43%), and those who underwent revision knee arthroplasty (3.65%; P=0.037) had a 2.18 times higher OR than those who underwent primary knee arthroplasty (1.68%) (Table 4).

3. Operation Time and Blood Loss
Mean operation time was 172 minutes (55–420 minutes). Mean operation times were 107 minutes (primary hip arthroplasty), 140 minutes (primary knee arthroplasty), 167 minutes (revision hip arthroplasty) and 182 minutes (revision knee arthroplasty). Bilateral simultaneous procedures had a mean operation time of 301 minutes. The mean intra-operative blood loss in total case was 708 mL (range, 100–2,500 mL). Mean estimated blood loss was 583 mL (primary hip arthroplasty), 710 mL (primary knee arthroplasty) 734 mL (revision hip arthroplasty), 704 mL (revision knee arthroplasty), and 1,172 mL (simultaneous bilateral procedures). Mean intra-operative blood loss was 1,157 mL (patients with VTE), higher than that for non-VTE patients (mean, 636 mL) (P=0.09). Mean hemovac drainage amount in total case after surgery was 1,235 mL (range, 370–4,890 mL). Mean postoperative hemovac drainage in the RXB group was 1,432 mL, compared with 1,892 mL in the control group. Postoperative hemovac drainage in patients that developed VTE was 2,086 mL compared with 1,198 mL in those that did not develop VTE.
4. Venous Thromboembolism Risk Factors and Incidence
As mentioned above, in a previous study the corresponding author found that female sex, revision surgery, a bilateral simultaneous procedure, a CVA, and a high preoperative PLT counts were risk factors of VTE in patients that did not receive prophylaxis.
In our study, 12 VTE patients were administered RXB (9 females and 3 males). Of the 685 female patients in the RXB group, 9 (1.31%) developed VTE, whereas of the 310 male in the RXB group, 3 (0.96%) developed VTE. In the control group, VTE developed in 32 patients (24 females and 8 males). Of the 970 female controls, 24 (2.47%) developed VTE, and of the 638 male controls, 8 (1.25%) developed VTE. No CVA episode occurred among the 7 patients that developed VTE and the mean preoperative PLT level for these patients was 250,700/µL. No significant difference was found between the preoperative PLT levels of patients that developed or did not develop VTE (201,300/µL).
5. On-treatment Bleeding
As previously mentioned, on-treatment bleeding was defined as: 1) major bleeding (i.e., bleeding that was fatal or occurred in a critical organ), 2) bleeding requiring re-operation, 3) nonsurgical site bleeding, which may have associated with a fall in the Hb level of at least 2 g/dL or which may have required transfusion of 2 or more units of whole blood or packed cells, or 4) hemorrhagic wound complications (e.g., persistent wound discharge or infection not severe enough to require re-operation). In our study, no reoperation due to bleeding was required and no hemorrhagic wound complications (e.g., continuous oozing or infection occurring before POD 14), however, three cases of nonsurgical site bleeding occurred, upper gastrointestinal bleeding (n=1) and retroperitoneal hemorrhages (n=2). In these three cases of nonsurgical site bleeding, RXB was discontinued on the day on-treatment bleeding was detected.
Of the 2,603 study subjects, 1,965 received a transfusion during or after surgery. Investigations were conducted to determine the causes of reduced Hb levels, but no definite cause (e.g., gastrointestinal bleeding, other bleeding) were observed. In all cases, Hb levels were maintained in the normal range after transfusion. Three patients older than mean study subjects age exhibited diminished general performance (e.g., poor oral intake), after surgery. We concluded diminished Hb was temporary and not influenced by RXB.
Go to :
DISCUSSION
VTE is a potentially fatal complication of hip or knee arthroplasty. The mechanical methods for VTE prophylaxis after hip and knee arthroplasties include mobilization, compression stockings, intermittent pneumatic compression device. In chemical methods for VTE prophylaxis, subcutaneous low-molecular weight heparin (LMWH) has been used for thromboprophylaxis, though other oral chemical agents, such as aspirin are also used. LMWH is applied subcutaneously, and thus, compliance might be an issue as compared with simple oral chemical methods12). Other oral chemical agents (e.g., dabigatran etexilate [a new direct thrombin inhibitor]) are also available, however, Wolowacz et al.13) reported this agent is not superior to other known oral chemical agents, especially when it is administered alone to patients. More recently, NOACs (new oral anticoagulants) have been shown to be effective for thromboprophylaxis after total hip arthroplasty (THA) and total knee arthroplasty in randomized controlled trials. Other studies have reported that prophylaxis with RXB for 2 weeks further reduces the risk of VTE following hip or knee arthroplasty14). The use of RXB is safe, without a statistically significant increase in severe hemorrhage or any bleeding15). In the present study, VTE occurred in 5 of 457 patients (1.09%) administered RXB after hip surgery and in 7 of 538 (1.30%) after knee surgery, which have a decisive effect on more nonspecific lower-extremity symptoms after knee surgery. Kim16) recommended that all patients undergoing THA are assessed preoperatively for risk of VTE and bleeding to choose appropriate VTE prophylaxis. Also, all patients are recommended to ambulate as early as possible postoperatively to reduce the risk of VTE. Vague and uncertain discomfort in lower legs after knee surgery tend to be evaluated more rigorously after knee surgery than after hip surgery17), though those that undergo knee arthroplasty may be more susceptible to VTE after surgery due to tourniquet application during surgery18). In fact, 44 patients diagnosed with VTE within 6 weeks of surgery all underwent knee or hip surgery. Furthermore, the incidence of VTE was reduced by RXB thromboprophylaxis. However, the incidence of PE was higher in the RXB group compared with controls, which we attribute to statistical underpowering due to the relatively small numbers. Furthermore, the RXB group contained a higher proportion of females, simultaneous bilateral procedures, and knee arthroplasties compared with the control group. Patients in the RXB group could have a lower risk to a VTE after surgery. In addition, demographics were significantly different among the 2 study groups, and thus, we adjusted the multivariate analysis for confounders, such as, sex, operation site, and unilateral versus bilateral procedure. We would expect that a larger-scale study would reveal a lower incidence of PE after RXB prophylaxis. Kakkar et al.10) recommended the use of RXB for more than 5 weeks after surgery, however, the present study indicates RXB usage until POD 14 is sufficient. As VTE mainly occurs at around POD 5 and is uncommon after POD 141920), the use of RXB after POD 14 appears to have little advantage. Furthermore, cost or bleeding problems may arise as a result of RXB overuse. In the present study, we used a compressive stocking until 6 week after surgery, and this might have been enough to prevent post-hospitalization VTE in primary arthroplasty patients. This study is meaningful as it includes hip and knee arthroplasty and simultaneous bilateral procedures. Other articles on the topic have focused on thromboprophylaxis after hip joint arthroplasty921), and the results obtained for thromboprophylaxis in knee arthroplasty patients in the present study support previous results.
Regarding limitations of the present study, we evaluated patients until 6 weeks after surgery, and thus, VTEs that occurred later were not considered. However, VTEs after 6 weeks postoperatively are uncommon. In addition, we included 2,603 patients in our analysis, a sample size which resulted in inadequate statistical power (0.313), but to have achieved a statistical power of >0.6, more than 20,000 patients were needed, which precluded the recruitment of cases treated by one surgeon at one hospital. Nevertheless, the study did reveal a decreasing tendency of VTE development after RXB use. Further multicenter studies are required to increase sample size. The diagnostic accuracy of ultrasonography for detecting DVT also varies according to the technique used. In general, optimal sensitivity for DVT is achieved by using duplex (proximal sensitivity 96%, distal sensitivity 71%, specificity 94%) or triplex ultrasound (proximal sensitivity 96%, distal sensitivity 75%, specificity 94%)22). Lastly, our uncontrolled before-and-after study (i.e., conducted before and after the introduction of an intervention) and observed differences in performance are assumed to be due to the intervention. Generally, uncontrolled before-and-after studies should not be used to evaluate the effects of quality improvement interventions and the results of studies using such designs have to be interpreted with great caution23).
Go to :
CONCLUSION
RXB thromboprophylaxis showed a tendency to decrease the incidence of VTE after knee or hip arthroplasty in a Korean population. Because no serious complications were encountered after the administration of oral RXB, and considering its convenience as compared with other agents, we suggest it be considered for oral chemical thromboprophylaxis in Korean arthroplasty patients. However, a multi-center study is required to improve statistical power.
Go to :
 XML Download
XML Download