

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Hip fractures are increasing in frequency, due in large part to a rapidly aging population12). Intertrochanteric fractures in the elderly are mostly osteoporotic fractures in a form of a comminuted fracture in which the bone has broken into 3–4 fragments in 30–40% and unstable intertrochanteric fractures that affect to the posteromedial cortex34). Hemiarthroplasty is one surgical treatment option for the management of unstable intertrochanteric fractures in older adults by allowing early ambulation after surgery, preventing several complications caused by prolonged bed rest, and having a positive effect on gait restoration567). Since fixation failure of the greater trochanteric fragment, the attachment site for the abductor muscles, may cause pain, limping and dislocation of the hip, a variety of fixation methods have been introduced to obtain solid fixation of bone fragments89101112). However, studies on the classification of greater trochanter (GT) fractures and fixation methods according to the type of GT fracture have been rarely performed. Here, we report a difference in the stability of the greater trochanteric fragment depending on the GT fracture types in our previous study13). For this reason, we hypothesized that bone fragments could be successfully fixed by choosing an appropriate fixation method according to fragment stability, and secondary surgery could be avoided by minimizing the risk of irritation in plate fixation. We aimed to investigate the success rate of fixation by altering fixation methods according to GT fracture types classified based on the fracture sites and the direction of the fracture.
Go to : 
MATERIALS AND METHODS
Of 73 patients who underwent cementless bipolar hemiarthroplasty for the management of unstable intertrochanteric fractures rated AO/OTA type A2 or higher from January 2015 to November 2017 among patients aged over 65 years, a total of 44 patients were included in the study. Twenty-nine patients were excluded because they could not be followed-up for more than 6 months (n=15) and because they died during follow-up (n=14). Thirty-two and 12 patients were females and male, respectively, and the mean age was 81.3±6.0 years. All fractures were caused by falls and the mean BMD T-score was −3.6.
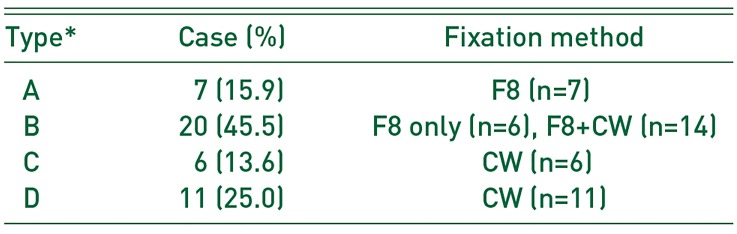
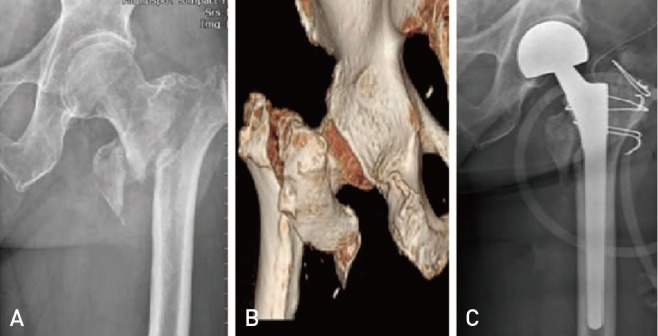
All operations were performed in a lateral position through a posterolateral approach by a single surgeon. Cementless femoral stems (Wagner SL revision Hip system®; Zimmer, Warsaw, IN, USA) were used. GT fractures were classified into four types according to the site and direction of the fracture. Type A is a transverse fracture located above the inferior border of the GT and the fracture fragment tends to be displaced superiorly by the pulling force of the hip abductors attached to the fragment. Type B is defined as a vertical fracture that is extended above the inferior border of GT. Type C included transverse fractures below the inferior border of the GT. Type C fractures are likely to have relatively weak displacement of fracture fragments because of the abductors proximally and vastus lateralis distally attached to the fracture fragment. Type D fractures occur vertically and extend to below to inferior border of the GT (Fig. 1). After insertion of a femoral stem and bipolar cup, reduction of the hip was performed, fixation methods of GT fracture fragment were chosen according to fracture type. Type A was fixed with figure of 8 wiring using 16-gauge wires, type B was fixed using the combination of figure of 8 wiring and cerclage wiring, and type C and D fractures were fixed with cerclage wiring alone (Table 1). Non-absorbable sutures (ethibond No. 1; Ethicon, Somerville, NJ, USA) were used to further reinforce fixation in comminuted fractures.
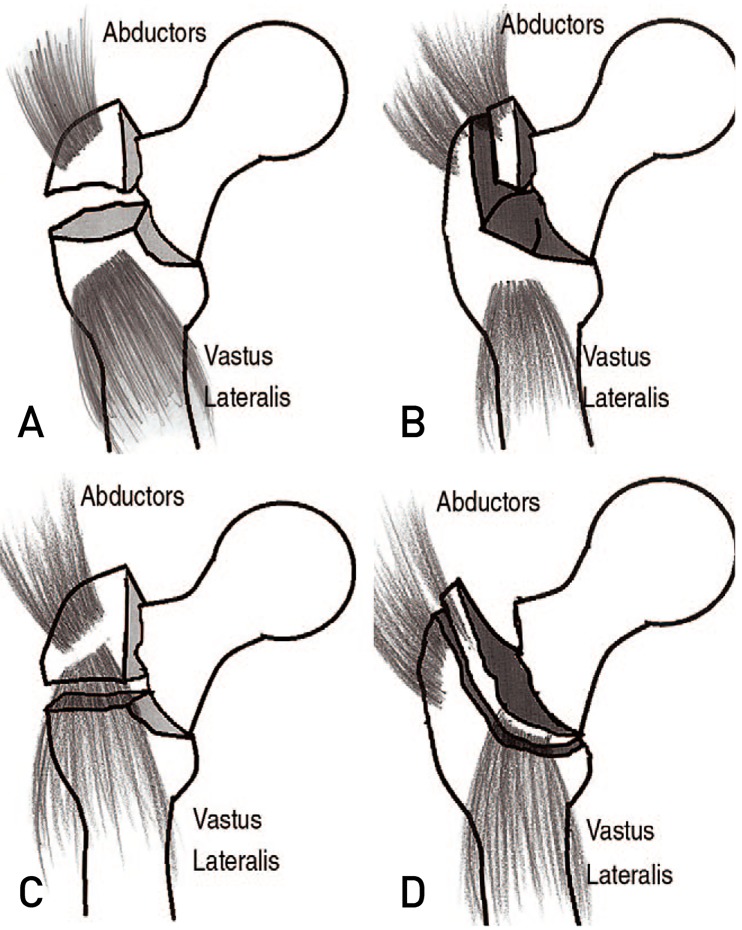 | Fig. 1Greater trochanter (GT) fracture classification. (A) Type A is a fracture with transverse direction above the inferior border of the GT. (B) Type B is a fracture with oblique direction above the inferior border of the GT. (C) Type C is a fracture with transverse direction below the inferior border of the GT. (D) Type D is a fracture with oblique direction below the inferior border of the GT.
|
Patients began ambulation using a walking aid (walker) from the 3rd postoperative day without a weight-bearing limit. Radiography was carried out before discharge and one month after discharge at one-month intervals to evaluate femoral stem subsidence and the fixation status of the greater trochanteric fragments. Fracture union was defined when fixation was well maintained without wire breakage on follow-up radiographic views. Failure of fixation was defined as a displacement of greater than 5 mm with breakage of the wire used for greater trochanteric fragment fixation. The success rate of fixation according to the fracture type of the GT was compared with the Kruskal–Wallis test. Gait ability was assessed using Clawson's Ambulation Capacity Classification14) before injury and at the final follow-up.
This study was approved by the Institutional Review Board of Kwangju Christian Hospital (KCH-2018-03-005). P-value of less than 0.05 were considered statistically significant. Statistical analysis was performed using the IBM SPSS ver.19 (IBM Corp., Armonk, NY, USA).
Go to :
RESULTS
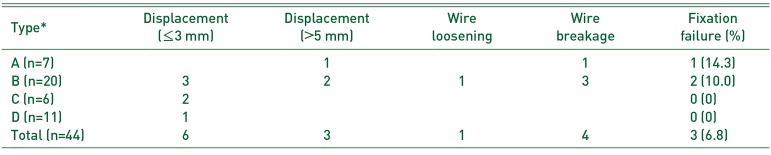
According to the AO/OTA classification, There were 7 (15.9%) type A, 20 (45.5%) type B, 6 (13.6%) type C, and 11 (25.0%) type D fractures. The success rate of fracture fixation was 85.7% (6 out of 7) in type A, 90.0% (18 out of 20) in type B, and 100% for type C (6 out of 6) and type D (11 out of 11). No statistical difference was observed in fixation success rate by fracture type (P=0.75). Wire breakage was detected in 4 cases within the first 2–3 months after surgery. Of these cases, 3 (6.8%) were defined as fixation failure due to displaced fracture fragments. Fixation failure was observed in type A (1 case) and B (2 cases), but not in type C and D (Table 2). Of these 3 cases, only one case had limping while walking.
At final follow-up, 17 (38.6%) of 44 cases had fully recovered pre-fracture gait ability. Twenty-seven cases had a decrease in walking ability, by one grade (n=15), 2 grades (n=10), and 3 grades (n=2).
Go to :
DISCUSSION
In bipolar hemiarthroplastys performed for the management of comminuted unstable intertrochanteric fractures, since non-union and displacement of the greater trochanteric fragment attached with the abductor muscles may cause pain, limping and hip dislocation, several studies have suggested using different fixation methods to manage the greater trochanteric fragment89101112). Koyama et al.15) proposed a fixation technique using a multifilament cable grip in revision hip arthroplasty after a greater trochanteric osteotomy. A cable grip can provide increased stability in the fixation of relatively large fragments, but has limited application to osteoporotic and severe comminuted fractures and is associated with high costs and postoperative irritations. On the contrary, wire fixation is a simple procedure that can minimize soft tissue injury and seems to be a more suitable method for fixation for different configurations of greater trochanteric fragments from osteoporotic intertrochanteric fractures because the shape of the wires can be customized8). Kim et al.16) reported that wiring was an effective method by achieving successful results in 80% of the patients after fixation of the greater trochanteric fragment. Suh et al.17) addressed that tension-band wiring was the optimal treatment choice after fixation of fracture fragments using figure-8, cerclage and tension-band wiring. Chin and Brick18) and Wang et al.19) also recommended that fixation of the GT fracture fragments using wires was a relatively simple and easy procedure that can minimize soft tissue injury compared to cable grip or other reattachment systems. In multifilament cable reattachment systems, cables had to be removed due to irritation. For this reason, we chose 16-gauge wires that can minimize soft tissue injury and be fixed in various methods.
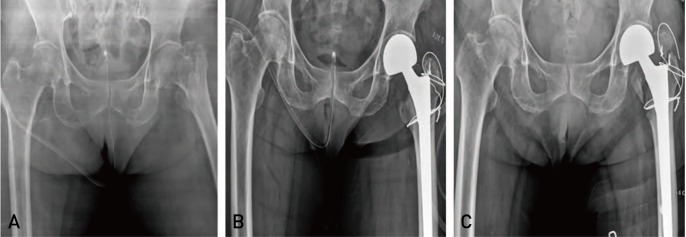
We reported that the GT fracture fragments vary in shape and can be classified as different types in bipolar hemiarthroplasty used for intertrochanteric fractures of the femur13). Although a previous study identified a difference in radiographic outcomes according to the type of fractures, the study was limited because fixation methods were not selected based on the fracture type. We realized the need for further study to investigate the surgical outcomes of different fixation methods chosen based on the classification of fracture types. Since several muscles are attached to the GT of the femur (e.g., abductors, vastus lateralis, short external rotators), we classified fractures into four types assuming that muscular action by the site and direction of the fracture determines the stability and displacement of the GT fragments. More rigid fixation was needed because the fracture fragment was more displaced upwards by the pull of the adductors in type A and B fractures (Fig. 2). On the contrary, cerclage wiring seemed to be sufficient to fix type C and D fractures because the force causing an upward displacement was relatively weak by the balanced pulling forces of the abductors proximally and vastus lateralis distally (Fig. 3). As a result of choosing a fixation method according the type of fractures using our classification system, failure occurred in only 3 out of 44 cases. This outcome demonstrates that, as we expected, the fixation method should be specifically selected based on the type of fracture fragments because of differences in fragment stability depending on the fracture type. No failure of fracture fixation occurred after cerclage wiring in type C and D fractures having relatively greater stability of fracture fragments. Even though the success rate of fixation was not statistically significantly different between type A and B and type C and D fractures, fixation failure occurred in 1 case in type A and 2 in type B (Fig. 4). We anticipate that better clinical outcomes can be expected if figure-8 wiring is performed using two single filament or multiple filament wires, instead of one single-filament wire. Patients were allowed to ambulate on the 3rd postoperative day. Wire breakage occurred at an average of two months after surgery. This was thought to be attributed to the use of a single 16-gauge wire that was unable to endure the pulling force of the abductors. There are some limitations to this study, including all operations being performed by a single surgeon, absence of a control group and the small sample size. Since hip fracture rates are increasing with a rapidly aging population, future studies with larger sample sizes are thought to be warranted to determine the optimal treatment modality for GT fragments.
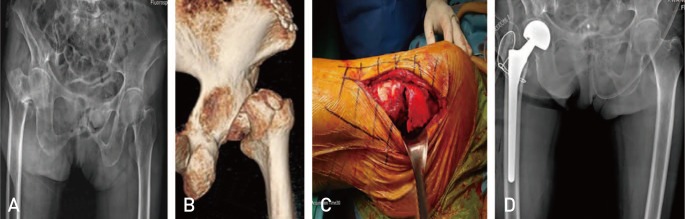 | Fig. 2(A) An 88-year-old female with an unstable intertrochanteric fracture of the right femur. Type A greater trochanter (GT) fracture was observed using computer tomography (B) and intraoperative findings (C). (D) The GT fragment was fixed using figure-8 wiring and non-absorbable suture.
|
Go to :
 XML Download
XML Download